

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
To ensure the success of revitalization procedures, it is necessary to perform adequate disinfection of the root canals through irrigation with auxiliary chemical substances and the subsequent insertion of intracanal medication with antibacterial properties [1]. The classic medication used in this procedure is triple antibiotic paste, described by Hoshino et al. [2], which consists of metronidazole, ciprofloxacin, and minocycline. Despite its effectiveness, this combination has some drawbacks, such as the possibility of tooth discoloration due to the presence of minocycline [3]. Thus, other alternatives have been suggested, such as the use of calcium hydroxide-based medications in various vehicles such as distilled water [4] or 2% chlorhexidine gel. The latter was identified as an option due to its antimicrobial properties, diffusion in dentin tubules, and low cytotoxicity (making it safe for teeth with an open apex) [3567].
To prevent recontamination of the root canal system in revitalization procedures, adequate coronal sealing must be carried out [8]. The most frequently used cement for this is mineral trioxide aggregate (MTA), as it has properties that are favorable for this procedure, such as interacting with dentin to form hydroxyapatite, which increases bond strength [910]. Despite its properties, this material has a long set time and potential for discoloration when in contact with dental structures, which limits its use in aesthetically sensitive areas [3111213]. Another material that has been tested as a coronal barrier is Biodentine (BD; Septodont, Saint-Maur-des-Fosses, France) [14], a calcium silicate-based cement, which has a short setting time and low potential for tooth discoloration [12].
The bond strength of the cements used for coronal sealing in revitalization procedures is important because materials can suffer displacement under occlusal forces, which might result in sealing failure [15]. Intracanal medication can affect dentin, with consequent impacts on bond strength [1617]. The complete removal of medications is challenging, as protocols mainly include irrigation in order to preserve the thin dentin walls [14]. Moreover, analyses of the interfacial properties of calcium silicate cements can verify the release of ions and calcium and hydroxyapatite formation, which can influence the sealing ability and bioactivity of these materials [1819]. In revitalization procedures, it is common to use intracanal medications, such as triple antibiotic paste and calcium hydroxide associated with distilled water. Thus, the aim of this study was to evaluate the effect of calcium hydroxide with 2% chlorhexidine gel as an intracanal medication on the push-out bond strength of the cement/dentin interface in canals sealed with White MTA Angelus (WMTA; Angelus Soluções Odontológicas, Londrina, PR, Brazil) and BD compared to 2 commonly used medications (triple antibiotic paste and calcium hydroxide associated with distilled water), as well as to analyze the interface with dentin. Calcium hydroxide with 2% chlorhexidine gel was chosen as an intracanal medication for analysis based on previous studies that demonstrated its effectiveness, as indicated by properties such as an extended antimicrobial effect and diffusion into dentinal tubules [3567]. Nonetheless, no previous studies have been conducted with the objective of verifying the effects of intracanal medication on the bond strength of WMTA or BD.
MATERIALS AND METHODS
Selection and preparation of specimens
This study was approved by the local Research Ethics Committee (protocol number 55036116.0) and was based on the methodology of Nagas et al. [14]. A total of 70 lower premolars with straight roots and single canals were selected. The crowns were sectioned below the cementoenamel junction using a diamond disk, and the length of all roots was approximately 15 mm.
The chemical-mechanical preparation was performed with the basic sequence of Mtwo (VDW, Munich, Germany) of up to size 25/0.06 with a length of 15 mm combined with irrigation of 2 mL of 5.25% sodium hypochlorite (Drogal, Piracicaba, SP, Brazil) between instrument changes. The final instrumentation was performed with Peeso 4 (JOTA do Brasil, Florianópolis, SC, Brazil) with a head size of 130 (1/10 mm) to create a standardized parallel canal space measuring 10 mm in length [14]. The canals were irrigated with 5 mL of 5.25% sodium hypochlorite for 5 minutes, followed by 10 mL of distilled water, 5 mL of 17% ethylenediaminetetraacetic acid (EDTA) for 5 minutes to remove the smear layer, and 10 mL of distilled water. The root canals were dried with absorbent paper points.
The specimens were randomly assigned to four groups, according to the intracanal medication that was used, as follows: group 1, calcium hydroxide P.A. (Biodynamic, Ibiporã, PR, Brazil) and 2% chlorhexidine gel (Endogel, Itapetininga, SP, Brazil); group 2, triple antibiotic paste (metronidazole [400 mg], ciprofloxacin [250 mg], and minocycline [50 mg]) in a proportion of 1:1:1; group 3, calcium hydroxide P.A. and distilled water; group 4 (control), no intracanal medication. All intracanal medications were inserted with Lentulo spirals (Maillefer Instruments, Ballaigues, Switzerland). After storing the specimens for 7 days in 100% humidity at 37°C, the medications were removed by irrigation with 5 mL of sodium hypochlorite, followed by the Mtwo size 25/0.06 and final irrigation with 10 mL of distilled water, 17% EDTA, and 10 mL of distilled water [14].
The cervical third of the specimens was sectioned, in a coronal-to-apical direction (five slices per tooth with a thickness of 1 mm) using a low-speed precision diamond saw (Isomet; Buehler, Lake Bluff, IL, USA) under water cooling [14]. Thereafter, the specimens were divided into two subgroups according to the coronal sealing material: WMTA or BD. The materials were handled according to the manufacturer's instructions, inserted into each sample with a MTA applicator (Angelus Soluções Odontológicas) and compacted with a hand plugger (Konne, Belo Horizonte, MG, Brazil) on a flat glass plate. The specimens were stored in 100% humidity at 37°C for 7 days.
Push-out bond strength test
The push-out bond strength in newtons (N) was tested in a universal testing machine (Instron 441, Canton, MA, USA) at a speed of 1 mm/min in a coronal-to-apical direction [14] until failure occurred. The bond strength was calculated in megapascals (MPa), dividing the load in N by the area of the bonded interface. The area in each section was calculated using the following formula: area = 2πrh (where π = constant value of 3.14, r = the radius of the intra-radicular space, and h = height in millimeters).
Elemental analysis at the interface
For interfacial analysis, one sample of each group was immersed in a flask containing 5 mL of Hank's Balanced Salt Solution (HBSS, Sigma-Aldrich, St. Louis, MO, USA) and stored at 37°C for 28 days. After this period, the samples were dried, desiccated, attached to aluminum stubs, and carbon-coated, followed by observation with a scanning electron microscope (JSM 5600 Lv JEOL, Tokyo, Japan); energy-dispersive spectroscopy (EDS) was carried out at the cement/dentine interface.
Statistical analysis
After exploratory data analyses and logarithmic transformation, the values of push-out bond strength were analyzed through analysis of variance (ANOVA), in a 4 × 2 factorial scheme (white MTA and BD × intracanal medications) followed by the Tukey test for multiple comparisons. The level of significance was set at 5% (α = 0.05). All analyses were performed in SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Push-out bond strength test
Table 1 shows the mean and standard deviation of the push-out bond strength values. ANOVA showed that BD yielded significantly higher values of bond strength than WMTA, regardless of the type of intracanal medication used (p < 0.05). WMTA in canals treated with calcium hydroxide and 2% chlorhexidine gel resulted in significantly higher bond strength values when compared to triple antibiotic paste associated with the same cement, but did not show statistically significant differences from canals treated with the calcium hydroxide with distilled water or the control group. For the BD group, intracanal medications did not affect the bond strength (p > 0.05).
Table 1
Push-out bond strength values of WMTA and BD with respect to intracanal medications

The values are in MPa: mean (standard deviation). Means values followed by different letters (lower vertically and horizontally uppercase) are significantly different (p ≤ 0.05).
WMTA, White MTA Angelus; BD, Biodentine.
![]()
Elemental analysis at the interface
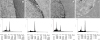
Figures 1 and 2 characterize the precipitates formed by MTA and BD in contact with dentin treated with different intracanal medications. Elemental analysis on EDS revealed that after immersion in HBSS, precipitates mainly composed of calcium, phosphorus, oxygen, silicon, and other elements were found in trace amounts. We detected high peaks of calcium for all groups, as well as small amounts of phosphorus in the groups treated with triple antibiotic paste, independently of coronal sealing. We also found this for samples of dentin without previous contact with the intracanal medication.

DISCUSSION
A coronal sealing material must adhere to root dentin and remain in place under occlusal forces to prevent leakage [1420]. The push-out test is used to evaluate the bond strength of a material to dentin; it is a widely accepted method that has been used in several studies [14161721].
Removing intracanal medications completely is a challenge in revitalization procedures [1422]. In this study, we conducted gentle manual agitation with the last instrument of the basic Mtwo sequence, along with irrigation using 5.25% sodium hypochlorite, 17% EDTA, and distilled water, to remove the intracanal medications. No known method is capable of completely removing intracanal medications from root canals, especially antibiotic pastes, even with the use of additional instruments such as passive ultrasonic irrigation, EndoActivator, EndoVac, XP-Endo, and sonic irrigation [222324]. The effects of medications on the bond strength of coronal sealing materials are critical because these cements remain in place under destructive forces, such as condensation and pressure of sealing materials, post placement, or restorative materials [14].
According to our results, BD presented significantly higher bond strength values than WMTA, regardless of the intracanal medication used (p > 0.05), which corroborates the findings of previous studies [14252627] that either used BD for sealing perforations or for coronal sealing. These results can be interpreted as resulting from small particle size and high flowability of BD, which might have improved the penetration of the material into the dentinal tubules, increasing bond strength [25]. The higher bond strength verified for BD is consistent with the higher calcium-to-phosphorus ratios found for this material when immersed in HBSS when compared to WMTA. This finding is in accordance with similar studies that showed greater calcium and silicon incorporation by BD than by MTA, indicating its bioactivity [1019]. Hence, assessments of biomineralization ability can be considered an important method for evaluating the sealing and dentin bonding properties of reparative cements [9102128]. We found that bond strength increased when calcium silicate-based cements were stored in synthetic body fluids, such as HBSS. This solution leads to the biomineralization of these materials (i.e., a tendency to form hydroxyapatite), which can increase bond strength at the dentin/cement interface [921]. The growth of crystals within the dentin tubules may enhance micromechanical retention [18]. The high calcium content detected at the BD interface might have contributed to its higher push-out values [10141927]. Further investigations should confirm the composition of precipitates at the interface, and in particular assess whether the precipitates are formed of hydroxyapatite or amorphous calcium phosphate, as bioactivity is more precisely evaluated in vivo than through indirect ex vivo analyses [28].
In push-out testing, the intracanal medications did not affect the bond strength of WMTA or BD, except for the triple antibiotic paste in combination with WMTA. On the EDS plots, we detected small amounts of phosphorus ions in the groups in contact with triple antibiotic paste. This medication may have interfered with precipitate formation at the interface, affecting the biomineralization of WMTA and BD. According to Nagas et al. [14], calcium hydroxide–based intracanal medications yielded better results in terms of bond strength. However, in our study, despite the higher values of these medications in BD groups, this difference was not significant when compared to the control group.
We observed that calcium hydroxide with 2% chlorhexidine gel did not influence the bond strength values for either material analyzed for coronal sealing, indicating that it is possible to use it safely with regard to its possible impact on coronal sealing in teeth undergoing revitalization procedures. Some studies have analyzed the effects of 2% chlorhexidine gel on bond strength, concluding that this substance yielded higher values than calcium hydroxide and Metapex when MTA Fillapex was used as a filling material [29], although it did not change the bond strength of fiberglass posts cemented with resin cement [30].
 XML Download
XML Download