

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Distal radius fractures are one of the most common injuries of the upper extremity, with an incidence of two fractures per 1,000 person-years.12) Distal radius fractures are mainly associated with osteoporosis in elderly patients, and several studies reported satisfactory recovery after conservative treatment.34) However, unlike elderly patients, young patients who have normal bone quality suffer comminuted fractures or terribly displaced fractures as a result of high-energy trauma. Therefore, surgical treatment of distal radius fractures is commonly required in young patients.
There are various surgical techniques for distal radius fractures including percutaneous Kirschner wire pinning, screw fixation, external fixation, and internal fixation using a plate.56789) Of those, open reduction and internal fixation (ORIF) using a volar locking plate, allowing for anatomic reduction of the fractured distal radius bone, has been closely associated with better clinical outcomes and functional recovery.101112) Wright et al.13) and Williksen et al.14) reported that ORIF with a volar locking plate for distal radius fractures yielded better functional and radiological recovery. On the other hand, abnormal reduction of the fractured bone in the wrist joint has been shown to decrease grip strength and range of motion (ROM) and cause pain, instability, and impingement syndrome.151617181920)
Despite such benefits, the conventional ORIF with a volar locking plate has some limitations: it requires an incision of the pronator quadratus muscle and detachment of the periosteum of the fractured area.212223) Several authors reported complications of the conventional technique related to meticulous soft tissue handling during the procedure. Armangil et al.24) reported the loss of pronation strength and pronator durability. Furthermore, Matullo and Dennison21) suggested that extensive soft tissue stripping over the bone may cause devascularization of the fracture fragments, resulting in delayed healing. Currently, biological approaches devised to prevent these complications, such as minimally invasive plate osteosynthesis (MIPO) with limited dissection, are receiving increasing attention.25) The main advantages of MIPO include less damage to the soft tissue and preservation of periosteal circulation in the fractured bone. By preserving soft tissue and vascularity, surgeons can expect faster healing and better clinical outcomes; however, clinical implications of these theoretical benefits have been rarely demonstrated in clinical trials. Previous studies reported the comparative results of the two techniques among only a small number of subjects. Furthermore, there has been no previously reported meta-analysis yet. Therefore, the purpose of the present study was to review published studies comparing the clinical results of the two techniques for volar locking plate fixation of distal radius fractures. We conducted a meta-analysis of the efficacy of the conventional versus MIPO technique for distal radius fractures. Our hypothesis was that the two techniques would be equally effective, showing no significant difference in clinical outcomes.
METHODS
Study Selection
We used multiple comprehensive databases to search studies comparing clinical outcomes of patients who achieved osteosynthesis using the conventional or MIPO technique. This study was based on the Cochrane Review Methods, and reporting was in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement. To identify relevant studies, we used the controlled vocabulary and free text words described in Appendix 1 to search in Medline, Embase, and the Cochrane Central Register of Controlled Trials databases. We identified all relevant studies regardless of language, publication type (articles, posters, conference articles, instructional course lectures, etc.), journal title, and publication year. This search was updated in July 2017 and included reference lists of studies and any review articles identified. The reference lists of the investigated studies were scrutinized to identify possible additional publications not found in electronic or manual search. Unpublished data were not included in this study because of the risk of bias.
Eligibility Criteria
Studies were included in our study if the patients were treated with plate osteosynthesis using conventional or MIPO technique for distal radius fractures and if the studies compared clinical outcomes of patients with distal radius fractures. Only comparative studies are included in this study. However, studies that used percutaneous fixation or recommended conservative treatment were excluded. In addition, noncomparative studies (no comparison of the effect of surgical techniques), single-arm studies only describing conventional or MIPO technique, animal or in vitro studies were not included in the present study.
Data Collection and Analysis
Initially, two authors independently assessed the titles or abstracts of studies identified by the search strategy; subsequently, full papers were assessed for final inclusion. Uncertainty about study inclusion was resolved through discussion and consensus. Eligible data were independently extracted onto predefined forms devised by the authors and evaluated for accuracy. The collected information included study characteristics (author information, journal title, study design, level of evidence, and publication year), patient demographics (sex, age, number of subjects for each surgical technique [conventional or MIPO], and follow-up period) (Table 1). Clinical outcome measures included Disabilities of the Arm, Shoulder and Hand (DASH) score or Mayo score, patient satisfaction, grip strength (in percentage compared to the contralateral side) and ROM. Radiological outcome measured included volar tilt, radial inclination, and ulnar variance at final follow-up (Table 2). Data reported as the number or mean and standard deviation (SD) were compared between two groups divided according to the surgical technique.
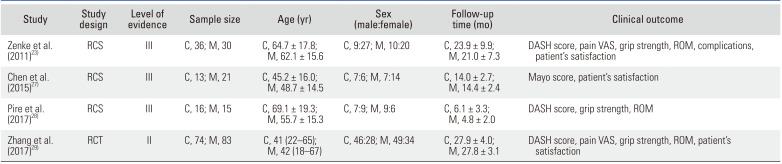
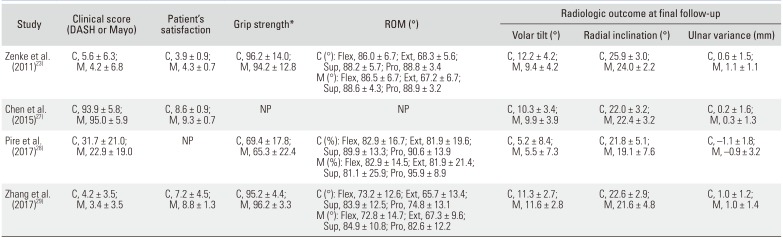
Table 1
Characteristics of the Included Studies
| Study | Study design | Level of evidence | Sample size | Age (yr) | Sex (male:female) | Follow-up time (mo) | Clinical outcome |
|---|---|---|---|---|---|---|---|
| Zenke et al. (2011)23) | RCS | III | C, 36; M, 30 | C, 64.7 ± 17.8; M, 62.1 ± 15.6 | C, 9:27; M, 10:20 | C, 23.9 ± 9.9; M, 21.0 ± 7.3 | DASH score, pain VAS, grip strength, ROM, complications, patient's satisfaction |
| Chen et al. (2015)27) | RCS | III | C, 13; M, 21 | C, 45.2 ± 16.0; M, 48.7 ± 14.5 | C, 7:6; M, 7:14 | C, 14.0 ± 2.7; M, 14.4 ± 2.4 | Mayo score, patient's satisfaction |
| Pire et al. (2017)28) | RCS | III | C, 16; M, 15 | C, 69.1 ± 19.3; M, 55.7 ± 15.3 | C, 7:9; M, 9:6 | C, 6.1 ± 3.3; M, 4.8 ± 2.0 | DASH score, grip strength, ROM |
| Zhang et al. (2017)29) | RCT | II | C, 74; M, 83 | C, 41 (22–65); M, 42 (18–67) | C, 46:28; M, 49:34 | C, 27.9 ± 4.0; M, 27.8 ± 3.1 | DASH score, pain VAS, grip strength, ROM, patient's satisfaction |
Values are presented as mean ± standard deviation or mean (range).
RCS: retrospective cohort study, RCT: randomized controlled trial, C: conventional technique, M (MIPO): minimally invasive plate osteosynthesis technique, DASH: Disabilities of the Arm, Shoulder and Hand, VAS: visual analog scale, ROM: range of motion.
![]()
Table 2
Comparison of Clinical and Radiological Outcomes between Groups in Included Studies on Conventional versus Minimally Invasive Osteosynthesis Technique
| Study | Clinical score (DASH or Mayo) | Patient's satisfaction | Grip strength* | ROM (°) | Radiologic outcome at final follow-up | ||
|---|---|---|---|---|---|---|---|
| Volar tilt (°) | Radial inclination (°) | Ulnar variance (mm) | |||||
| Zenke et al. (2011)23) | C, 5.6 ± 6.3; M, 4.2 ± 6.8 | C, 3.9 ± 0.9; M, 4.3 ± 0.7 | C, 96.2 ± 14.0; M, 94.2 ± 12.8 | C (°): Flex, 86.0 ± 6.7; Ext, 68.3 ± 5.6; Sup, 88.2 ± 5.7; Pro, 88.8 ± 3.4 | C, 12.2 ± 4.2; M, 9.4 ± 4.2 | C, 25.9 ± 3.0; M, 24.0 ± 2.2 | C, 0.6 ± 1.5; M, 1.1 ± 1.1 |
| M (°): Flex, 86.5 ± 6.7; Ext, 67.2 ± 6.7; Sup, 88.6 ± 4.3; Pro, 88.9 ± 3.2 | |||||||
| Chen et al. (2015)27) | C, 93.9 ± 5.8; M, 95.0 ± 5.9 | C, 8.6 ± 0.9; M, 9.3 ± 0.7 | NP | NP | C, 10.3 ± 3.4; M, 9.9 ± 3.9 | C, 22.0 ± 3.2; M, 22.4 ± 3.2 | C, 0.2 ± 1.6; M, 0.3 ± 1.3 |
| Pire et al. (2017)28) | C, 31.7 ± 21.0; M, 22.9 ± 19.0 | NP | C, 69.4 ± 17.8; M, 65.3 ± 22.4 | C (%): Flex, 82.9 ± 16.7; Ext, 81.9 ± 19.6; Sup, 89.9 ± 13.3; Pro, 90.6 ± 13.9 | C, 5.2 ± 8.4; M, 5.5 ± 7.3 | C, 21.8 ± 5.1; M, 19.1 ± 7.6 | C, –1.1 ± 1.8; M, –0.9 ± 3.2 |
| M (%): Flex, 82.9 ± 14.5; Ext, 81.9 ± 21.4; Sup, 81.1 ± 25.9; Pro, 95.9 ± 8.9 | |||||||
| Zhang et al. (2017)29) | C, 4.2 ± 3.5; M, 3.4 ± 3.5 | C, 7.2 ± 4.5; M, 8.8 ± 1.3 | C, 95.2 ± 4.4; M, 96.2 ± 3.3 | C (°): Flex, 73.2 ± 12.6; Ext, 65.7 ± 13.4; Sup, 83.9 ± 12.5; Pro, 74.8 ± 13.1 | C, 11.3 ± 2.7; M, 11.6 ± 2.8 | C, 22.6 ± 2.9; M, 21.6 ± 4.8 | C, 1.0 ± 1.2; M, 1.0 ± 1.4 |
| M (°): Flex, 72.8 ± 14.7; Ext, 67.3 ± 9.6; Sup, 84.9 ± 10.8; Pro, 82.6 ± 12.2 | |||||||
Values are presented as mean ± standard deviation.
DASH: Disabilities of the Arm, Shoulder and Hand, ROM: range of motion, C: conventional technique, M (MIPO): minimally invasive plate osteosynthesis technique, Flex: flexion, Ext: extension, Sup: supination, Pro: pronation, NP: not provided.
*Grip strength is indicated as a percentage of the contralateral grip.
![]()
Assessment of Methodological Quality
Two investigators independently assessed the methodological quality of each study using the Coleman methodology score,26) a 10-criteria scoring system with a final score ranging from 0 to 100. A perfect score of 100 indicates a study design that largely avoids the influence of chance, various biases, and confounding factors. Each author scored the methodological quality of the studies twice, with a 10-day interval between assessments. Any disagreement between the authors was resolved through discussion or review by a third investigator. We did not test publication bias using the funnel plot of the studies involved in this meta-analysis because the number of included studies was < 10 in each field of research.
Statistical Analysis
The main purpose of this review was to evaluate the clinical outcomes of patients with distal radius fractures after plate osteosynthesis using conventional or MIPO technique. Clinical outcomes in included studies were based mainly on DASH and Mayo scores, patient satisfaction, grip strength, ROM, and radiological outcomes (volar tilt, radial inclination, and ulnar variance) at final follow-up. To evaluate clinical outcomes, we calculated the mean ± SD of each result of the conventional and MIPO techniques and analyzed the differences in the outcome parameters between the groups. Review Manager ver. 5.3 (The Cochrane Collaboration, Oxford, UK) was used to estimate the overall pooled effect size for each outcome. A meta-analysis of the included studies was carried out using a random-effects model. For continuous outcomes, we calculated the weighted mean difference (WMD) or standard mean difference (SMD) with 95% confidence interval (CI) using the inverse variance method. Statistical heterogeneity among the studies was assessed using the I-square (I2) statistic, with values of 25%, 50%, and 75% considered low, moderate, and high, respectively, and Cochran's Q statistic (chi-square test) was used to assess heterogeneity. A p-value < 0.10 was defined as a significant degree of heterogeneity.
Go to : 
RESULTS
Identification of Studies
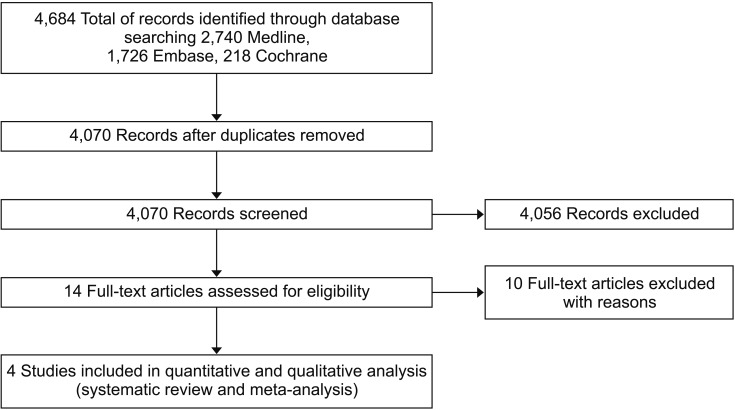
A total of 4,684 relevant articles were initially identified. Of these, 614 were duplicated in the databases. After screening the remaining 4,070 articles using titles and abstracts, all but 14 were excluded because they were not relevant to the purpose of the present study. A full-text review of the 14 articles resulted in exclusion of four articles because they lacked vital data. Finally, four studies were included for data extraction and meta-analysis (Fig. 1).23272829) As this study was a literature review, ethical approval was not obtained and the informed consent was waived.
Quality of the Included Studies
In order to evaluate the methodological quality of the studies included in our analysis, we used the modified Coleman methodology score. The mean modified Coleman methodology score of the included studies was 71.3 ± 12.1 (range, 58 to 87). The mean Coleman methodology score for each criterion is listed in Table 3.
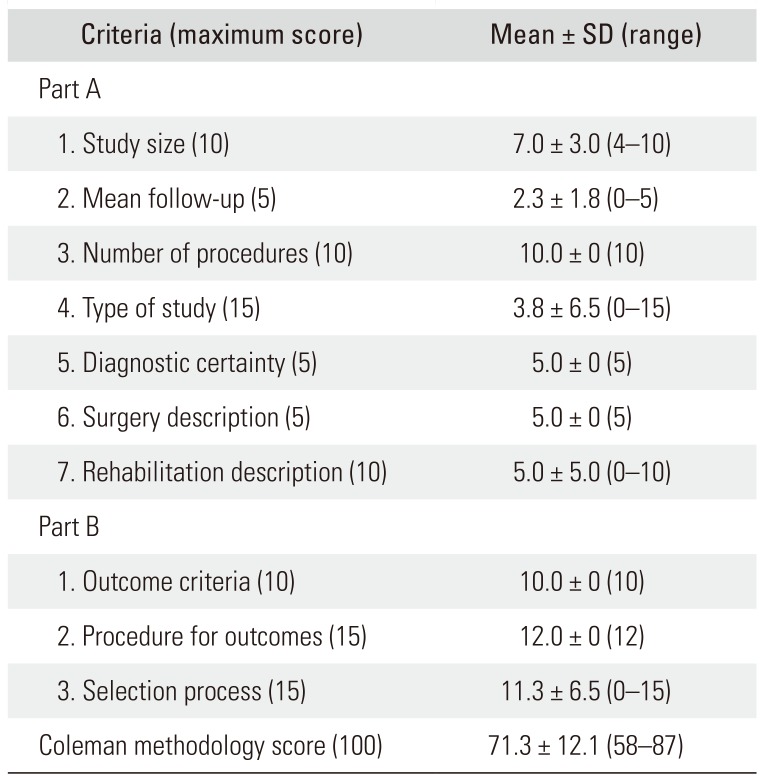
Table 3
Overall Coleman Methodology Score for Each Criterion
![]()
Clinical Outcomes
Clinical score
Four studies23272829) reported clinical scores (such as DASH and Mayo scores) at the final follow-up of 139 subjects in the conventional group and 149 subjects in the MIPO group. There were no significant differences in clinical scores between the conventional and MIPO groups (SMD, 0.20; 95% CI, −0.03 to 0.43; I2 = 0%) as shown in Fig. 2A.
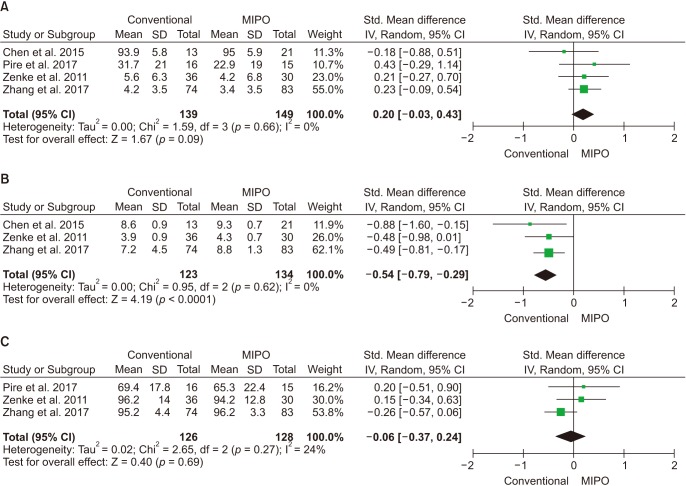 | Fig. 2Forest plots showing standard mean differences in clinical outcomes of conventional osteosynthesis and minimally invasive plate osteosynthesis (MIPO). (A) Clinical score. (B) Patient satisfaction. (C) Grip strength. SD: standard deviation, Std: standard, IV: inverse variance, CI: confidence interval, df: degrees of freedom.
|
Patient satisfaction
Three studies232729) reported patient satisfaction at final follow-up (123 subjects in the conventional group and 134 subjects in the MIPO group). There were significant differences in patient satisfaction between the conventional and MIPO groups (SMD, −0.54; 95% CI, −0.79 to −0.29; I2 = 0%). Patient satisfaction was significantly greater in the MIPO group than in the conventional group (Fig. 2B).
Range of motion
Three studies232829) reported ROM after surgery at final follow-up in the conventional and MIPO groups (126 subjects in the conventional group and 128 subjects in the MIPO group). Four parameters of ROM such as flexion, extension, supination, and pronation were evaluated. There were no significant differences in each ROM between the conventional and MIPO groups (flexion: SMD, −0.00; 95% CI, −0.25 to 0.25; I2 = 0%; extension: SMD, −0.04; 95% CI, −0.29 to 0.21; I2 = 0%; supination: SMD, −0.02; 95% CI, −0.27 to 0.22; I2 = 0%; and pronation: SMD, −0.39; 95% CI, −0.77 to 0.00; I2 = 49%) (Fig. 3).
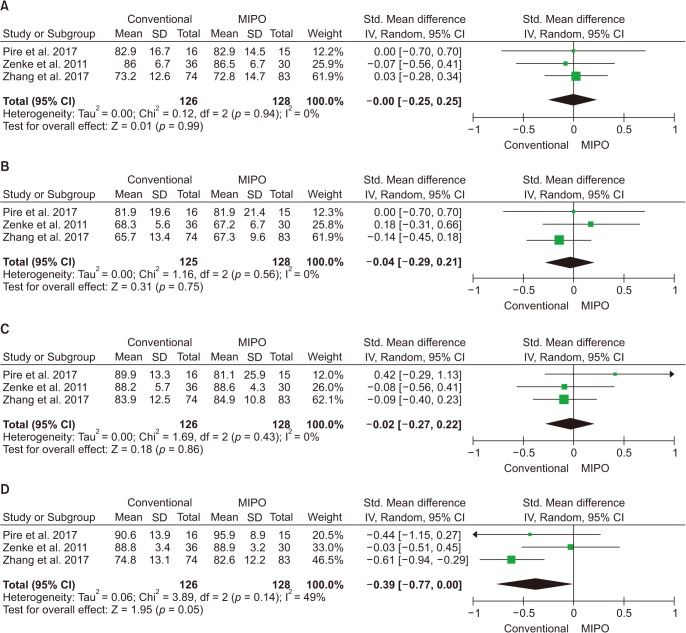 | Fig. 3Forest plots showing standard mean differences in the ranges of motions at final follow-up of conventional osteosynthesis and minimally invasive plate osteosynthesis (MIPO). (A) Flexion. (B) Extension. (C) Supination. (D) Pronation. SD: standard deviation, Std: standard, IV: inverse variance, CI: confidence interval, df: degrees of freedom.
|
Radiological Outcomes
Volar tilt, radial inclination, and ulnar variance
Four studies23272829) reported the radiological outcome at final follow-up in the conventional and MIPO groups (139 subjects in the conventional group and 149 subjects in the MIPO group). Three parameters of radiological outcome such as volar tilt, radial inclination, and ulnar variance were evaluated. Among them, radial inclination revealed a significant difference between the two groups (WMD, 1.20; 95% CI, 0.25 to 2.15; I2 = 19%). However, there were no significant differences in volar tilt and ulnar variance between the conventional and MIPO groups (volar tilt: WMD, 0.72; 95% CI, −0.99 to 2.44; I2 = 61%; ulnar variance: WMD, −0.14; 95% CI, −0.46 to 0.17; I2 = 0%) (Fig. 4).
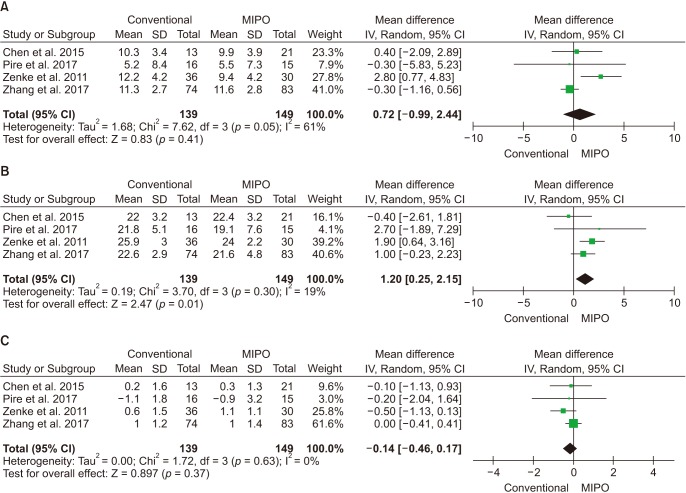 | Fig. 4Forest plots showing mean differences in radiological parameters at final follow-up of conventional and minimally invasive plate osteosynthesis (MIPO). (A) Volar tilt. (B) Radial inclination. (C) Ulnar variance. SD: standard deviation, IV: inverse variance, CI: confidence interval, df: degrees of freedom.
|
Go to :
DISCUSSION
In the present study, we assessed evidence from clinical studies that evaluated the outcomes of osteosynthesis using volar locking plates in patients with distal radius fractures, and we compared the effects of the conventional and MIPO techniques. Although there were no significant differences in clinical scores, grip strength, ROM, and radiological parameters such as volar tilt and ulnar variance, the MIPO technique was associated with more favorable patient satisfaction in the present study. Our hypothesis was supported by this meta-analysis: the two techniques were both equally effective and not significantly different in clinical outcome measures. In addition, the MIPO technique yielded more favorable patient satisfaction.
Based on the outcomes of the present study, it remains unclear which technique is superior in terms of clinical outcomes and grip strength. Conventional techniques were widely used for distal radius fractures. However, they often require meticulous soft tissue stripping such as pronator quadratus dissection and result in periosteal injury and may be associated with delayed union, nonunion, or high rates of postoperative infection.3031) To minimize soft tissue injury and damage to the vascularity of the bone, the pronator quadratus-sparing MIPO technique was suggested by several authors.323334) By preserving the pronator quadratus muscle, the authors expected some advantages such as reduced blood loss and scarring, decreased stiffness, and a lower risk of attritional rupture of postoperative flexor tendon, because the pronator quadratus muscle acts as a protective layer.303536) Grip strength of the patients was expected to be preserved as well. Despite the theoretical evidence, comparative studies analyzing the two techniques revealed no significant differences and our meta-analysis also showed no significance on comparison of the two groups. This discrepancy might be attributed to the small number of patients, different ages of the patients, and different follow-up times. Therefore, the findings of the present study should be interpreted with great caution; the data were extracted from heterogenous studies. In the future, to overcome the impact of these confounders, larger-scale randomized prospective studies that control for these independent factors need to be encouraged.
Unlike clinical outcomes and postoperative grip strength, there was significant difference in patient satisfaction between the groups, which may be associated with the small skin incision and minimal soft tissue dissection. Conventional approach entails a large longitudinal skin incision and wide dissection, which can cause tendon rupture, median nerve injury, cosmetic defects associated with a large scar, soft tissue adhesion, and longer operation time.2327) Conversely, the MIPO technique only requires a small skin incision and minimal dissection and is associated with various advantages such as preservation of periosteal blood supply, better bone union, lower infection rates, easier fracture reduction by ligamentotaxis, better aesthetic outcomes, and short operation time.2227323738) Although the association between these various risk factors and clinical outcomes has not been fully established due to insufficient data, we assumed that the major reason underlying higher patient satisfaction in the MIPO group was closely associated with cosmetic benefit and short operation time. Our meta-analysis results are consistent with those of previous studies, which also found a higher level of patient satisfaction with the MIPO technique for distal radius fractures.272829) The functional outcomes of MIPO were comparable to those of the conventional technique; therefore, the procedure can be recommended for patients with appropriate indications.
In terms of radiological parameters, our study revealed no significant differences in volar tilt or ulnar variance between the conventional and MIPO groups. Available surgical techniques are different according to the use of the conventional or MIPO approach, which increases the risk of bias. For instance, the leverage technique, which is widely used to obtain more acceptable radiological results in terms of volar tilt, can only be applied to the conventional technique because of the small incision in the MIPO technique. Although the exact frequency of the use of leverage technique was not identified due to insufficient data, there was no significant difference in volar tilt between both techniques and its clinical implication remains unclear. However, radial inclination showed a significant difference between the two groups: the mean difference was 1.2° between groups. Previous studies demonstrated the importance of anatomic reduction of distal radius fractures in terms of functional recovery.19203940) Porter and Stockley39) reported that poorly reduced fractures (> 20° of dorsal angulation and/or < 10° of radial inclination) had worse outcomes with lower grip strength. Mann et al.19) and Altissimi et al.40) suggested that residual ulnar positive variance greater than 5 mm was associated with poor clinical outcomes. In addition, loss of radial height or radial inclination is related to shifts in the center of rotation during pronation and supination, as well as increased strain on the triangular fibrocartilage complex up to 13%.15414243) However, despite the mean difference in radial inclination between the groups, all the other radiological parameters such as volar tilt, radial inclination, and ulnar variance were within the acceptable range, suggesting that both the conventional and MIPO techniques are effective in restoring the anatomy of the fractured radius, and the little radiological difference between the two techniques did not affect the clinical outcomes.
The included clinical studies evaluated the outcomes of osteosynthesis with a volar locking plate using the conventional versus MIPO techniques for distal radius fractures. Based on Coleman scales for assessment of the methodological quality, major methodological deficiencies persisted with regard to the study size and type of study. Theoretically, large-scale prospective studies provide rigorous control of potentially confounding factors. In the future, further prospective studies are warranted to address the methodological limitations. However, one of the strengths of this study is that screening and data extraction were carried out by two independent. Considering that studies comparing these two techniques for distal radius fractures are rare, the significance of this study can also be found in the fact that it provides valuable evidence supporting the use of MIPO with a volar locking plate in patients with distal radius fractures.
Despite its strengths, our study has a few limitations. First, this meta-analysis mainly included retrospective studies and only one randomized controlled trial was included for each technique. This was because only a few prospective original studies with a low risk of bias had been published previously. Second, the methodologies of the included studies were somewhat different from each other, suggesting the presence of heterogeneity. Various factors such as patients' characteristics, follow-up period, different scoring systems for evaluation, and the type of plate need to be controlled, because these factors may affect the postoperative results. Third, the characteristics of distal radius fractures were not fully considered. The minimally invasive technique in patients with distal radius fractures should be applied with more strict indications. The studies included in the meta-analysis described that extensive metadiaphyseal fractures of the distal radius is a proper indication for the MIPO technique. Thus, the results of the present study cannot be applied to all types of distal radius fractures but to limited fracture patterns. Furthermore, Chen et al.27) suggested that anatomical reduction of the articular surface is critical for treatment of intra-articular fractures; therefore, the MIPO technique is not recommended for this type of fracture. In the four included studies, characteristics of distal radius fractures were not classified strictly, which needs to be addressed in the future study. However, we only included comparative studies performed under the same protocol to minimize the risk of bias and compensate for heterogeneity and used random effects model analysis according to the Cochrane Guidelines. Furthermore, we used the SMD according to the Cochrane Collaboration Handbook to compensate for different scoring systems in each study. The SMD is used as a summary statistic in meta-analyses of studies assessing the same outcome in a variety of ways. To use the SMD, it is necessary to standardize the results of the studies before they can be combined. The SMD expresses the size of the intervention effect in each study relative to the variability observed in the study.44) In the future, large-scale randomized prospective studies that control for such independent variables and directly compare the four surgical techniques are needed.
In conclusion, based on our results, both the conventional and MIPO techniques were effective for patients with distal radius fractures. Despite limited high-quality evidence to compare osteosynthesis using a volar locking plate between the conventional and MIPO techniques, more favorable patient satisfaction was associated with the MIPO technique.
Go to :
 XML Download
XML Download