

 ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Merkel cell carcinoma (MCC) is a rare cutaneous malignancy with a poor prognosis1. It was first described in 1972 as an indolent disease2. The current literature indicates that the disease has an aggressive course, and higher mortality rates than melanoma (approximately 46% vs. 12%) with increasing incidence34. Previous morphological studies reported that MCC originated from Merkel cells (MCs) in the basal layer of the epidermis. It has been demonstrated that these tumors originate from totipotential stem cells that exhibit epithelial and neuroendocrine properties during malignant transformation56. The annual incidence is variable and ranges between 0.11 to 1.6 cases per 100,000, and higher incidence rates were reported in Australia and New Zealand. MCC is typically seen in older individuals, with a mean age at diagnosis of 76 years for females and 74 years for males. Incidence rates were higher in males than females789.
Although the pathogenesis of MCC is not completely known, multiple factors contribute to the etiopathogenesis of MCC including older age, increased aggregate ultraviolet (UV) exposure, immunosuppression, and Merkel Cell Polyomavirus (MCPyV) infection1. MCC typically presents as a rapidly growing, painless, firm, non-tender, shiny, flesh-colored or bluish-red, intra cutaneous nodule. Early tumors are usually misdiagnosed as benign lesions (e.g., cyst, lipoma, pyogenic granuloma). Early recognition of MCC is important since the expected 5 years survival is 79% in the early stage (IA), unfortunately only 18% by the time of metastasis (stage IV). High clinical suspicion and early diagnosis may improve survival rates10. Due to its rarity epidemiological data are scarce, and have not been previously analyzed in Turkey to identify the main epidemiological trends. The aim of this study was to describe the clinical characteristics, demographic features, therapeutic parameters, and outcome of MCC cases from Turkey.
MATERIALS AND METHODS
Patients
We retrospectively analyzed the digital medical records of the 13 patients who were followed-up between January 2008 and January 2018 with the diagnosis of primary cutaneous MCC. Our tertiary referral center is located in the south east Marmara region of Turkey about 5 million population. Basic patient demographics (age of onset, gender), past medical history (diabetes mellitus, hypertension, coronary artery disease and malignancy), tumor characteristics (duration of the lesion, localization, maximum tumor size), treatment parameters including surgical margin, tumor, node, metastasis (TNM) stage, treatment modalities, follow-up period, recurrence, and survival status were retrieved from computerized medical records. Immunosuppression status was considered positive if the patients had any history of solid organ transplantation, were taking chronic immunosuppressive or chemotherapeutic drugs, or had a prior or current diagnosis of chronic leukemia or lymphoma11. Ethical approval was obtained from the ethics committee of the Uludag University (approval number: 2017-14/39). Written informed consent was obtained from the patient or legal guardian to report and publish the identifiable patient images.
Diagnosis and management
Histopathological diagnosis required that the tumor morphology was consistent with MCC on hematoxylin-eosinstained tissue sections and that the specimens were immunohistochemically positive for cytokeratin 20 (CK20). If CK20 was negative, but morphology consistent with MCC, the diagnosis was confirmed by immunostaining for Synaptophysin and Chromogranin A. Negative immunostaining for thyroid transcriptase factor 1 was required to rule out metastatic small cell lung carcinoma12.
Clinical or radiological evidence of lymph node involvement or distant metastasis were evaluated for all patients with a biopsy-confirmed cutaneous MCC. Management of the primary lesion included wide local excision (WLE) with margins of at least 2 cm of normal appearing skin wherever possible, adjuvant radiotherapy (RT), chemotherapy (CT) or a combination of these modalities were recommended as individual basis. The tumors were staged according to the American Joint Committee on Cancer (AJCC) staging recommendations. Overall survival (OS) was measured from the date of presentation to the date of death from any cause13.
Statistical analysis
Statistical analyses were performed by IBM SPSS Statistics for Windows ver. 20.0 (IBM Co., Armonk, NY, USA). Mean±standard deviation were calculated for continuous variables, while percentiles and frequencies were reported for categorical variables. The Kaplan–Meier method was used for survival estimations and the log-rank test was used for survival curve comparisons. All comparisons were two-tailed, with a p-value of 0.05 or less considered to statistical significance.
RESULTS
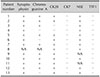
Total of 13 patients were followed-up during 10 years period. Mean age at the onset of the lesions was 71.23±10.83 with median was 69 years. Female predominance (61.5%) was noticed. None of the preliminary clinical diagnosis was MCC before the histological examination. All diagnoses were confirmed by immunostaining (Table 1). The duration of the lesions was ≤3 months in nine (69.2%) patients. The most common primary site of the tumors was the lower extremities (Fig. 1) followed by head and neck (Fig. 2), and 77% of lesions were located on the extremities. One (7.7%) of patients had a tumor at a highly sun-protected site (buttock), and one patient (7.7%) had tumor arise on partially protected sites (thighs) (Fig. 3). One male patient had bilateral lesions. While more than 90% of the lesions were asymptomatic, pain was noticed with a 10 cm tumor with 12 months' duration. Concomitant malignancy (diagnosed prior, after or during the initial evaluation of the MCC diagnosis) was detected in four cases including; papillary thyroid carcinoma in one patient diagnosed six months after the diagnosis of MCC and breast carcinoma (T1N0M0) in another patient diagnosed two years before the diagnosis of MCC. One patient had a 15 years history of stage III chronic lymphocytic leukemia (CLL) without any medication and simultaneous basosquamous cancer. One patient had simultaneous breast carcinoma (patient numbers 2, 8, 9, and 11 respectively). Two of the patients had a history of immunosuppression due to CT for CLL and breast carcinoma. Seven patients had long-term comorbidities including diabetes mellitus, hypertension, and coronary artery disease, which some authors described as immunocompromised patients14.
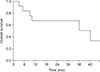
At presentation, 39% of the lesions were confined to the skin (AJCC stage 1~2). Within a median 15 months follow-up only one patient developed metastasis on the regional nodes after 12 months who had a 1×1 cm primary tumor on the hand, and treated with only WLE without RT (patient number 6). During the follow-up period six (46.2%) patients were died; seventh patient was dead due to cardiovascular arrest at third years of follow-up unrelated with treatment, ninth patient was dead within three months after MCC diagnosis, during initial evaluation who had history of stage III CLL for 15 years without any treatment, tenth patient was dead at first year of follow-up unrelated with treatment, eleventh patient was dead at first year of the follow-up due to febrile neutropenia after CT, twelfth patient was dead at fifth years of follow-up unrelated to treatment, and thirteen patient was dead within first year due to febrile neutropenia after CT. Epidemiological, clinical, and demographical characteristics of the patients were presented in Table 2, 3. OS was 42 months (Fig. 4), and 68% at first year, 68% at third years, and 29% at fifth years. The effect of factors on survival could not be evaluated statistically due to small numbers of the patients.
DISCUSSION
The epidemiologic, demographic, and clinical characteristics of MCC patients shows differences in the literature are mainly consist of single-institution retrospective studies with small numbers in western and eastern populations, and little is known in Turkey aside from a few case reports15161718192021222324252627282930. Increasing incidence of MCC had been reported worldwide; however, incidence was similar in this study in two periods of five years MCC predominantly affects elderly Caucasians, and a male predominance has been reported in large studies789. Most of our patients were elderly, in their eighth decade of life on average, as reported in the literature. Approximately 31% of our patients were younger than 65 years, and the youngest was 57 years old. A female predominance with a female/male ratio of 1.6 was noticed in this study. Review of literature revealed that the female/male ratio was ranging between 1.12 to 3 in Denmark, Finland, United Kingdom, Germany, Italy, China, and Korea1617181920212223. MCC appears to be more common at sun-exposed areas including the head and neck (46%~48%), in Caucasian populations, nevertheless MCC can arise in UV-protected areas including the extremities (35%~38%) and trunk (11%~17%)131. The lower extremity predilection was reported in African-Americans32. In our study, the most common primary site of tumors was the lower extremities followed by the head and neck, although most studies report the reverse sequence789. Lower extremity was the second most common site in Heath et al.'s report33 from Australia. Several reports from New York, the United Kingdom, India, Italy and Greece noticed a predilection for the extremities222324252627. The last two countries are Mediterranean countries like Turkey, and Hindus are the largest migrant population in the United Kingdom.
MCs are located within the basal epidermis, being concentrated in eccrine glandular ridges of glabrous skin, and within hair follicles which works as slowly adapting mechanoreceptors34. The distribution of MCs may help the understanding of their function. There is a site variation in the density of MCs, and probably does not reflect only the effect of chronic sun-exposure because much variation has also been reported in fetal skin3536. Although the number of the our patients are small the accumulation of primary tumors around the high pressure joint like knee took our attention (Fig. 3). This accumulation may be related with mechanoreseptor function of MCs or a predilection site for our region.
MCPyV has been found in normal skin at all body sites as well as in urine, nasal, and respiratory secretions, and seroprevalence of antibodies increases with age37. MCPyV is integrated into genomes of up to 80% of human MCC. The integration of the virus into the genome precedes the clonal expansion of tumor cells. It has been reported that MCPyV-DNA positivity was more common at sun-exposed area tumors including head, neck, forearm and lower thigh38. In the Northern hemisphere, the majority of MCC cases had viral etiology, while in areas with high UV exposure, UV–mediated carcinogenesis is predominant. Although there is no consensus, it has been reported that MCPyV positive MCC shows less metastatic tendency and better prognosis38.
Although presentation with other skin cancers is common, only one of our patients had a diagnosis of basosquamous cancer strongly associated with UV exposure; however, this patient had a 15 years history of stage III CLL, which is an another risk factor for the development of non-melanoma skin cancer39.
The risk of MCC is significantly increased in patients with other malignancies. A meta-analysis demonstrated that there is an overall increased risk for second malignancies one year after the diagnosis of MCC40. However, four (30.8%) of our patients had an accompanying malignancy, including breast carcinoma in two patients, CLL and newly diagnosed papillary thyroid carcinoma. This may be a real relationship, but it may also be a simple outcome of a detailed assessment for staging after the diagnosis of MCC in the older population. The higher incidence of MCC in immunosuppressed subjects had been reported. In our study, two (15.4%) of the patients had immunosuppression due to immunosuppressive agents.
The acute onset of the tumors in this study occurred at a median of three months; however, some tumors located on the extremities became prominent up to 12 months duration. This may be related to the late detection of lesions which located in an invisible area and neglected by the patients because of the asymptomatic nature of the lesions. The size of the tumor can vary up to 15-cm in diameter, with an average of three cm at presentation, as we observed. The AEIOU acronym was proposed to define the clinical risk factors of MCC from Australia: Asymptomatic (88%), rapidly Expanding (63%), Immunosuppression (8%), older than 50 years of age (90%), and UV exposed area on fair skin (81%)33. In this study, more than 90% of the patients were asymptomatic, 69% of the patients had developed lesions within three months, immunosuppression was noted in 15% of the patients, all of our patients were older than 50 years, and 76% of the lesions were located on sun-exposed areas. The clinical and demographic features of our cases overlap with those of the AEIOU acronym with a predilection for the lower extremities.
The eighth (2017) edition of the TNM staging system is recommended by both the AJCC and the Union for International Cancer Control (UICC) is based upon an analysis of 9,387 patients with MCC. At presentation, 65% of patients had local disease, 26% of patients had regional lymph node involvement and 8.4% of patients had distant metastatic disease13. In this study, 61% of the patients had regional and metastatic disease. These reverse results may be explained with increasing knowledge of the MCC and more careful application of staging procedures, improved diagnostic techniques, and the use of different staging methods prior to the AJCC recommendation161720232526. In addition, the high rate of advanced stage may be the natural course of MCC patients seen in our region. There is no standardized management of MCC, and randomized trials are challenging due to relatively small numbers of the reports. Most patients with MCC are treated by WLE followed by adjuvant RT. RT has an important role in patients with MCC to treat occult lymph node disease or minimal residual tumor at the primary site. Systemic CT has demonstrated high response rates in patients with metastatic disease41. Our experience, compatible with previous literature, RT is the best option for locoregional control, although we were unable to demonstrate this statistically due to the small number of cases. The natural history of MCC is variable. The median OS in this study (42 months) was lower than previous reports, which tends to be approximately 60 to 70 months, although the 5 years OS was within the reported range of 30% to 60%11. Significant favorable prognostic factors for OS were described as localized disease, female sex, age less than 65 years, and the absence of comorbid conditions1342. Since the number of the patients were small, the effect of factors on survival could not be evaluated statistically. This is a retrospective study with a small number of patients, and we could not investigate the virological features of the cases, which are major limitations of this study.
This is the first largest report from a Turkish population. Female predominance and a lower extremity tendency were remarkable. Clinicians should keep in mind the diagnosis of MCC, especially for asymptomatic fast-growing lesions with older patients. The well-known clinical and demographic characteristics are vital for the differential diagnosis and early management of patients.





 XML Download
XML Download