

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Tuberculosis (TB) is an infectious disease, most commonly of the respiratory system, caused by Mycobacterium tuberculosis. The symptoms on presentation include chronic cough, fever, and production of sputum, among others. According to the global tuberculosis report, 2017, approximately 1.6 million new cases of TB were reported worldwide in 2016, with approximately 1.67 million deaths.1
Asymptomatic individuals who do not transmit the infection despite being infected with M. tuberculosis are considered to have latent tuberculosis infection (LTBI).1 It is estimated that 1 out of 3 adults are infected with latent TB in Korea.2 About 10% of people infected with latent TB progress to active TB, so it is important to control the TB epidemic.34 In 2016, the Korea Centers for Disease Control & Prevention (KCDC) prepared an “Implementation plan” for a TB-safe country. The focus of the policy has been directed to the need for the reduction of TB cases through active detection and management of LTBI patients.2
Many Koreans are exposed to congregated settings (settings in which a large numbers of people spend a considerable amount of time together in relatively enclosed spaces) such as in schools and military institutions. Since the risk of a TB epidemic is high in congregated settings, TB interventions are particularly relevant in their context. Since 2013, the KCDC has performed epidemiological investigations in contacts of contagious TB cases with an exposure period of more than one day in congregated settings.2 In particular, the KCDC has performed epidemiological investigations and TB control projects in these settings using the National Tuberculosis Control Guidelines,2 the Tuberculosis Epidemiological Investigation Guidelines,5 the Tuberculosis Control Guidelines for Schools,5 the Tuberculosis Control Guidelines for Correctional Institutions,5 and the Tuberculosis Control Guidelines for the Military and Police.5 The guidelines, including the implementation criteria for epidemiological investigations, were revised along with the progress made on the TB control project in congregated settings since 2013. Studies on TB control in congregated settings in Korea and in other countries have comprised various populations including children, youths, and school-goers.678 These studies include those conducted among healthcare workers, patients in medical institutions,91011 inmates in social welfare facilities,1213 military and police units,141516 correctional institutions,17181920 and workers in certain workplaces.21 There are also studies on prevalence, diagnosis, and completion of treatment for latent TB, which were mainly conducted to report on the effects of treatment initiation and completion among LTBI-infected people.22232425 In addition, some studies were performed on TB contacts.262728 These preceding studies have partially investigated the characteristics or influencing factors in patients with LTBI, based on the type of facility. However, no studies have determined the indicators of the management of latent TB (diagnosis, judgment regarding need for treatment, and the start and completion of treatment) among contacts and LTBI patients, and the influence of the characteristics of the index case and the type of facility where the infection occurred.
The present study aimed to identify the factors influencing the occurrence of latent TB in the exposed population in congregated settings, based on the type of facility and the year. Indicators of different congregated settings were also calculated and compared, accounting for the type of facility and index case characteristics.
METHODS
Data sources
The present study utilized raw data from the TB epidemiological investigation databases in congregated settings, which were collected by the KCDC between January 1, 2013 and December 31, 2016. TB epidemiological investigations are performed according to the National Tuberculosis Control Guidelines when more than 2 active TB patients are identified within 6 months or more than 1 case of infectious TB occurs.2 For the management of TB in Korea, the databases are the only source of data for the onset of TB in the first and additional patients in congregated settings, their contacts, outcomes of diagnosis, and the treatment of latent TB. The TB databases include information collected from congregated settings and include data on epidemic clusters, TB patients, their contacts (i.e., those who had been in contact with a patient for more than 1 day during the period of communicability), and information on patients with LTBI. Based on the four most recent years (2013–2016) of epidemiological investigations, data for 8,648 TB clusters (occurring in congregated settings) were available for the present study. The number of clusters and contacts analyzed by process are shown in Fig. 1.

Definitions of indicators and variables in the TB process
In this study, the general characteristic variables included were: gender of the first index case diagnosed with active TB in the cluster and age (0–12, 13–18, 19–29, 30–39, 40–49, 50–59, 60–69, and 70 years or older). TB-related variables including sputum test results (negative and nontuberculous mycobacterium [NTM], unknown, culture positive, and smear positive), chest radiography findings (normal, unknown, cavity-negative TB, cavity-positive TB), presence or absence of symptoms, and duration of symptoms (no symptom, 1–3 weeks, 4–5 weeks, 6–7 weeks, and 8 weeks and over).
To examine the effect of facility type, congregated settings were categorized as: school, workplace, medical institution, social welfare facility, military and police units, correctional institution, and other facilities. To find the effect of the year when an epidemiological investigation was performed, the year cluster was divided into two groups (2013–2014, 2015–2016). Since the database did not include information on the sub-type of schools, categorization according to school type was not possible.
For examining the variables related to the diagnosis and treatment of latent TB contacts, latent TB diagnosis, need for treatment, treatment initiation, and treatment completion were treated as outcome variables; rates for each indicator were then calculated. The diagnosis rate of latent TB was defined as the number of persons diagnosed with LTBI (n = 46,535 in 8,648 clusters) among the contacts who completed the test (n = 488,735). The rate of the need for treatment, was the percentage of people diagnosed with latent TB and deemed necessary to treat (individuals aged 35 years or younger, susceptible to isoniazid and rifampin, not immunosuppressed, no history of TB infection or treatment, and non-diabetic) (n = 32,938).2 The rate of treatment initiation was defined as the percentage of people who needed and were started on treatment (n = 25,002); the rate of completion of treatment was defined as the percentage of people who completed the treatment schedule (n = 19,562).




Analytic methods
The general characteristics of the first index case in the TB outbreak groups were described using univariate analysis according to the types of facilities. Mean values and 95% confidence intervals (CIs) were also evaluated to determine the rates of diagnosis, need for treatment, treatment initiation, and treatment completion of LTBI in each TB outbreak group. In addition, t-tests and variance analysis were performed to identify differences between clusters depending on the characteristics of the first index case.
To identify factors affecting the diagnosis and treatment of latent TB, multilevel logistic regression analysis was performed. Multilevel analysis is known as an analytic method that considers upper level contextual effects, such as the ‘area belonged to at the local level’ or ‘time for example, year cluster’.29 In the multilevel logistic regression model used for this study, dependent variables included diagnosis and need for treatment of latent TB, as well as the initiation and completion of latent TB treatment in TB outbreak groups. Independent variables corresponding to level 1 (individual level) were biological characteristics (gender and age), TB characteristics (sputum test results, chest radiography results, and presence or absence of symptoms and its duration) of the index case, as well as the facility type. Independent variables for level 2 (year level) were year clusters (2013–2014 and 2015–2016). In addition, the median odds ratio (MOR) was calculated to examine variations by year. MOR is calculated as follows:

Here, ö refers to the cumulative distribution function in the normal distribution with a mean of 0 and a variance of 1, where ö−1(0.75) is the 75th percentile.3031 MOR refers to an indicator that quantifies the variation between levels, by comparison between two individuals between different levels (year cluster in the present study); this is the median value of the odds ratios (ORs) in one group with a higher tendency and another with a lower tendency. MOR is a value that evaluates the degree of variation in outcome variables at the higher-level cluster (year in the present study) compared to the individual level (when considering variables at the individual level), which is equivalent to the fixed-effects ORs.303132 The MOR value is always 1 or more. An MOR value of 1 implies no variation between levels; the MOR value increases when there are considerable variations between levels. The present study used the PROC GLIMMIX command in the SAS 9.4 software package (SAS Institute Inc., Cary, NC, USA) for multilevel logistic regression analysis. The statistical significance level in this study was reported at P < 0.05.
RESULTS
General characteristics
Data pertaining to the characteristics for each epidemiological cluster is presented in Table 1. Among the 8,648 TB clusters investigated from 2013 to 2016, schools (2,925 clusters, 33.8%), accounted for the highest proportion of outbreaks according to facility type, followed by medical institutions (2,100 clusters, 18.8%), and social welfare facilities (1,624 clusters, 13.2%). In terms of the gender and age of the first index case, the total cluster had a higher proportion of men (4,870 clusters, 56.3%) than women; and the age group of 19–34 years accounted for the highest proportion (2,483 clusters, 28.7%). Regarding the sputum test of the index case, the highest rate of smear positivity was found to be 59.2% (5,188 clusters), while culture positivity was 31.7% (2,740 clusters). On chest radiography, the proportion of cases with cavity-negative TB was the highest at 61.5% (5,320 clusters), followed by cavity-positive cases, at 26.7% (2,306 clusters). The highest duration of symptoms for the index case was 1–3 weeks (3,371 clusters, 39.0%), followed by those with no symptoms (2,551 clusters, 29.5%), and those with symptoms for 4–5 weeks (1,275 clusters, 14.7%). For epidemiological investigation by year, the rate for the year 2015–2016 was 69.0% (2,678 clusters), which was 2.23-fold higher than that of the year 2013–2014.
Table 1
Number and percentages of the index case of cluster

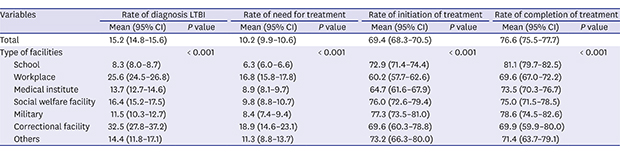
Table 2 shows the rates of need for treatment, treatment initiation, and treatment completion by type of facility and year group. The total LTBI diagnosis rate for contacts who completed the latent TB test was 15.2% (95% CI, 14.8%–15.6%). Highest LTBI diagnosis rates by type of facility, were noted in correctional institutions (32.5%; 95% CI, 27.8%–37.2%), and by year, in the 2015–2016 group; the diagnosis rate increased with the advancement of years. The rate of need for treatment of contacts who were diagnosed with latent TB was 10.2% (95% CI, 9.9%–10.6%). Correctional institutions showed the highest rate of need for treatment of contacts at 18.9%, followed by the workplace, at 16.8%. By year, the need for treatment of contacts was 12.0% in 2015–2016; this value was approximately 2-fold higher than that in 2013–2014.
Table 2
Rate of indicator by process for LTBI diagnosis and treatment by cluster

The treatment initiation rate of contacts diagnosed with latent TB needing treatment was 69.4% (95% CI, 68.3%–70.5%). By year, the treatment initiation rate of contacts significantly and progressively decreased in recent years, with a decline from 76.3% in 2013 to 64.2% in 2016 (P < 0.001).
The treatment completion rate of contacts who started treatment was 76.6% (95% CI, 75.5%–77.7%). Among facility type, schools showed the highest treatment completion rate at 81.1%, compared with the workplace, at 69.6%. The treatment completion rate of contacts progressively decreased in the recent years.
Influential factors in the process of latent TB: multilevel regression analysis
As shown in Table 3, multilevel logistic regression analysis was performed using the diagnosis of latent TB in contacts, need for treatment, treatment initiation, and treatment completion as dependent variables, and the characteristics of the index case and cluster as independent variables; years were considered as a random effect. All indicators showed significant differences depending on year (MOR, 1.133–1.189). Compared to school, the other facilities that the index case belonged to, such as the workplace, showed a significantly higher rate of latent TB diagnosis in contacts (P < 0.001). Correctional institutions had a high risk for latent TB diagnosis (OR, 6.37; 95% CI, 5.92–6.86). By year cluster, LTBI became significantly lower with the progression of years (OR, 0.75; 95% CI, 0.61–0.91). Among contacts, men index cases had a 1.16-fold higher LTBI diagnosis rate than women index cases. Compared to the 70 years or older age group, all other age groups showed a significantly higher LTBI diagnosis rate in contacts; however, there was no apparent pattern (P < 0.001).
Table 3
Impact of factors for diagnosis of contacts, need for treatment, initiation and completion of treatment for latent TB using multilevel logistic regression
When the need for treatment of latent TB was used as a response variable, most variables showed significance similar to that of latent TB diagnosis. When compared by type of facility that index cases belonged to, other facilities showed significantly high ORs for rates of need for treatment of latent TB compared to schools (P < 0.001). In particular, the risk for the need for treatment was the highest in correctional facilities (OR, 4.49; 95% CI, 4.13–4.89; P < 0.001). When OR was examined by year, the rate of need for treatment of contacts with latent TB was significantly lower in the most recent year (OR, 0.82; 95% CI, 0.67–0.99; P < 0.05). Men index cases had a 1.11-fold higher rate of need for treatment of contacts with latent TB compared to women cases; this was significantly higher in all ages of index cases (P < 0.001).
When treatment initiation of latent TB was used as a response variable, most variables were statistically significant. Other facilities except the workplace had significantly higher ORs of treatment initiation rate in contacts (P < 0.01), while the OR of the workplace was significantly lower, at 0.72 (95% CI, 0.654–0.793). By year cluster, the treatment initiation rate in latent TB became significantly lower in the most recent year (OR, 0.65; 95% CI, 0.49–0.87; P < 0.01). Compared to women cases, men index cases had a 1.19-fold higher rate of treatment initiation among contacts with latent TB. By age group, the 13–18 years and 40–49 years groups showed significantly higher rates than the group aged 70 years and above (P < 0.001); the rates in the other age clusters were not significant.
Multilevel logistic regression analysis using treatment completion in latent TB as the response variable, found that all variables except the gender of the index case and sputum test results were significant. When examined by facility type of index cases, all facilities except other facilities demonstrated significantly lower treatment completion rates among contacts (P < 0.01). Unlike other indicators, when OR was examined by year, it showed no significant results.
DISCUSSION
The present study is the first to calculate the indicators related to latent TB and to investigate the influencing factors among congregated settings in Korea. Depending on the type of facility, each indicator was found to have significant differences along the process, from diagnosis of latent TB to treatment completion; differences were also noted depending on year cluster.
According to the results of this study, the most extensive epidemiological investigation was conducted at schools, compared to other facilities. This may be explained by the fact that a longer time is spent in communal living in schools, with longer contact times. In addition, schools have a better reporting system and accessibility to medical systems than other facilities. Epidemiological investigations for TB among congregated facilities in Korea were started in schools from 2013. Remarkably, the number of epidemiological investigations rapidly increased with age, beginning from when the first index case was aged > 13 years; this was probably due to the fact that this is a rapid period of growth in youths, and they spend longer times in high school.6 As reported by Fox et al.26 in 2013, contact investigation is known to be important for children, because unlike older age clusters, in congregated settings with many children, the risk of developing active TB is higher, and the response to the latent TB test is often unreliable; more controls are therefore required.
Compared to schools, other facilities had significantly higher rates of diagnosis of LTBI and need for treatment and the rate was still high even after adjusting for other factors. In this study, correctional institutions showed the highest diagnosis rate and OR. In comparison to international studies, the LTBI rate of contacts in correctional institutions was higher in Korea than that reported in the United States (17%)17; however, it was lower than that of Spain (45.5%)18 and Brazil (49%–73%).20 It may be speculated that the LTBI risk in correctional institutions was higher than of other facilities owing to the overpopulated setting and small rooms, in addition to medical accessibility issues. Correctional institutions in Korea accommodate 1,098.8 inmates on average in each institution, corresponding to the highest level in the Organisation for Economic Co-operation and Development (OECD) member countries. Furthermore, the accommodation rate is 121.8%, corresponding to the second largest in the OECD member countries.33 Correctional institutions hold 4 inmates per 8.48 m2 of room space and 6 inmates per 12.75 m2 of room space; this corresponds to approximately 2 m2 per person. The setting in which inmates stay, living together in small rooms with short periods of outdoor activities, seemed to enhance TB transmission. In 2015, 87 doctors working in correctional institutions were in charge of 54,581 prisoners, and one doctor treated about 200 prisoners every day.34 Under such circumstances, there could be delayed identification of prisoners infected with active TB, thus the possibility of transmission to contacts increases.
In this study, medical institutions had higher rates of latent TB diagnosis, need for treatment, and treatment initiation than schools. However, the treatment completion rate was lower. This finding may be explained by the fact that medical institutions perform more tests and monitor treatment more strictly. The hospital-ward characteristics in Korea possibly had some impact. In 2017, there were a total of 154,753 wards, of which 99,523 (64.3%) were general wards accommodating at least four inpatients, indicating that a high proportion are dormitory-type wards, and 85.9% of the total 534,157 beds were in non-isolated wards.35 The setting with the most bed supplies were the non-isolated wards; this was identified as the major cause of nosocomial infections during the Middle East respiratory syndrome (MERS) outbreak in 2015.36 Although treatment of latent TB was initiated, considering the short hospitalization period of within 1 month, a relatively low treatment completion rate of latent TB indicated a poor post-discharge control. To date, there is no clear regulation for post-discharge control of latent TB patients. A system has been established to share the information about TB-infected soldiers after discharge with the corresponding community health center. In contrast, for patients with LTBI, there is no system that registers these patients after discharge in the corresponding community health center or the TB control information system. Thus, there is need to establish a system that provides continuous treatment for patients with LTBI after discharge, and the same is applicable to social welfare facilities, as well as the medical and other institutions that have admission and discharge processes.
Although the rates of initiation and completion of treatment for latent TB have reduced, patients with LTBI aged ≥ 35 years have been included as treatment targets since 2015. After 2015, in view of the lower ORs for treatment initiation and completion, the general workplace has been particularly considered for active TB control interventions in congregated settings. In a similar study in Japan, workers with latent TB had a lower treatment completion rate than patients in other occupation groups such as school students, healthcare professionals, and homemakers.22 Workplaces had lower treatment and completion rates of latent TB; this could be attributed to the large numbers of individuals aged ≥ 35 years who were recently included as treatment subjects. It could also be explained by the fact that unlike schools or correctional institutions, the guidelines for the management of infected cases in the workplace congregated settings were unclear leading greater difficulties in the management of infected individuals. Overall, these results show that unlike the case of active TB patients a system of management from initiation to completion of treatment has not been fully established for LTBI, despite the expansion in numbers of treatment subjects with latent TB. An additional system, which can monitor and manage the treatment process in patients with LTBI aged 35 years or older is also necessary.
Despite the significant findings of this study, there are a few limitations. First, the database contained only the information of Korean individuals; non-Korean individuals were not included in the analysis. The number of new TB patients among foreigners has increased in recent years, while that of Koreans has tended to decrease, showing an opposite trend.37 Follow-up studies should be performed among foreigners with TB, whose numbers seemed to be on an increase. Secondly, the characteristics (gender and age, among others) of contacts of TB patients were not considered. However, the present study primarily intended to investigate the characteristics of clusters including type of facility and effect of timing after considering the characteristics of the index case; therefore, characteristics of contacts were not a major issue. Since the age of the contacts was a characteristic of the cluster they belonged to, the range was relatively similar and its influence was considered minor. Future studies should be performed with individual units considering the characteristics of contacts. Thirdly, the characteristics of the sub-categories in the congregated settings were not considered in this study. Schools maybe classified into kindergarten, elementary school, middle school, high school, and college; other facilities also have sub-types. In previous studies, the highest number of contact cases in Korean schools was found in high schools. Kindergartens and daycare centers also showed high LTBI rates.6 As for correctional institutions in the United States, prisons where they serve their terms, had a higher treatment completion rate than detention centers that held inmates temporarily.17 Since the details supplied by the facilities were incomplete, the data in the present study did not completely reflect all sub-types of facilities. However, this study had a different goal and those variables were not considered. Further studies are necessary to evaluate individual facilities according to sub-types. Lastly, the jobs among the first index cases in congregated settings were not classified. School populations could be sub-categorized as students and teachers, and medical institutions could be sub-divided into patients and healthcare professionals (doctor and nurse). These characteristics are likely to vary. For instance, the index cases in a study had different types of occupations depending on school type6; in another study, healthcare professionals had a higher risk of LTBI due to contact with patients.13 However, the analysis in the present study was based on various types of facilities. Therefore, they were not sub-divided to ensure consistency in the analysis. In future studies, analysis should be performed by facility type as well as by occupation in individual facilities. Despite these limitations, this study identified the impact of characteristics of the first index case, type of facility, and timing in each cluster on latent TB; the findings of this study are therefore significant.
These results have considerable implications. First, the overall incidence level in the school population needs to be reduced. Since this population has more contact with the family than that of other collective facilities, it is also necessary to manage the family contacts.
Second, a strategy is needed to increase the TB-treatment completion rate among contacts in other facilities. In Korea, the management of TB in collective facilities has been focused on finding additional TB patients and identifying LTBI cases through epidemiological investigations in case of epidemics.3738 Conversely, efforts to monitor treatment in cases with LTBI were relatively less enthusiastic.3738
In Korea, patients with active TB are managed by the TB public-private mix model (PPM) recommended by the World Health Organization.138 The PPM is regarded as an effective policy for TB control in Korea and other countries.13738 However, till date, people with LTBI have not been included in the target population of the PPM. For improving levels of completion of LTBI treatment, the active management of LTBI is essential. This may be achieved by sharing information about patients to medical institutions participating in the PPM; also, public health centers need to monitor and manage the completion of treatment via telephone and text communication.
The directly observed treatment (DOT) service needs to be extended to include patients with LTBI. In Korea, the DOT service has been implemented since 2013 for patients with TB.38 However, till date, patients with LTBI are not included in the target population for DOT. Since DOT is known to be effective in improving the compliance of TB patients,1 it should be implemented to increase the treatment completion rate in these patients.
Third, a cohort of contact and latent TB cases should be established to monitor the status of management and the occurrence of active TB in the long-term. It is known that individuals with LTBI have a 10% of risk of latent TB for the rest of their lives.38 In contact control programs, epidemiological investigations can take up to 9 months.2 However, a period of 9 months is insufficient for obtaining information about the occurrence of active TB in contacts.
Fourth, tests should be performed for latent TB before including individuals in congregated settings and also during the period of stay. Fifth, accessibility to medical institutions should be improved to facilitate timely access to medical services in case of suspected TB symptoms. Lastly, it is necessary to establish a system that transfers information about latent TB patients to the corresponding community health centers after discharge from the congregated settings; this will serve to raise treatment completion rates in patients with latent TB.
The present study investigated the states and influential factors along the process, extending from the diagnosis of latent TB to the completion of treatment in Korea. The findings showed that compared to schools, other facilities carried high risks of LTBI. Therefore, efforts should be made to enhance the early detection of the first patients with TB. In addition, efforts should be made to establish policies to determine the rates of treatment completion among latent TB cases in correctional institutions, medical institutions, and social welfare facilities, and to improve the treatment initiation rate in workplaces, particularly among those aged 35 years or older. There is a growing understanding of the need to manage LTBI, but the evidence for this is lacking. Further research is needed to facilitate the implementation of evidence-based policies for the control of LTBI.
 XML Download
XML Download