

 ePub
ePub Citation
Citation Print
Print



Dear Editor:
Merkel cell carcinoma (MCC) is a rare neuroendocrine cancer of the skin. The annual incidence of MCC is 0.6 per 100,000 persons in the United States, though the rate is increasing1. However, in Asians, there have been fewer case reports of this cancer, and the incidence of MCC is estimated to be 25 times lower than that of whites2. It is a highly aggressive primary skin cancer and the leading cause of death in non-melanoma skin cancer3. Usual presentation of primary MCC is a solitary violet or blue dome-shaped rapidly growing nodule with non-tender intra-cutaneous swelling. The common locations are head and neck (50%), extremities (40%), and trunk (10%)4. Finger involvement has been rarely reported.
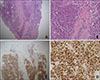
An 87-year-old female presented with an asymptomatic mass on the finger. Metastatic cancer was suspected, and she was referred to our department as a result of histopathologic examination performed at another hospitals. Physical examination revealed a solitary 1.5×1 cm sized erythematous nodule on the dorsal surface of the left 4th finger (Fig. 1). She had diabetes, hypertension, and Alzheimer's disease. We performed skin biopsy and immunohistochemistry on the lesion. The histopathological evaluation demonstrated intradermal coalescing sheets consisting of small blue cells with many atypical mitotic features. Immunohistochemical findings were positive for CK-20 and negative for anti-thyroid transcription factor-1 and S-100 (Fig. 2). Because there were no other skin lesions or evidence of metastasis on positron emission tomography/computed tomography, the patient was finally diagnosed with primary MCC. We transferred the patient to the department of orthopedics. The tumour was excised widely with a 10 mm margin of surrounding tissue. The axillar sentinel lymph node biopsy result was negative. After the surgery, adjuvant radiotherapy was performed. The patient was followed up one year after the surgery without recurrence.
The pathogenesis and risk factors of MCC are not fully understood. But, the known risk factors for MCC are sun exposure, immunosuppression, and Merkel cell polyomavirus infection1. Of all cases of MCC, 85% appear in sun exposed sites, so ultraviolet exposure seems to be a significant etiological factor4. The occurrence of MCC at the hands and fingers is likely to occur due to exposure to sunlight. A case report showed the relation of ionizing radiation exposure with the development of MCC in an 80-year-old surgeon who had frequently performed radiography using the naked hand5. Although The hand and finger may be relatively easy to expose with sun-exposure and naked radiation, MCC on these sites has been rarely reported45. Because of frequent sun-exposure and a high density of Merkel cells on the hand, however, the possibility of the occurrence of MCC would not be negligible.
Dermatologists should include the possibility of MCC when encountering painless firm erythematous nodules, especially in sun-exposed areas. Although rarely reported, considering the aggressive aspect of this cancer, MCC in the hands or fingers should be considered. If diagnosis is challenging, immunohistochemical staining is useful in diagnosis of MCC. We received the patient's consent form about publishing all photographic materials.

 XML Download
XML Download