

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Carbapenem-resistant Enterobacteriaceae (CRE) is an emerging problematic infectious agent, with reports of its prevalence worldwide.123 Invasive infections caused by CRE are associated with high mortality rates of about 40%–50%.456 Treatment of CRE infection is difficult because treatment is limited to certain antibiotics, such as colistin and tigecycline.7 CRE outbreak in hospitals has become a critical issue. Transmission by patients with CRE, as well as carriers of CRE, contribute significantly to in-hospital CRE transmission.89 Patients admitted to the intensive care unit (ICU) are at high-risk of contracting infection caused by multidrug-resistant microorganisms, and often receive empirical broad-spectrum antibiotics, including carbapenem.10 These patients have a high-risk of CRE colonization, and subsequent CRE infection.1112 Reports have indicated that patients colonized with CRE are at least twice as likely to have a CRE infection.5
The Centers for Disease Control and Prevention (CDC) have emphasized that healthcare facilities must intervene to prevent CRE transmission.9 Active surveillance culture of CRE (ASC-CRE) in high-risk units has been reported to significantly reduce nosocomial transmission of carbapenem-resistant Klebsiella pneumoniae colonization and infection.13 Active surveillance in ICUs is a highly cost-effective means of decreasing CRE infection and mortality in areas with low CRE prevalence.14 Thus, ASC-CRE is recommended in high-risk settings, such as ICUs, to prevent CRE outbreaks or invasive infections.15
In Korea, CRE was reported for the first time in 2010. Sentinel surveillance of CRE in Korea showed that the prevalence of CRE increased sharply in 2015–2016.161718 CRE infection appears not to be indigenized in Korea yet and has been managed as a nationally notifiable communicable disease since June 2017 in order to prevent its spread. In our hospital, the number of CRE isolates has increased between 2015–2016. Also, there was an outbreak of CRE infection associated with emergency ICU (EICU) use, which occurred in summer 2016. Thus, we applied preemptive contact precaution immediately after admission to the EICU, and ASC-CRE was performed by collecting rectal swabs in ICUs to identify CRE carriers and to detect CRE acquisition promptly. Whenever CRE was detected, contact precaution was applied immediately. In this study, we performed ASC-CRE to monitor CRE acquisition during ICU care and to examine potential risk factors associated with CRE acquisition.
METHODS
Study population and study design
We conducted a retrospective analysis on patients aged ≥ 18 years who were admitted to the EICU between October 15, 2016 and October 31, 2017. The study hospital is an acute care, university-affiliated and tertiary hospital with around 1,400 beds, and 8 different ICUs (emergency, medical, surgical, neurosurgical, cerebrovascular, and 3 traumatic ICUs) in the Southeastern region of Korea. Per the Ministry of Health and Welfare regulations, only patients in the emergency room can be admitted to the EICU; therefore, all patients admitted to the EICU came from home or were transferred from other hospitals or long-term care facilities. Upon admission, empirical contact precautions were applied in all patients, ASC-CRE was performed by collecting rectal swabs for culturing, and real-time polymerase chain reaction (PCR) was performed to detect carbapenemase-producing Enterobacteriaceae (Fig. 1). Rectal swab samples were collected every Monday until ICU discharge and were tested for CRE. Patients who had CRE detected by culture or by carbapenemase gene expression via PCR at the time of admission were excluded from this study (Fig. 1). The primary outcome was CRE acquisition in the ICU. The secondary outcome was in-hospital mortality.
Fig. 1
Study design for the ASC-CRE among patients admitted to the EICU in an acute care hospital in non-endemic area.
CRE = carbapenem-resistant Enterobacteriaceae, ASC-CRE = active surveillance culture of carbapenem-resistant Enterobacteriaceae, EICU = emergency intensive care unit, PCR = polymerase chain reaction.

Data collection and analysis
Demographic and clinical information was collected from electronic medical records, including age, gender, comorbidities, prior exposure to healthcare facilities within one year (history of admission, regular visit to outpatient clinic or surgery), colonization or infection with multidrug resistant organisms (MDROs) including methicillin-resistant Staphylococcus aureus, multidrug-resistant Acinetobacter baumannii (MRAB), multidrug-resistant Pseudomonas aeruginosa (MRPA), vancomycin-resistant Enterococcus, or extended-spectrum β-lactamases-producing bacteria (ESBL), comorbidities, use of medical devices (central venous catheter, ventilator, indwelling urinary catheter, or nasogastric tube) during the period at risk for CRE, exposure (≥ 1 day) to any antimicrobials in the past 30 days before the admission, ICU length of stay, hospital length of stay, and in-hospital mortality. In addition, the Acute Physiology and Chronic Health Evaluation II (APACHE II) score was calculated from clinical data for adult patients on admission, as a marker of disease severity.
Microbiological methods and definitions
ASC-CRE was performed by collecting rectal swabs according to modified protocols from the CDC.19 Each rectal swab was inoculated in 5 mL trypticase soy broth (Becton Dickinson, Heidelberg, Germany) containing a 10-μg ertapenem or meropenem disk (BIO-RAD, Hercules, CA, USA) and incubated overnight at 35°C in ambient air. The trypticase soy broth was vortexed and 100 μL was subcultured onto a MacConkey agar plate (Asan Pharmaceutical, Seoul, Korea). All lactose-fermenting colonies were identified by matrix assisted laser desorption ionization-time of flight mass spectrometry (Bruker Daltonics, Bremen, Germany). CRE colonization was defined if carbapenem non-susceptible Enterobacteriaceae was identified in rectal swab specimens. Carbapenem nonsusceptibility was confirmed when zone diameter on disk diffusion testing was < 23 mm for meropenem or < 21 mm for ertapenem by the Clinical Laboratory and Standards Institute M100-S26.20 To detect carbapenemase-producing Enterobacteriaceae, a PCR assay was performed to detect five carbapenemase genes (blaNDM, blaKPC, blaVIM, blaIMP-1, and blaOXA-48) using either real-time PCR (Xpert® Carba-R; Cepheid, Sunnyvale, CA, USA), or an in-house conventional multiplex PCR.919 Invasive CRE infection was defined as CRE isolated from normally sterile specimens or CRE isolated from any given body site except rectal swab or stool that was associated with clinical infection.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics, version 25.0 (IBM Corp., Armonk, NY, USA). All continuous variables were summarized as means and standard deviations, and categorical variables were described using frequencies and percentiles. Categorical variables were compared using Pearson's χ2 test or Fisher's exact test, whereas non-categorical variables were tested using a t-test. Multivariate analysis was performed for variables with P < 0.1 in univariate analysis. Independent risk factors of CRE acquisition were evaluated using logistic regression. The risk factors of in-hospital mortality were analyzed using Cox proportional hazard regression. All results were considered significant at P < 0.05.
Ethics statement
All patients admitted to the EICU received informed consents for ASC-CRE according to the hospital infection control policy. The present study protocol was reviewed and approved by the Institutional Review Board (IRB) of Pusan National University Hospital (IRB No. 1802-005-063), and the requirement for obtaining informed consent was waived because of the study's retrospective design.
RESULTS
During the study period of 12.5 months, a total of 909 patients were admitted to the EICU, and 840 patients underwent ASC-CRE testing. Specimens from the other 69 patients could not be collected because of death or early transfer. In total, 810 patients met the inclusion criteria and they contributed 4,838 person-days in EICU (Table 1). Thirty patients were excluded; 23 patients had positive CRE culture or carbapenemase-positive PCR at admission, and 7 patients were aged < 18 years (Fig. 1). The median age of the patients was 66 years (range, 18–105), and 499 (61.6%) patients were men. In total, 131 (16.1%) patients had cardiovascular disease, and 252 (31.1%) had diabetes (Table 2). Overall, the CRE acquisition rate was 2.6% (Table 1). The incidence of CRE acquisition in the ICU was 4.3/1,000 person-days. The median length of ICU stays from ICU admission to the 1st CRE detection in CRE acquisition group was 10 days (range, 3–60) (Fig. 2). There were no cases of invasive CRE infection.
Table 1
Incidence rate of CRE and microbiologic characteristics of isolates

Table 2
Baseline characteristics and outcomes of 810 patients admitted in ICU with CRE acquisition and without CRE acquisition

Data are presented as mean ± standard deviation or number (%).
CRE = carbapenem-resistant Enterobacteriaceae, COPD = chronic obstructive pulmonary disease, HIV/AIDS = human immunodeficiency virus infection and acquired immune deficiency syndrome, APACHE II = acute physiology and chronic health evaluation II, MDROs = multidrug resistant organisms, MRSA = methicillin-resistant Staphylococcus aureus, MRAB = multi-drug resistant Acinetobacter baumannii, MRPA = multidrug-resistant Pseudomonas aeruginosa, VRE = vancomycin-resistant Enterococcus, ESBL = extended-spectrum beta-lactamase-producing bacteria, ICU = intensive care unit.
Fig. 2
Length of ICU stay from ICU admission to the 1st CRE detection (days) in patients with CRE acquisition.
ICU = intensive care unit, CRE = carbapenem-resistant Enterobacteriaceae.

In the 21 CRE-colonized patients, 22 CRE isolates were identified, with one patient colonized with both K. pneumoniae and Escherichia coli (Table 1). The most common CRE isolate was K. pneumoniae (72.7%). Carbapenemase-producing CRE comprised 42.9% (9/22) of CRE isolates and included blaKPC and blaNDM.
Men gender and old age were frequent among those who colonized CRE during ICU admission “CRE acquisition” (Table 2). They also had a higher APACHE II score at admission, and were frequently co-colonized with MRAB, MRPA, and ESBL. Device usage and previous antibiotic use were more frequent in the CRE acquisition group.
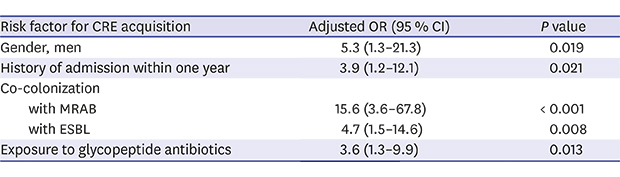
In the multivariate analysis, men gender (adjusted odds ratio [aOR], 5.3; 95% confidence interval [CI], 1.3–21.3), history of admission within one year (aOR, 3.9; 95% CI, 1.2–12.1), co-colonization with MRAB (aOR, 15.6; 95% CI, 3.6–67.8) and ESBL (aOR, 4.7; 95% CI, 1.5–14.6), and exposure to glycopeptide antibiotics (aOR, 3.6; 95% CI, 1.3–9.9) were independent risk factors of CRE acquisition during ICU admission (Table 3).
Table 3
Multivariate analysis of risk factors for CRE acquisition in 810 patients admitted in intensive care unit
Of the 810 study subjects, the average hospitalization period was 16.9 ± 20.3; 85 (10.5%) patients died during the admission. Compared to the non-CRE acquisition group, the CRE acquisition group had longer lengths of ICU and hospital stay and a higher proportion in-hospital mortality (Table 2). However, CRE acquisition was not an independent risk factor for in-hospital mortality (P = 0.109) (Supplementary Table 1).
DISCUSSION
The present study investigated the prevalence of and risk factors for CRE acquisition through active CRE surveillance in the EICU at a tertiary hospital in Korea, which is a non-endemic area. Most of the patients admitted to the ICU in the emergency room come from communities that are considered to be at a low risk for MDROs. The prevalence of CRE colonization among adult patients at the time of admission was 2.8% (23/833). The CRE acquisition rate, and incidence in patients admitted to the ICU were 2.6%, and 4.3/1,000 person-days, respectively. In the CRE acquisition group, APACHE II Score was higher, and the proportion of patients who needed additional antibiotic exposure and invasive treatments was higher. The independent risk factors of CRE acquisition during ICU admission were men gender, history of admission within one year, co-colonization with MRAB and ESBL, and expose to glycopeptide antibiotics. In CRE acquisition group, length of ICU and hospital stay was longer and in-hospital mortality was higher. To our knowledge, this is the first report to assess the risk factors for CRE acquisition during ICU stay by conducting weekly ASC-CRE in a non-endemic region.
Infection with MDROs is increasing worldwide,21 and of the MDROs, CRE infections are a specific threat to public health.123101622 In United States, the reported incidence of CRE infection is 2.93/100,000 people.2 One study in Brazil reported a CRE colonization rate of 6.8% at admission, and a CRE acquisition rate of 18% in patients admitted to the emergency room.23 The carbapenem-resistant K. pneumoniae (CRKP) acquisition rate during the ICU stay ranged from 27%–72.6% in endemic areas.1024 Asia has been reported to have a low CRE incidence; however, it is increasing. In China, the overall CRE infection incidence was 4/10,000 discharges.3 Furthermore, in Korea, there have been sporadic outbreaks and episodes of CRE.1 In one study, the prevalence of CRE carriers at admission was 0.3% (1/347), and the CRE acquisition rate was 2.9% (4/140) in the ICU of a tertiary university hospital.17 Another study in 2013 showed a CRE prevalence of 7.5% (3/40) in the rectal swab cultures of patients admitted to the ICU of a tertiary university hospital.25 The carbapenem-resistance rate of E. coli and K. pneumoniae blood isolates were reported as around 0.1% and 1.0%–1.3%, respectively, according to Korea-Global AMR Surveillance System.26 Our study showed that the rate of CRE colonization on admission, and the acquisition rate during the ICU stay were 2.8%, and 2.6%, respectively, revealing that Korea is no longer an area with low CRE prevalence.
Previous reported risk factors of CRE colonization include prior exposure to healthcare facilities (an ICU stay, hospitalization, and regular visits to the outpatient department), pulmonary disease, liver disease, immunosuppression, prior antimicrobial exposures, previous use of carbapenem, β-lactams/β-lactamase inhibitors, penicillin and glycopeptide, days of antibiotic therapy, and indwelling devices (vascular catheter, and mechanical ventilation).121723272829 In addition, CRKP infections are associated with high mortality rates.1230 There have been a few studies on the risk factors for CRKP colonization and acquisition in endemic areas. A study in Israel reported that independent risk factors for CRKP acquisition included recent surgery, and Sequential Organ Failure Assessment score.10 In Greece, risk factors for infection with K. pneumoniae carbapenemase-producing KP (KPC-KP) during ICU stay were men gender, previous bed occupant who was colonized with KPC-KP, nearby beds colonized with KPC-KP, tracheotomy, invasive catheterization, and number of antibiotics.24 In our study, 72.7% of the CRE isolates that were acquired comprised K. pneumoniae, and KPC-KP comprised 28.6% (6/21). The presence of invasive devices was not identified as independent risk factors for CRE acquisition. Independent predictors for the acquisition of CRE in ICU patients were men gender, previous admission, co-colonization with MRAB and ESBL, and expose to glycopeptide antibiotics.
Rectal colonization with CRE has been identified as an important risk factor for the development of CRE infection. In a recent meta-analysis, approximately 16.5% of CRE colonization cases were reported to be of an invasive nature.15 CRE-colonized patients had a 10.8-fold higher risk of CRE infection than in non-colonized patients.6 However, active surveillance is limited in terms of cost-effectiveness for all patients, especially in CRE non-endemic areas. Ben-David et al.13 reported that 52% of patients with CRKP infection or colonization were identified by screening culture, and active surveillance testing was effective in reducing hospital transmission in high-risk patients.1315 Ho et al.14 revealed that ASC-CRE was highly cost effective in reducing the CRE infection rate and mortality in a non-endemic area.
Hwang et al.31 reported that CRE active surveillance was not effective in patients transferred from long-term care facilities to a tertiary hospital located in Gyeonggi province, a mid-west province in Korea. However, the CRE incidence in Korea varied. In June 2017, CRE was classified as a notifiable infectious disease in Korea. The CRE incidence rate in Busan, Southeastern province, where this study hospital is located, was reported as 24.25/100,000 in 2017.32 The CRE incidence rate in Gyeonggi province was reported as 6.43/100,000 in 2017.
This study had several limitations. First, despite a study period of more than one year, only 21 (2.6%) patients were found to contract CRE. Therefore, there are some limitations to the application of risk factors in the CRE endemic area. Second, we analyzed the association between CRE acquisition and in-hospital mortality rate. However, all-cause mortality and CRE infection from CRE colonization through long-term follow up were not evaluated. Third, ASC-CRE was performed together with carbapenemase PCR to increase the sensitivity of CRE detection at admission, but the follow-up was only performed by CRE culture. The sensitivity of CRE culture by CDC protocol is about 85% (58%–96%),33 so we cannot exclude the presence of false negative CRE culture. Fourth, patients with CRE colonization can act as reservoirs for transmission of CRE to other patients, resulting in carriage, infection, or outbreak. ASC-CRE is an important measure for early detection of these reservoirs, such that they can be isolated by applying contact precaution.34 However, we did not analyze whether the incidence of CRE outbreak was decreased than the introduction of ASC-CRE.
In conclusion, CRE acquisition rate, and incidence were 2.6%, and 4.3/1,000 person-days, respectively, during ICU stay in the emergency department in a non-endemic area. Men gender, history of admission within one year, co-colonization with MRAB and ESBL, and expose to glycopeptide antibiotics were risk factors for CRE acquisition during ICU admission. The identification of patients with risk factors for CRE acquisition and early detection of CRE acquisition using ASC-CRE may be useful for CRE control. Further studies on targeted screening strategies based on a risk prediction model for CRE acquisition and its effect on prevention of CRE outbreaks or invasive infections are needed.
 XML Download
XML Download