

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The two main goals of total knee arthroplasty (TKA) are to obtain a stable knee with functional improvement and to correct deformity.1) There has been much debate about which is better for achieving these goals between cruciate-retaining (CR) and posterior-stabilized (PS) TKAs.2) Each type of prosthesis has its own advantages and disadvantages (Table 1),34567) and most studies have failed to prove which type is superior to the other in terms of functional outcome, range of motion (ROM), kinematics, and long-term survival rate.289)
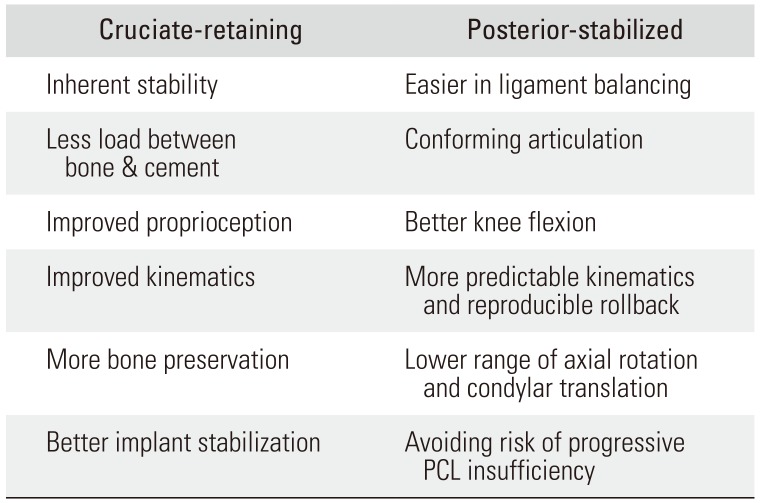
Table 1
![]()
CR and PS TKAs present not only conceptual but also technical differences, which the surgeon should be well familiar with. However, many surgeons tend to select the type of prosthesis on the basis of their own training and experience.4) Some surgeons favor the use of a specific type of prosthesis, but others select one on an ad hoc basis.10) The selection of the type of prosthesis must be based on a great store of knowledge rather than on dogmatic preconceptions or rigid preferences.4)
The topics of this review article include situations where CR TKA is difficult to perform, surgical tips for CR TKA, and the differences in surgical procedures between CR and PS TKAs. In addition, we sought to review the literature comparing clinical results, kinematics, long-term survival rate, and postoperative noise generation between CR and PS TKAs.
SITUATIONS WHERE CR TKA IS DIFFICULT TO PERFORM
Contraindications for CR TKA include posterior cruciate ligament (PCL) insufficiency, posterolateral instability, significant coronal deformity, inflammatory arthritis, and extensor mechanism deficiency.411) However, advances in implant design, surgical technique, and rehabilitation have led to an expansion of the indications for CR TKA. Archibeck et al.12) and Dennis et al.13) suggested that CR TKA would yield excellent results in rheumatoid patients with knee arthritis. Reinhardt et al.14) showed good results at minimum 2 years after CR TKA even in previously patellectomized knees.
Although the indications for CR TKA are expanding, PS TKA is generally considered easier to perform in most surgical situations without concern for obtaining appropriate tension on the PCL.15) Therefore, we would like to describe the situations that might preclude the use of CR prosthesis.
The severity of deformity should be considered before surgery. Presence of significant coronal and sagittal malalignment and possibility of difficulty in balancing often necessitate resection of the PCL.1016) A cadaveric study showed that there was significantly less change into valgus after both medial and lateral releases with retention of the PCL.17) This finding is based on the assumption that PS TKA would be more efficient for proper mediolateral (ML) balancing in the knees with severe varus or valgus deformity. Baldini et al.18) reported that CR TKA performed in patients with a coronal deformity of > 15° was associated with an increased incidence of pain and revision. In addition, PS TKA is a preferred procedure in the presence of fixed flexion contracture, especially in the knee with a fixed flexion contracture of > 20°,1019) because a symmetric flexion and extension gap is easy to obtain when the PCL is resected.
The past history should also be thoroughly examined. The history of previous operations including internal fixation of fractures around the knee, high tibial osteotomy, and unicompartmental knee arthroplasty indicates the poor quality of the remaining ligaments.20) The posterolateral corner injury would inflict great strain on the remaining PCL.4) Therefore, in patients with a past history of trauma or surgery around the knee, accurate soft tissue balancing would be easier with PS TKA.
Intraoperatively, the status of PCL should be evaluated carefully. The finding of PCL insufficiency and poor elasticity of the degenerated PCL constitutes a contrain-dication to CR TKA.20) Bone defects or the need for augments are factors that do not favor CR TKA as well.4) Patients with these conditions will not be proper candidates for CR TKA because most manufacturers do not provide a metal augment or stem for CR TKA.
Even though CR TKA is planned after consideration of these factors, there are many cases where conversion to PS TKA is intraoperatively determined for unexpected factors, which seems to be the biggest reason for many surgeons to select either a CR or PS prosthesis on an ad hoc basis during surgery. A conversion to PS TKA in what was supposed to be a CR TKA imposes a tremendous burden to the operative team and compromises surgical efficiency. Furthermore, undesirable conditions can occur when conversion is unavoidable after bone cutting. For example, a relatively greater tibial slope made for CR TKA should be decreased and a thicker polyethylene insert should be used, which may lead a limb length discrepancy. Therefore, it will be beneficial to recognize factors that may necessitate conversion from CR TKA to PS TKA.10) In our previous analysis,10) the conversion rate from CR TKA to PS TKA was high in patients with severe flexion contracture, steep posterior slope, and a small femoral component. We think those factors should also be carefully considered for appropriate selection of the prosthesis type.
Flexion contracture can be resolved by removal of osteophytes located at the posterior condyles of the distal femur and the proximal tibia, release of the posterior capsule, additional resection of the distal femur, and decrease of the slope of the tibial cut during CR TKA.202122) It seems that sustained severe flexion contracture and progression of osteoarthritis cause degenerative contracture of the posterior capsule and PCL. Conversion to PS TKA is necessary if flexion contracture and extension tightness are still present despite application of the abovementioned procedures in severe flexion contracture.21) In our analysis, the rate of conversion to PS TKA in the knees with a flexion contracture of > 20° was nearly twice higher than that in the knees with a flexion contracture of < 5° (14.3% vs. 7.8%).10)
Generally, the recommended slope of the tibial cut is less than 10° in the sagittal plane.1623) In patients with an excessive preoperative tibial posterior slope angle (PSA), resection of the bone at the posterior aspect of the tibial plateau is limited. Then, the posterior aspect of the tibial component will be placed too proximal to the original joint line; flexion gap tightness and flexion-extension gap mismatch can occur.516) Therefore, in these patients, resection of the PCL and conversion to PS TKA can be required because the resection induces more increase in the flexion gap.
In our previous study with NexGen prosthesis, the conversion rates to a PS type femoral component of size C, D, and E were 13.1%, 7.0% and 6.3%, respectively.10) The conversion rate increased with the use of smaller femoral components in the multivariate analysis (p = 0.011). We attributed these results to morphologic characteristics of the distal femur and the aspect ratio (anteroposterior/ML ratio) in Asian populations.2425) Numerous morphologic studies have demonstrated that Asians have a small and narrow width of femoral condyles.2426) Hitt et al.25) described that the prostheses did not account for the changes in the aspect ratio across the femoral condylar size and that the ML size of the contemporary femoral components tends to be too large for small knees. ML overhang can result in irritation of the soft tissue or overstuffing of the joint space and increase the incidence of femoral component downsizing.272829) In this situation, additional distal femoral cutting can be required, and it can induce the PCL sacrifice because CR TKA allows less joint line elevation compared to PS TKA.30)
Besides these factors, consideration should be given to various factors associated with the selection of CR versus PS TKA. PS TKAs can present patellar complications such as patellar crepitus or clunk due to the intercondylar box.31) Revision TKA is easy to perform with the preserved bone of femoral notch box after CR TKA. The PCL and soft tissue condition can change over the long-term follow-up. Progression of hyperextension my occur after CR TKA (Fig. 1). These various factors should be examined thoughtfully when selecting a specific type of prosthesis.
 | Fig. 1Postoperative radiographs showing insufficiency due to progressive weakening of the posterior cruciate ligament (PCL) tension. (A) One-year postoperative (right knee) and 14-year postoperative (left knee) radiographs after cruciate-retaining total knee arthroplasty (CR TKA); the sagittal angle of the CR TKA was 0.9° of flexion. (B) Three-year postoperative (right knee) and 17-year postoperative (left knee) radiographs after CR TKA. Gradual insufficiency of the PCL tension caused hyperextension of the left knee although she had no clinical instability symptoms and limited range of motion; the sagittal angle was 10.5° of hyperextension.
|
Go to : 
SURGICAL TIPS FOR CR TKA AND DIFFERENCES IN SURGICAL PROCEDURES BETWEEN CR TKA AND PS TKA
Fundamental difference between PCL retaining and sacrificing and resultant differences in flexion gap suggest that subtle but different surgical techniques should be used for each procedure (Table 2).17) We perform TKAs using a modified measured technique at our institution; the order of the procedures is femoral preparation (distal femur cutting, femoral component sizing, and anteroposterior femoral cutting), tibial preparation, and soft tissue balancing. We will describe sequential considerations according to this order.
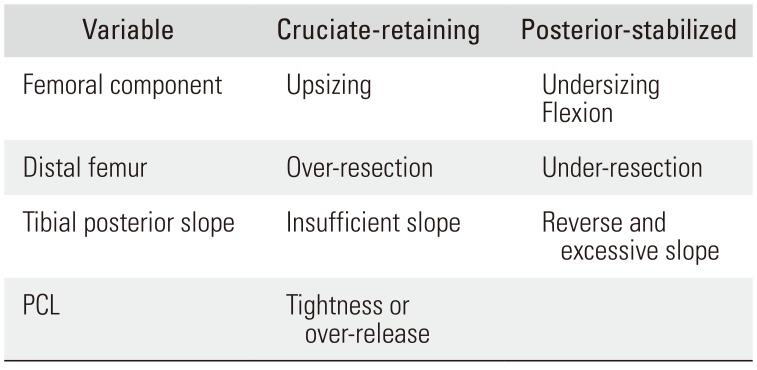
Table 2
Technical Pitfalls of Cruciate-Retaining and Posterior-Stabilized Total Knee Arthroplasty
![]()
The first intraoperative step is to evaluate the appearance and tension of the PCL after arthrotomy. If the integrity of PCL is doubtful, a switch to PS TKA is indispensable. In gross inspection, degenerative PCL with scattered bundles is considered functionally impaired. The PCL quality is also examined by pulling the ligament with a mosquito clamp. If the PCL shows firm and proper elasticity when pulled, CR TKA can be performed as planned; however, if it shows abnormal stiffness or poor elasticity, PS TKA becomes the treatment of choice from the beginning. Cadaver studies showed that sacrificing the PCL increases the flexion gap from 1.8 mm to 4.8 mm.32) For this reason, it would be better to decide the type of prosthesis before size selection and anteroposterior resection for femoral component, which influences the flexion gap.
Considering the tendency of flexion tightness that characterizes CR TKA, the surgeon should avoid over-resection of the distal femur in CR TKA for flexion and extension gap balancing (Table 2).4) Care should be taken not to cause deviation of the saw blade or cutting error intraoperatively. Surgeons are advised to select a smaller-sized femoral component in place of an intermediate size to avoid creating too much tension on the PCL, which would require release of the PCL.32) Conversely, in PS TKA where there is a greater flexion gap, a larger-sized femoral component is preferable to compensate for the flexion space created by sacrificing the PCL.32) During the posterior or posterior chamfer cut of the distal femur, iatrogenic injury of the PCL might occur because of vibration or toggling of the saw blade; this surgical error should be avoided carefully.
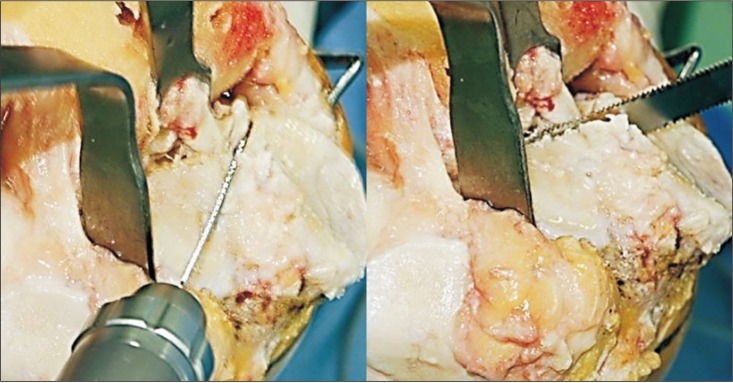
The PCL inserts distal to the articular surface of the tibia by 5 to 10 mm, and the surgeon should take care to preserve this insertion.15) Some surgeons place an osteotome or leave a small block of bone in front of the PCL insertion.432) Several studies highlighted the importance of this step; a flat tibial cut of an appropriate slope will disrupt the PCL insertion, which causes changes in anteroposterior stability.333435) We perform vertical reciprocating sawing in front of the PCL insertion site for protection during tibial resection (Fig. 2).
Okazaki et al.36) reported that the influence of changing the tibial slope by 5° on the flexion gap was approximately 2 mm with CR TKA and 1 mm with PS TKA. The adjustment of tibial slope seems to be more efficient for fine-tuning the flexion gap in CR TKA; a slight increase in the tibial slope will reduce tension on the PCL and facilitate flexion in CR TKA. However, surgeons should know that a large slope can injure the insertion of PCL at the tibia, leading to instability in flexion. In addition, the design characteristics of the implant and the inherent slope of polyethylene insert should also be considered when making PSA following the manufacturers' recommendation.16) In the majority of PS type prostheses, a small tibial PSA is recommended.2032) An increase of tibial slope would further increase the flexion gap and the risk of significant instability in flexion in PS TKA. Furthermore, a large slope in PS TKA would lead to impingement of the post-cam mechanism.32)
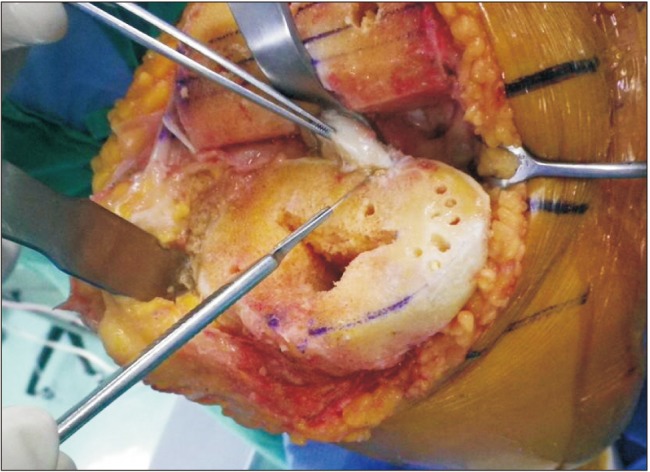
Adjustment of the PCL tension in CR TKA is for restoration of the appropriate tension (not too tight or too loose) of the retained PCL. It is important to avoid excessive flexion gap looseness as well as flexion gap tightness for acquisition of better flexion angle in CR TKA.37) If the PCL is loose, paradoxical roll-forward can occur in CR TKA.38) It has been reported that there should be some restriction on the postoperative knee flexion angle to preclude an early posterior tibiofemoral impingement.38) If flexion gap is tight due to PCL retraction or excessive tension, the PCL should be released. Before deciding whether or not to release the PCL, bone resection and component position and size should be carefully evaluated.4) We prefer PCL recession at its distal insertion due to the gradual detachment of the PCL fibers from the tibia (Fig. 3). Extreme care should be taken when recessing the PCL because it can cause intraoperative injury or postoperative insufficiency due to progressive weakening (Fig. 1).
Go to :
COMPARISON OF CLINICAL RESULTS OF CR AND PS TKA
Most studies failed to prove the difference in functional outcome of CR and PS TKAs.289) There were many prospective studies with the evidence level 1–2 to compare the CR and PS TKAs using contemporary prostheses (Table 3).39404142434445) Most studies reported no difference in clinical scores, ROM, midterm survival rate, and quadriceps muscle recovery;3940414243) two studies reported only the better ROM in PS TKAs.4445) In our preliminary prospective study using the recently introduced prosthesis of Persona (Zimmer, Warsaw, IN, USA), all the clinical results did not differ at 1 year postoperatively (Table 4).
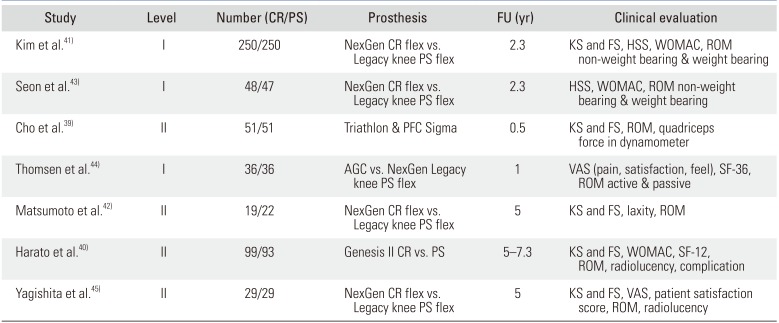
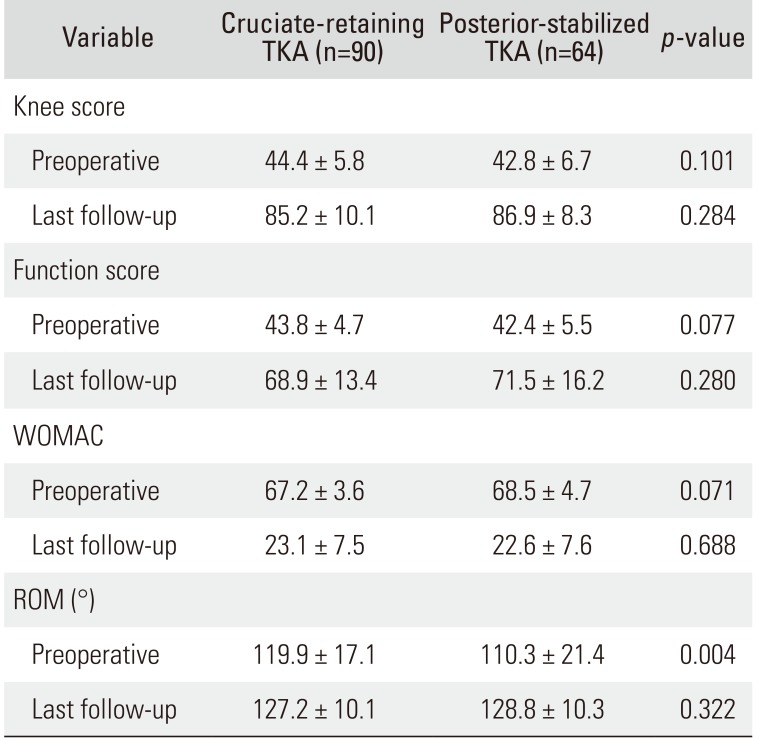
Table 3
Summary of Level 1–2 Studies Comparing the Outcomes of CR and PS Total Knee Arthroplasty
| Study | Level | Number (CR/PS) | Prosthesis | FU (yr) | Clinical evaluation |
|---|---|---|---|---|---|
| Kim et al.41) | I | 250/250 | NexGen CR flex vs. Legacy knee PS flex | 2.3 | KS and FS, HSS, WOMAC, ROM non-weight bearing & weight bearing |
| Seon et al.43) | I | 48/47 | NexGen CR flex vs. Legacy knee PS flex | 2.3 | HSS, WOMAC, ROM non-weight bearing & weight bearing |
| Cho et al.39) | II | 51/51 | Triathlon & PFC Sigma | 0.5 | KS and FS, ROM, quadriceps force in dynamometer |
| Thomsen et al.44) | I | 36/36 | AGC vs. NexGen Legacy knee PS flex | 1 | VAS (pain, satisfaction, feel), SF-36, ROM active & passive |
| Matsumoto et al.42) | II | 19/22 | NexGen CR flex vs. Legacy knee PS flex | 5 | KS and FS, laxity, ROM |
| Harato et al.40) | II | 99/93 | Genesis II CR vs. PS | 5–7.3 | KS and FS, WOMAC, SF-12, ROM, radiolucency, complication |
| Yagishita et al.45) | II | 29/29 | NexGen CR flex vs. Legacy knee PS flex | 5 | KS and FS, VAS, patient satisfaction score, ROM, radiolucency |
CR: cruciate-retaining, PS: posterior-stabilized, FU: follow-up, KS: Knee Society Knee Score, FS: Knee Society Function Score, HSS: Hospital for Special Surgery score, WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index, ROM: range of motion, VAS: visual analog scale, SF-36: 36-Item Short Form Health Survey, SF-12: 12-Item Short Form Health Survey.
![]()
Table 4
Comparison of Preliminary Results of Cruciate-Retaining and Posterior-Stabilized TKAs Using Persona
Values are presented as mean ± standard deviation. The preliminary prospective study was conducted from April 2015 to June 2017. The mean follow-up period was 1 year for both groups.
TKA: total knee arthroplasty, WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index, ROM: range of motion.
![]()
There have been several studies that analyze the kinematics in CR and PS TKAs. A prospective study with bilateral paired CR and PS TKAs compared three-dimensional kinematics using a computer model fitting technique.46) In the weight bearing condition, the CR TKA showed an anterior femoral translation from 30° to 60° of flexion, but the PS TKA showed the maintenance of a constant contact point. The tendency of the anterior femoral translation of the CR TKAs also existed in the non-weight bearing situation without statistical significance; PS TKA showed posterior femoral roll back between 60° and 90° of flexion in non-weight bearing. However, recent two studies using the same evaluation technique reported that paradoxical femoral anterior translation at low flexion angles was seen in both CR and PS TKAs.4748) On in vivo kinematics of stair climbing using radiographic-based image matching techniques, CR TKA was more sagittally stable in mid-flexion.47)
Four studies compared the long-term (10–20 years) survivorship between CR and PS TKAs.18949) Two studies showed no difference,89) but the other two studies reported better survival rate in CR TKA.149) But, it seems that the use of a specific brand of prosthesis with poor locking mechanism could increase the revision of tibial component due to backside wear and loosening.50) In a previous study comparing the long-term results at our institution, there was no difference in functional outcome, ROM, and 15-year survival rate between CR and PS TKAs.10)
The first-generation PS femoral component was known to increase the risk of postoperative patellofemoral crepitus or clunk. The contemporary femoral components with patellofemoral conformity has been shown to decrease the risk of such postoperative noise.51) Nevertheless, Nam et al.52) recently reported that the likelihood of noise generation was greater in PS TKA than in CR TKA (odds ratio, 2.5; 95% confidence interval, 1.8 to 3.7; p < 0.001). It is noteworthy that patient-perceived noise generation was associated with residual symptoms, including difficulty getting in and out of a chair, limping, swelling, and stiffness compared with those who did not report noise generation after TKA in their study. The surgeon should inform the patients of the possibility of noise preoperatively, especially when performing PS TKA. In addition, it is important to make efforts to avoid surgical errors and to use modern prostheses with improved design.
Go to :
CONCLUSIONS
CT TKA may not be feasible in certain conditions; PCL insufficiency, severe deformity, and the history of previous traumas or operations should be carefully examined for appropriate selection of the prosthesis type. The surgeon should have a clear idea on the technical differences between CR and PS TKAs. The extent of distal femoral resection, selection of femoral component size, and adjustment of tibial slope are particularly crucial for successful TKA. There was no difference in clinical results, ROM, kinematics, and survival rate between CR and PS TKAs in most studies. Therefore, adherence to the surgical indications and understanding of the differences in surgical principles might be more important than the selection of the prosthesis type.
Go to :
 XML Download
XML Download