

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Femoral head osteonecrosis usually affects adults younger than 50 years and frequently leads to collapse and subsequent osteoarthritis of the hip.12) It is becoming more prevalent because of increasing use of steroids in the management of organ transplantation and adjuvant therapy for leukemia and other myelogenous diseases.345) This disease frequently necessitates total hip arthroplasty (THA).678) As alternatives to THA, several osteotomies of the proximal femur have been introduced to preserve the hip joint.91011) These techniques move the necrotic portion from the weight-bearing region to a non-weight-bearing region. Among them, transtrochanteric curved varus osteotomy (TCVO)11) and transtrochanteric rotational osteotomy (TRO)9) are well-known and popular in use.
In 1971, Nishio and Sugioka11) introduced TCVO (Fig. 1). In this procedure, a curved osteotomy is made between the greater and lesser trochanters. Then, the femoral head is rotated into a varus position. To date, five studies, four from Japan and one from Korea, have reported the results of TCVO. In these studies, the success rate ranged from 90% to 97.3%.12131415)
In 1978, Sugioka9) introduced another osteotomy, TRO (Fig. 2). In this technique, the greater trochanter is osteotomized, and the femoral head fragment is rotated anteriorly. The success rates of TRO were inconsistent ranging from 17% to 100%. While studies from Japan and Korea reported successful results,16171819) further collapse of the femoral head developed in 83% in a study from the United States.20)
The aim of this review is to provide up-to-date guides for the osteotomy of femoral head osteonecrosis.
COMPARISON BETWEEN TCVO AND TRO
There is no randomized clinical trial comparing TCVO and TRO. Thus far, only one study retrospectively compared these two osteotomies. Lee et al.15) compared 85 patients (91 hips) who were treated with TRO and 58 patients (65 hips) who were treated with TCVO. The TCVO patients had shorter operation time and less blood loss. Postoperative collapse developed in 26 TRO hips (28.6%) and seven TCVO hips (10.8%). Osteophyte developed in 34 TRO hips (37.4%) and 13 TCVO hips (20%). Fifteen TRO hips (16.5%) and seven TCVO hips (10.8%) underwent conversion THA. The survival rate at 9 years with an endpoint of radiographic collapse was 68.7% in the TRO group and 84.7% in the TCVO group. With conversion to THA as the endpoint, the survival rate was 82.2% in the TRO group and 89.2% in the TCVO group. Their comparison showed that TCVO was better than TRO in terms of operation time, the amount of blood loss, postoperative collapse, osteoarthritic change and postoperative survival.
There are several differences between the two osteotomies. In TRO, the greater trochanter should be osteotomized and the joint capsule should be circumferentially incised. Accordingly, TRO necessitates longer operation time and more bleeding. In TCVO, the head segment is simply rotated into varus by about 30° in the coronal plane. However, in TRO, the femoral head is rotated anteriorly by 60° to 90° and varization is required.
The femoral head is not perfectly spherical but elliptical. The greater axis lies horizontally; that is, the radius of curvature along the meridian is greater than the radius of curvature along the equator. In the study of Hammond and Charnley,21) the mean difference of the two radiuses was 1.7 mm. Therefore, the femoral head might become less congruous to the acetabulum after TRO than after TCVO. The mechanical simplicity and avoidance of capsulotomy in TCVO seemed to result in less osteophyte formation compared to TRO.
INDICATION OF THE OSTEOTOMY
The reported results after the osteotomies were inconsistent.12131416171820) Inappropriate patient selection is a reason for poor outcomes after the osteotomy;1620) to improve the success rate, more efficient selection of patients is mandatory. Patient's age, body mass index, the preoperative stage of the disease, the size of the necrotic portion, and remaining viable portion of the femoral head are known factors affecting the result after the osteotomy.
Patient's Age and Body Mass Index
Patient's age and body mass index are factors that affect results after the osteotomy. In a previous study,22) secondary collapse was more frequent in patients who were aged > 40 years and whose body mass index was > 24 kg/m2. After the osteotomy, an intact bone is established in the weight-bearing region of the femoral head. Secondary collapse is a stress fracture of this newly-established intact portion, which is usually thin and beak-shaped. Age-related osteopenia develops by the age of 40 years and progresses afterwards.23) In patients with high body mass index, an excessive load is applied on the femoral head, which leads to a stress fracture and secondary collapse of the newly formed weight-bearing portion.
Size of Necrotic Portion
Small lesions do not progress even without any medical or surgical intervention;26) whereas hips with a large lesion preoperatively have subsequent collapse of the femoral head after the osteotomy.27) Thus, the osteotomies should be performed in medium-size lesions with a combined necrotic angle between 190° and 240° (Fig. 3),28) or type B lesions involving the medial two-thirds or less of the weight-bearing portion according to Japanese Investigation Committee (JIC) classification (Fig. 4).29) The extent of necrotic portion should be measured on magnetic resonance imaging (MRI) for the accurate measurement of the necrotic portion.
Viable Portion of the Femoral Head
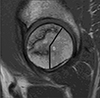
The femoral head should have a viable portion of such a size that restoration of an adequate weight-bearing articular surface is possible after the osteotomy.3031) The adequate area of viable bone for TRO is an arc of > 120° between the central vertical line of the femoral head and the posterior margin of the necrotic portion on a midsagittal MRI scan (Fig. 5), and that for TCVO is an arc of > 150° between the central vertical line of the femoral head and the lateral margin of the necrotic portion on a midcoronal MRI scan (Fig. 6).
CONCLUSIONS
We recommend the use of TCVO for the treatment of femoral head osteonecrosis in patients who have (1) hip pain, (2) age less than 40 years, (3) a body mass index less than 24 kg/m2, (4) the Ficat stage IIA or III disease, (5) a medium-size lesion (combined necrotic angle between 190° and 240° or JIC type B lesion), and (6) enough viable bone (> 150° between the central vertical line and the lateral margin of the necrotic portion on the midcoronal MRI).





 XML Download
XML Download