

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The major goals of root canal treatment are to treat the infection and to preserve the health and functionality of the tooth. Although the survival rate of initial root canal treatment is higher than 90% [12], endodontically treated teeth can be extracted for various reasons, such as non-restorable caries, periodontal disease, procedural errors during endodontic treatment, prosthetic reasons, and vertical root fractures (VRFs) [34]. VRFs are one of the most common reasons for extraction of an endodontically treated tooth [3]. The prevalence of VRFs was reported to be 11%–20% in extracted endodontically treated teeth [4]. Excessive loss of tooth structure is associated with an increased risk of VRF, which often results from caries or trauma, access cavity preparation, and root canal instrumentation [56].
To date, many studies have evaluated the effects of various treatment protocols and applications, including root canal obturation with different filling materials and the application of different post-endodontic restorations, on the fracture strength of endodontically treated teeth [78]. However, divergent conclusions have been reported regarding the effect of such procedures on the fracture strength of endodontically treated teeth, potentially due to methodological differences among the studies. The applied parameters of in vitro fracture tests, such as the diameter and direction of the plunger and simulation of the periodontal ligament (PDL), vary among studies. Although in vitro studies provide a platform to create, compare, and check materials or techniques prior to their clinical application, the majority of them lack consistency. According to recent reviews, standardization of in vitro studies would promote quality and transparency in the reported results [910].
Finite element analysis (FEA) is an engineering method that is used to determine the stress distribution when a force is applied to a structure by the numerical analysis of complex structures based on their material properties. In this framework, the von Mises stress criterion is generally used to interpret the results. von Mises stress is a measure that accounts for various stress components, including tensile, compressive, and shear stresses, alone or in combination. von Mises stresses depend on the entire stress field and are widely used as an indicator of the possibility that damage will occur [11]. Furthermore, the factors that affect fracture susceptibility can be determined using FEA [1213]. Therefore, the aim of this study was to use FEA to evaluate the effects of variation in the test parameters used in fracture strength analysis, such as the diameter and direction of the plunger and simulation of the PDL, on the stress distribution in an endodontically treated mandibular premolar. The null hypothesis of this study was that applying different test parameters during fracture strength analysis would not affect the stress patterns or concentrations.
MATERIALS AND METHODS
Three-dimensional (3D) FEA was conducted using the SolidWorks 2007 9.0.3 structural analysis program (SolidWorks Corp., Waltham, MA, USA), as in a previous study [14]. Briefly, the CosmosWorks Program (SolidWorks Corp.) was used to perform linear elastic FEA. The sequentially performed procedures are shown in Figure 1. A 3D FEA mathematical model simulating a mandibular premolar tooth with supporting tissues was created. The average anatomic dimensions of the alveolar bone and PDL were generated according to data in the literature [15]. The geometry used for the tooth model was described previously [16]. Accordingly, a model of a tooth obturated with gutta-percha was created. Composite resin fillings were then added to this model. The geometric models were meshed with tetrahedral quadratic elements, and each model consisted of approximately 275,000 nodes and 180,000 tetrahedral solid elements. The exterior nodes of the models' bone structures were fixed in all directions as the boundary condition. The materials used in the study were assumed to be homogenous and isotropic. The properties of the structures and materials are summarized in Table 1 [1718192021]. Acrylic resin and elastomeric material (data provided from the SolidWorks Material Library) were used to simulate the alveolar bone and PDL, respectively, in order to represent in vitro test conditions. Access cavities in the models were assumed to be filled using composite resin. Eight finite element models were created in the present study (Table 2). To calculate the stress distribution, a 300-N static load was applied vertically or at a 135° angle to the central fossa. The results are presented in terms of von Mises stresses. To better visualize mechanical phenomena in the models, calculated numeric data were transformed into color graphics. Sections obtained from the 3D models were used to present the stress distribution, and the color scale was limited to between 0 and 0.5+ MPa.
 | Figure 1A schematic overview of the endodontically treated mandibular premolar tooth model.AR, acrylic resin; CR, composite resin; D, dentin; E, enamel; EM, elastomeric material; GP, gutta-percha.
|

RESULTS
Table 2 summarizes the maximum von Mises stress values (MPa). Figures 2 and 3 show the stress distributions that occurred within the test models. The diameter of the plunger affected the stress distribution within the crown, but it had no effect on the stress distribution within the root. The smaller plunger increased stresses at the contact area of the crown (Figures 2A, 2B, 3A and 3B). The direction of the plunger affected the stress distribution in both the crown and root regions. When the plunger was directed angularly, higher stresses occurred at the buccal cusp of the crown and within the root (Figures 2B, 2D, 3B and 3D). However, when the direction of the plunger was vertical to the long axis of the tooth, stress accumulation was localized at the center of the crown, and no significant stress accumulation was observed within the root (Figures 2A, 2C, 3A, and 3C). The simulation of the PDL affected the stress distribution within the root and caused higher stress accumulation in the cervical region of the root when an angular force was applied (Figure 2).
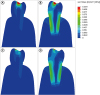 | Figure 2The von Mises stress distribution of models with periodontal ligament simulation. (A) Vertical direction and plunger diameter of 3 mm; (B) angular direction and plunger diameter of 3 mm; (C) vertical direction and plunger diameter of 6 mm; and (D) angular direction and plunger diameter of 6 mm. The blue to red colors represent low to high stress values, respectively.
|
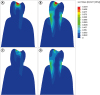 | Figure 3The von Mises stress distribution of models without periodontal ligament simulation. (A) Vertical direction and plunger diameter of 3 mm; (B) angular direction and plunger diameter of 3 mm; (C) vertical direction and plunger diameter of 6 mm; and (D) angular direction and plunger diameter of 6 mm. The blue to red colors represent low to high stress values, respectively.
|
DISCUSSION
The effects of several parameters of fracture strength test on stress distribution in endodontically treated teeth were evaluated in the present study. FEA was chosen as a methodology, because it would be difficult to test the present hypothesis using an in vitro fracture strength test due to the difficulties in standardizing the age, dimensions, mineral content, and root canal anatomy of extracted teeth. Root fractures generally occur in areas of high stress concentration when a load is applied to the teeth during mastication [22]. FEA provides a qualitative and comparative methodology for evaluating stress distribution and accumulation in tooth structures, and enables many factors to be kept uniform during the analysis, unlike in vitro tests [23]. According to previous studies, FEA models correlated very well with the observed fracture pattern in fracture strength tests, demonstrating reliable predictability for VRF [2324]. In the present study, a mandibular premolar tooth model was used, as mandibular premolars have been reported to be susceptible to fracture [25] and have been commonly used for fracture strength analysis in previous studies [78].
The effect of PDL simulation during the fracture strength test was evaluated, in light of the discordant findings reported in previous studies. Soares et al. [26] reported that the root embedment method and PDL simulation had significant effects on the fracture resistance values of extracted teeth. In contrast, Marchionatti et al. [27] reported that simulation of the PDL did not affect fracture resistance. The divergent findings in previous research might be related to the inherent limitations of fracture strength testing, such as the use of extracted teeth. In the present study, the distribution and accumulation of stresses were affected by PDL simulation. Interestingly, simulation of the PDL caused increased stress accumulation, especially in the cervical region of the root, which has been reported to be one of the most vulnerable areas for the propagation of VRFs [28]. According to González-Lluch et al. [29], more accurate results could be obtained by simulating the PDL.
The diameter of the plunger is another parameter with inconsistent results in in vitro fracture strength studies [78]. In the present FEA results, the maximum stress concentrations exhibited changes at the contact area of the crown, but did not change within the root, when different plungers were used. Therefore, the diameter of the plunger does not seem to be a distinctive factor when evaluating the fracture strength of roots in in vitro studies. In contrast, the direction of the plunger affected the distribution and accumulation of stresses in both the crown and root regions, similar to a previous study [30]. An angular direction resulted in increased stresses within the root, while a vertical direction caused no significant stress accumulation within the root. Considering the direction of mastication forces, applying an angular direction during a fracture strength test may represent the clinical situation more realistically.
Although FEA is a useful and multifunctional technique, it has some limitations. The precise and accurate simulation of the structure of teeth remains a challenge for FEA. Furthermore, in the most FEA experiments, it is assumed that the distribution of forces on the canal surface is uniform. However, this seldom occurs clinically [11]. Belli et al. [14] and Eraslan et al. [31] used the elastic properties of cortical/cancellous bone and PDL in their FEA studies. Belli et al. [14] reported that the maximum von Mises stress value observed in a composite resin–restored, root canal–treated model was 25.90 MPa, while Eraslan et al. [31] reported this value as 21.20 MPa. These values are higher than those obtained in the present study. Using the elastic properties of acrylic resin and elastomeric material in the current model could be another limitation of this study, as those materials do not exactly simulate clinical circumstances. However, the aim of this study was to explore the effects of variation in several parameters on the results of in vitro fracture strength studies. Therefore, the elastic values of acrylic resin and elastomeric material were preferred to ensure similarity to previous FEA studies [2932]. In this regard, the present findings may be useful for comparison with the results of previous in vitro fracture resistance studies.
CONCLUSIONS
Within the limitations of the present study, the null hypothesis was rejected, and it can be concluded that the direction of the plunger and simulation of the PDL during fracture strength testing affected the distribution and accumulation of stresses within the root. Simulation of the PDL and applying angular forces instead of vertical forces can be recommended for future studies, considering the conditions of the intraoral environment. Standardization of these parameters would allow a more reliable comparison of the results obtained from various in vitro studies.
 XML Download
XML Download