

 PDF
PDF ePub
ePub Citation
Citation Print
Print


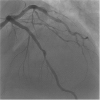
A 59-year-old man who underwent bare-metal stent implantation in the left-anterior descending artery (LAD) 15 years previously was admitted to our hospital because of stable angina pectoris. Coronary angiography revealed 75% in-stent restenosis at the proximal LAD, showing a fractional flow reserve of 0.74 at the distal LAD (Figure 1). This lesion was successfully treated using excimer laser coronary angioplasty (ELCA) and Xience Alpine® (Abbott Vascular, Santa Clara, CA, USA) stent implantation under optical frequency domain imaging (OFDI) guidance (FastView®, Terumo, Tokyo, Japan) which demonstrated a cavity due to plaque rupture with thrombi, and fibroatheroma (Figure 2A and B). We performed coronary angioscopy (Forwardlooking®, OVALIS, Osaka, Japan) pre and post-ELCA for further evaluation with direct vision. Pre-ELCA coronary angioscopy showed a cavity due to plaque rupture with thrombi, indicating the progression of in-stent neoatherosclerosis (Figure 2C). Incomplete stent coverage was confirmed at the stent's proximal segment (Figure 2D). We performed ELCA 6 times using a 1.4-mm concentric laser catheter (CVX300®, Spectranetics, Colorado Springs, CO, USA) at a pulse rate 25 Hz, and energy output 45 mL/mm2. OFDI detected the ablation of in-stent surficial fibrous plaque after ELCA (Figure 2E and F). Coronary angioscopy revealed neointimal minor bleeding, and stent strut with neointima peeled off due to ELCA (Figure 2G and H). Final coronary angiography showed optimal results (Figure 3). Post-ELCA OFDI demonstrated that ablation of superficial plaque in in-stent area. Following OFDI, coronary angioscopy demonstrated surficial minor bleeding that was unclear on OFDI. Furthermore, coronary angioscopy clearly revealed the exposed strut after ELCA. Clinical studies using ELCA for in-stent restenosis have been reported1)2); however, coronary angioscopy pre- and post-ELCA is unreported.
Shinichiro Masuda, MD1 , Takashi Shibui, MD1, Sho Nagamine, MD1, Takaaki Tsuchiyama, MD1, Takashi Ashikaga, MD, PhD2
, Takashi Shibui, MD1, Sho Nagamine, MD1, Takaaki Tsuchiyama, MD1, Takashi Ashikaga, MD, PhD2
, Takashi Shibui, MD1, Sho Nagamine, MD1, Takaaki Tsuchiyama, MD1, Takashi Ashikaga, MD, PhD2
Figures and Tables
Figure 1
Initial coronary angiography shows 75% in-stent restenosis at the proximal left anterior descending artery. White dotted lines indicate the stent segment.
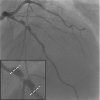
Figure 2
Optical frequency domain imaging and coronary angioscopy findings before excimer laser coronary angioplasty (A-D), and after excimer laser coronary angioplasty (E-H). (A) A cavity (red arrows) and fibroatheroma (yellow asterisks). (B) Circumferential fibrous plaque with a minimum lumen area of 2.8 mm2. (C) On angioscopy, a cavity due to plaque rupture is confirmed at the 1–2 o'clock (red arrows) position, and yellow plaque is confirmed at the 9 o'clock position (yellow asterisks). (D) Yellow arrowhead indicates stent strut. (E) On optical frequency domain imaging, ablation of the surficial plaque is confirmed (white arrows). (F) Ablation of surficial fibrous plaque is confirmed (yellow arrowhead). The minimum lumen area is 2.9 mm2. (G) On angioscopy, surficial minor bleeding is confirmed at the 9 o'clock position (yellow arrows). (H) Yellow arrowheads indicate the stent strut with neointima peeled off.

References
1. Ambrosini V, Golino L, Niccoli G, et al. The combined use of drug-eluting balloon and excimer laser for coronary artery restenosis in-stent treatment: the DERIST study. Cardiovasc Revasc Med. 2017; 18:165–168.

2. Hirose S, Ashikaga T, Hatano Y, et al. Treatment of in-stent restenosis with excimer laser coronary angioplasty: benefits over scoring balloon angioplasty alone. Lasers Med Sci. 2016; 31:1691–1696.
 XML Download
XML Download