

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ceruminous adenoma refers to a benign subtype of ceruminoma originating from ceruminous glands, which are specialized apocrine sweat glands present in the dermis of the cartilaginous portion of the external auditory canal.1 Its occurrence among dogs and cats is relatively common, but that in the human external auditory canal it is very rare. It is known that about 150 cases have been reported worldwide so far,23 and only six cases have been reported in Korea.4567 Due to such rare occurrence, the diagnostic criteria and the extent of excision required for the cure have not yet been clearly established. The authors recently treated a 55-year-old female patient who was diagnosed with ceruminous adenoma after coming to the hospital with a mass of the external auditory canal as a chief complaint. Therefore, we report this case in combination with a review of the literature.
CASE
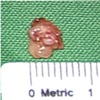
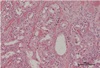
A 55-year-old female patient came in with otorrhea and ear fullness of the right ear as chief complaints. The patient did not present accompanying symptoms such as ear ache, changes in hearing, tinnitus, dizziness or anything else. She had no special medical, surgical and trauma histories. In the otoscopic examination, a mass with a smooth surface that originated from the antero-superior portion of the right external auditory canal and filled it was found along with serous otorrhea near the lesion (Fig. 1). When palpitated, the mass was elastic and soft and caused no tenderness and the eardrum was not observed due to the mass. In pure tone audiometry, the patient displayed normal bilateral air-conduction hearing thresholds at 12 dB and no air-bone gap was present. In the temporal bone computed tomography scan performed to identify the origin and distribution of the mass, a lesion of about 1.1 cm and of soft tissue that displayed a shaded hue was observed on the antero-superior wall of the osteochondral junction in the right external auditory canal, accompanied by adjacent compressive bony erosion. The lesion was not markedly enhanced by contrast medium and showed heterogeneous signal intensity (Fig 2). A wide en-bloc excision was planned for the purpose of lesion removal and histologic confirmation with the suspected diagnosis being a non-osseous benign external auditory canal tumor. After general anesthesia, under surgical microscope, a transcanal approach was used to incise the marginal edge of the mass and raise the skin flap. The mass detected by the naked eye was surrounded by a capsule, so the boundary was clear between the mass and the surrounding tissues. So the planned en-bloc excision was attempted, but as the base of the mass adhered to surrounding tissues, it was removed piece by piece and the excision was performed with the capsule checked, until normal tissues were identified (Fig. 3). As no invasion to the skin covering the mass and necrosis was observed, the extra skin was removed and then the skin was returned to its original position to complete the operation. After this, the eardrum displayed normal features. The findings of the histopathologic examination revealed features of simple papillary hyperplasia of ceruminous glands and fibrosis of the surrounding tissues in hematoxylin and eosin (H & E) staining, and no cell dysplasia or cleavage was observed (Fig. 4). And the results of additional immunohistochemical staining for CK 7 and p63 were positive, based on which the patient was finally diagnosed with ceruminous adenoma (Fig. 5). The patient was discharged without further treatment after the operation, and has been monitored for 10 months after the surgery without showing any signs of recurrence of the problem (Fig. 6).
DISCUSSION
The human external auditory canal is divided into two parts: the cartilaginous external auditory canal forming the outer third of the canal and the osseous external auditory canal corresponding to the inner two thirds of the canal. The dermal layer of the cartilaginous external auditory canal includes follicles, sebaceous glands and ceruminous glands, which are specialized apocrine sweat glands and known to be almost absent in the bony part.8 Since the first report of ceruminoma by Haugh in 1894, all of the masses arising from ceruminous glands of the external auditory canal have been diagnosed as ceruminous adenoma; however, due to ambiguity about the terminology, it was excluded from the WHO diagnostic classification in 1991.9 Afterwards, as ceruminous glands were found to have the properties of apocrine glands, and not being solely composed of sweat glands, a new classification concept was established. In 1995, Mills et al. classified masses in ceruminous glands as benign and malignant. According to the classification, benign masses include ceruminous adenoma, pleomorphic adenoma and cylindroma; while malignant masses include adenoid cystic carcinoma, adenocarcinoma and mucoepidermoid carcinoma.10 In addition, subtypes such as syringocystadenoma papilliferum, eccrine cylindroma, mucoepidermoid carcinoma and others were presented; however, according to the WHO classification system, only ceruminous adenoma and ceruminous adenocarcinoma are clearly defined as masses originating from ceruminous glands and the other types are regarded as probable sub-categories.1459 Ceruminous adenoma is defined as a benign mass that arises due to the local proliferation of well-differentiated ceruminous gland tissues.19 It occurs mainly in adults but occurrence among children has been reported very occassionally,41112 and it is known that there is no significant difference in prevalence between males and females.13 There is no clinical manifestation unique to ceruminous adenoma; therefore, depending on the degree of the occlusion of the external ear canal, hearing loss, tinnitus, ear fullness and other symptoms may occur. In addition, nonspecific manifestations such as otorrhea on the pressured sites, ear ache due to secondary infection and bleeding caused by ulcer formation can appear as main symptoms.13 Ceruminous adenoma takes the form of a polypoid or papillary mass and has a smooth or necrotic surface.213 There is no feature unique to ceruminous adenoma which makes it distinctive from other masses in imaging examination.9 Its diagnosis is made by histologic examination. The tissues composed of luminal epithelial cells and basal myoepithelial cells constituting normal ceruminous glands show acinar or trabecular proliferation and in many cells, yellowish brown cytoplasmic granules are observed.23 Also, in immunohistochemical staining, luminal epithelial cells are positive for CK 7, and basal myoepithelial cells for S-100 and p63 as normal ceruminous glands, which is helpful in the identification of the cell origin and diagnosis.23913 Non-osseous masses to be distinguished from ceruminous adenoma include benign tumors such as seborrheic keratosis, neuroendocrine adenoma, pleomorphic adenoma of the parotid gland, meningioma, paraganglioma and others, as well as malignant tumors such as ceruminous adenocarcinoma, mucoepidermoid carcinoma, basal cell carcinoma, squamous cell carcinoma and so on.4 When it comes to the treatment of ceruminous adenoma, there still exist different opinions. But the first-step in treatment has been centered on wide local excision and additional anticancer and radiation treatments have not been recommended.121213 In most cases, the excision is possible through the approach to the external auditory canal. However, if a mass is large enough to cause conductive hearing loss or there is no clear boundary of the mass, a surgical procedure through posterior auricular incision is recommended because it gives a broader field of view.813 Generally, ceruminous adenoma has good prognosis, but recurrence has been reported in a small percentage of cases.13 Niemczyk et al. recommended long-term monitoring in consideration of potential recurrence and malignant alteration.12




 XML Download
XML Download