

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Fracture–dislocation of the proximal interphalangeal (PIP) joint is a common yet challenging hand injury;1) the fracture fragments are very small, making fixation difficult.2) Several treatment options for acute fracture–dislocation have been introduced. Conservative treatment includes immobilization using an extension blocking splint or buddy taping and surgical fixation using a Kirschner wire,3) dynamic external fixators,45) mini cannulated screws,6) or a miniplate,7) with no treatment being superior to the others. Treatment becomes significantly more difficult when the soft tissues, which usually start to heal in 7 to 10 days after the injury, obstruct fracture reduction.8) Therefore, fracture–dislocation of the PIP joint is often neglected, and patients would present with such conditions at a later stage in outpatient clinics. In chronic or neglected cases, the treatment is more challenging due to joint stiffness and partial union or malunion. Although some authors reported success with open reduction and internal fixation9) or the use of a dynamic external fixator,1) it is not uncommon for surgeons to resort to salvage surgery such as arthroplasty,1011) arthrodesis,12) or joint transplantation.13)
Yabe14) demonstrated the surgical technique of transosseous wire fixation for late-presenting fracture–dislocation of the PIP joint. We modified the transosseous wiring method by combining it with prior extension block pinning. This combination approach allows for better removal of the fibrous tissue surrounding the old fracture site with the fracture site open, and it is cost-effective because it does not require an expensive implant. Therefore, the purpose of this study is to introduce the modified transosseous wiring technique and evaluate clinical and radiologic outcomes of the technique for the management of chronic fracture–dislocation of the PIP joint.
METHODS
After receiving approval of Kyungpook National University Hospital Institutional Review Board (IRB No. 2016-11-013), which waived the informed consents from the patients, we retrospectively reviewed the records of 10 consecutive patients who underwent surgical treatment with transosseous wiring for neglected fracture–dislocation of the PIP joint between April 2003 and October 2013. We considered fracture–dislocation was neglected when the patient presented at least 3 weeks after the initial injury. There were nine men and one woman with a mean age of 38.3 years (range, 21 to 69 years). The mean time from injury to operation was 14.7 weeks (range, 3 to 66 weeks). Other demographic data are shown in Table 1. All cases involved dorsal dislocation.
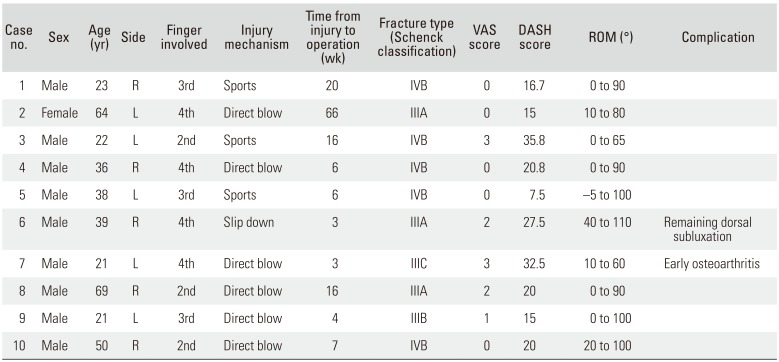
Table 1
Patient Demographics
![]()
We excluded any patients with an open fracture or neurovascular injury. Patients with fixed arthritic changes were also excluded. Each fracture was classified according to Schenck classification,15) which considers both the articular side involvement and the degree of dorsal dislocation. Fracture grade was categorized as type I when the fracture was less than 10% of the surface, type II when it was 11%–20%, type III when it was 21%–40%, and type IV when it was greater than 40%. Dorsal dislocation was classified as grade A when it was less than 25%, grade B when it was 25%–50%, grade C when it was greater than 50%, and grade D when it was full.
Surgical Technique
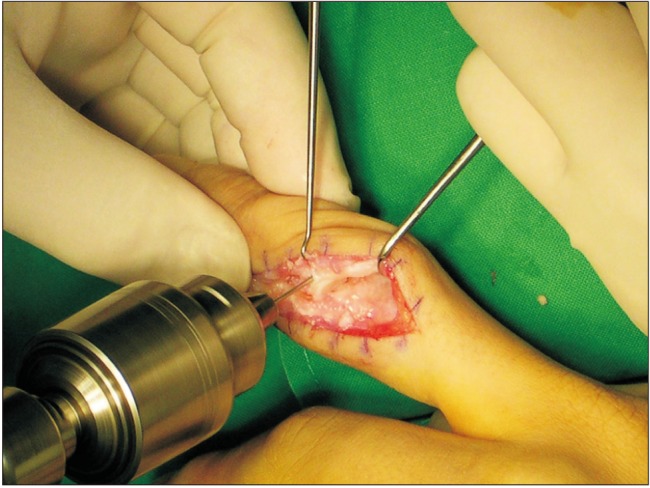
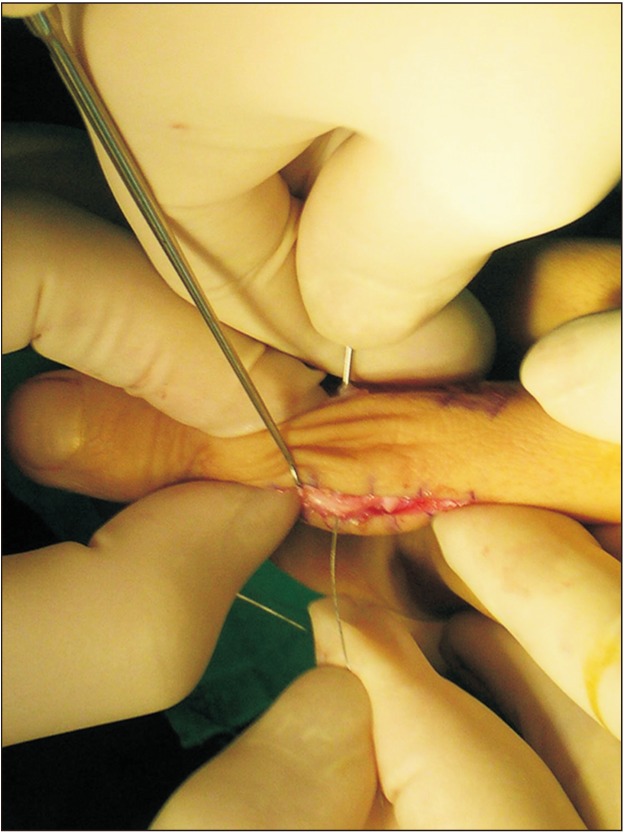
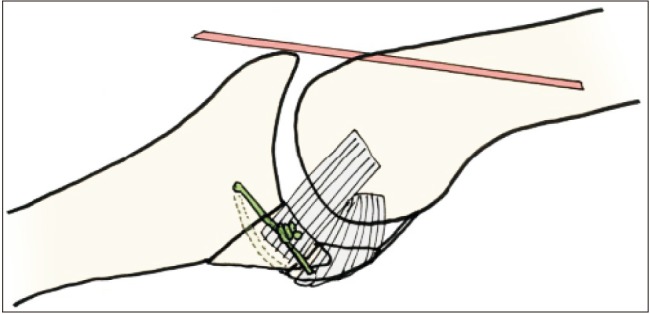
Dorsolateral skin incisions around the PIP joint were used. The extensor hood was retracted from the lateral to the medial side of the PIP joint to expose the fracture site. The extensor hood was incised as necessary. The dorsal capsule was usually hypertrophied and dorsal dislocation of the middle phalanx was observed. The hypertrophied tissue of the dorsal space was debrided. If exposure was not sufficient, we added dorsomedial approach. The volar plate and the collateral ligament were typically intact. The fibrotic tissue between the fracture fragments was thoroughly removed using a rongeur and a curette (Fig. 1). When the fracture was malunited, an osteotome was used to separate the fragments (Fig. 2). To correct the dorsal subluxation of the middle phalanx, a 1.1-mm Kirschner wire was inserted into the proximal phalanx head as an extension block in all patients except two, who underwent surgery in the relatively early period. After reduction of the dislocation, a lateral view was obtained by fluoroscopy. A bone tunnel for the metal wires parallel to the joint surface was made by drilling a 0.9-mm Kirschner wire into the base of the proximal phalanx (Fig. 3). The volar fracture fragment was reduced using a small periosteum elevator or forceps. A 25-gauge wire was passed through the bone tunnel in the proximal phalangeal base (Fig. 4) and tightened and twisted to ensure that it purchased the anterior part of the volar small fragment. The volar plate can be punctured; however, the volar fragment itself should not be punctured by the wire to avoid further damage (Fig. 5). If the fragment was large enough, two transosseous wires were used. The reduction status was checked using fluoroscopy. After range of motion (ROM) of the PIP joint was ensured, the soft tissue envelope was repaired in a layered fashion.
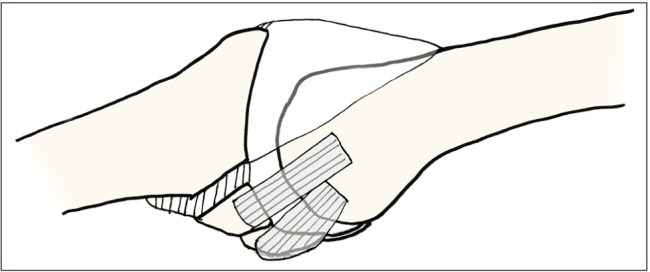 | Fig. 1The drawing shows a dorsally dislocated fracture with scar tissue in the dorsal dead space and the malunited site. The scar tissues should be debrided in such cases.
|
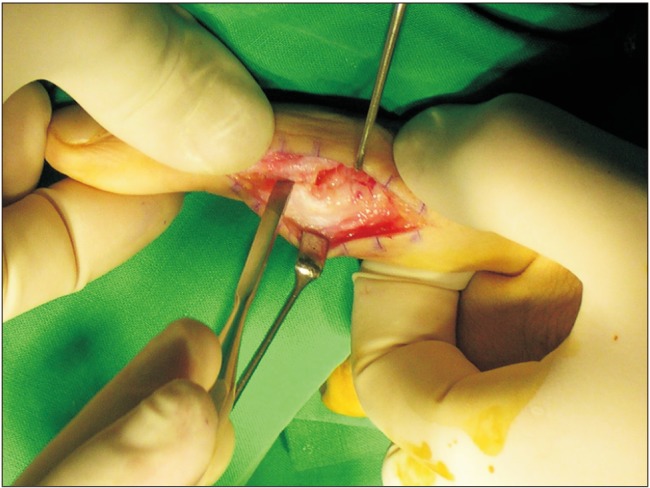 | Fig. 2Intraoperative photograph of a 36-year-old male patient. The fracture site was exposed through the dorsolateral incision. The malunited fracture was osteotomized by using an osteotome. The collateral ligament was intact from the volar fragment of the middle phalanx.
|
Postoperative Rehabilitation
Immediately after surgery, the finger was protected with a volar aluminum splint with the PIP joint in a neutral position, leaving the distal interphalangeal joint free. If the patient underwent an extension block with Kirschner wires, the wires were removed after a mean of 29 days (range, 24 to 35 days). Active ROM exercises were started immediately after removal of the extension block or 1 month after the operation.
Evaluations
Radiological evaluations were conducted using anteroposterior, lateral, and oblique views on simple radiographs. They were taken immediately after surgery, 2 weeks after surgery, and 1, 2, 6, and 12 months after surgery until bone union was achieved. Bone union and arthritic change of the PIP joints were investigated. Bone union was defined as bridging trabeculae and the absence of a radiolucent line at the fracture gap.
Clinical evaluations include measurement of active ROM of the PIP joint and pain by using visual analog scale (VAS) scores. ROM was measured using a goniometer by another surgeon who did not perform the surgery. Finally, Disabilities of the Arm, Shoulder and Hand (DASH) score at the final follow-up was measured in all patients.
Go to : 
RESULTS
The mean follow-up period was 12.9 months (range, 12 to 19 months). All patients demonstrated evidence of radiographic healing within an average healing time of 6 weeks (range, 4 to 10 weeks) (Fig. 6). However, in two cases of early loosening, the fractures healed with a widened fracture gap. Of these two patients, one showed dorsal subluxation at the final follow-up, while another patient showed an early arthritic change 1 month after surgery. Both patients refused further surgery due to the unsatisfactory results and fear of not achieving good results even after a second surgery.
 | Fig. 6(A) The lateral radiograph of a 21-year-old man who was injured by a direct blow 3 weeks before presentation shows a Schenck type IIIC fracture–dislocation of the third proximal interphalangeal joint. (B) The postoperative radiograph shows a fracture–dislocation that was reduced by transosseous wiring that purchased the volar fragment with an extension blocking Kirschner wire in the proximal phalanx. (C) One year after surgery, the wire was removed. The radiograph shows a normal joint space with bony union.
|
The mean ROM of the PIP joint was 81° (range, 50° to 105°). The mean VAS and DASH scores were 1.2 (range, 0 to 3) and 21.6 (range, 7.5 to 35.8), respectively. No cases of infection were observed. Due to implant irritation, one patient underwent removal of the transosseous wire under local anesthesia.
Go to :
DISCUSSION
Fracture–dislocation of the PIP joint is difficult to treat and often results in motion limitations, residual pain, and joint instability.16) The treatment goals include restoration of a normal articular surface, normal ROM, and motion stability, joint reduction,17) and clinical pain reduction.13)
Although several treatment options such as extension block pinning,18) closed reduction and pin fixation,19) volar miniplate and screw fixation,7) and dynamic traction20) have demonstrated satisfactory results for acute fracture–dislocation of the PIP joint, few authors have reported good results for chronic fractures. Agee2122) reported that the average arc of motion was greater in acute injuries than in chronic injuries (95° vs. 70°), and several complications were observed in acute cases. The postulated causes of such poor results were fibrotic tissues between the fracture fragments, hence poorer reduction. As with other malunion fractures, several factors require consideration in the management of chronic PIP fracture–dislocation. First, curettage of the fibrotic tissues in the malunited site must be performed thoroughly. Thus, for chronic and neglected fractures, open reduction is essential. In this study, the site was thoroughly cleaned until we confirmed new vascularization. Because exposure of the malunited site is important, we recommend both dorsomedial and dorsolateral approaches when the fracture site is not accessible in one direction. Ishida and Ikuta9) also reported acceptable results in chronic cases after using open reduction and internal fixation.
Second, the fixation should be firm and accurate enough to enable early ROM exercises. Using the surgical technique described in this study, we achieved satisfactory results. Our technique was effective in restoration of normal anatomy as well as soft tissues. Reliable fixation provided by transosseous wiring was the key to the successful results. Based on our experience, we believe that transosseous wiring enables more secure bone purchase than cerclage wiring without associated slippage. Rehabilitation was started approximately 1 month after surgery, and there was no need to remove an implant. To ensure accurate reduction, removal of the fibrous tissues at the dorsal dead space is also needed. Further, subluxation should be corrected before fracture reduction as necessary.
However, not all patients obtained successful outcome. Accurate reduction of the joint surface and reasonable integrity of the chondral surfaces are essential to restoration of the joint and achievement of good results.23) In our study, one patient with a relatively longer duration (6 weeks) between the injury and the surgery had poorer outcomes according to the DASH score. We assumed that the early arthritic change in this patient was caused by the predamaged articular cartilage and the widened fracture gap. Regarding the wire loosening in two patients, we think this was due to the small number of wire twists, which resulted in an untied wire. A considerable number of wire twists is mandatory to avoid early loosening. Also, one patient with preoperative arthritic changes in the PIP joints (a 64-year-old woman) had poor ROM. When the articular cartilage is severely damaged at or before the time of injury, surgeons should consider other treatment options.
The limitations of this study include the small number of cases, retrospective design, and short follow-up for the assessment of the rate of degenerative change. Moreover, the results were not compared with those of other treatment methods in a similar patient cohort. Therefore, the validity of our findings should be further investigated in studies that include a larger number of patients and a longer observation period.
Fracture–dislocation of the PIP joint, especially the chronic one, remains a challenging condition in hand surgery. The modified transosseous wiring technique might be a clinically and radiologically reliable and cost-effective treatment alternative.
Go to :
 XML Download
XML Download