

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Constipation is a common problem occurring in up to 29.6% of children of all ages and is a cause for concern for many parents [12]. The median prevalence of constipation in infants up to 12 months of age is 7.8% [3]. In more than 95% of the children, no underlying cause for constipation can be found and is consequently defined as functional constipation [4]. In the remaining proportion of children, constipation occurs due to the underlying condition, which includes metabolic, musculoskeletal, or neurologic conditions such as Hirschsprung's disease [56].
Age at gestation, birth weight, colic, and breastfeeding are important factors associated with constipation in infants [78]. Although exceptions do exist, breastfed infants produce a greater number of stools than infants who consume a combination of breastfeeding and formula feeding [9]. Hard stool consistency is also more frequent in formula-fed infants aged less than four months of age (9.2%) compared to only breastfed infants of the same age (1.1%) [8]. Premature babies, specifically those born at gestational ages between 23 and 26 weeks exhibit symptoms of constipation at 6 months of age [10].
Treatment of constipation in infants and children primarily involves parental education about the condition as well as dietary changes, including the use of dietary fiber [51112]. However, due to the poor quality of studies, evidence for the effectiveness of fiber and probiotic supplementation in infants with constipation, as well as other gastrointestinal disorders, remains inconsistent [1314]. The European Society for Pediatric Gastroenterology Hepatology and Nutrition/North American Society for Pediatric Gastroenterology, Hepatology and Nutrition guideline strongly suggest starting oral medication, suppositories, and disimpaction as soon as possible if symptoms of constipation persist [51516]. Magnesium (Mg) intake has been shown to improve stool consistency in children, adults, and the elderly [17-21]. In experiments in a rat model, Mg sulfate increased the expression of aquaporin 3, a water channel protein found in the colon, and increased osmotic pressure, resulting in the increased water content of feces [22]. Constipation in children has also been associated with low dietary intake of Mg [23].
This study aimed to compare the effectiveness of the Mg-rich formula in terms of improving stool consistency and stool frequency in infants with constipation. Furthermore, the study aimed to assess effectiveness with regards to relief in constipation symptoms, parent satisfaction, and tolerance of treatment.
MATERIALS AND METHODS
Study design
An open-label, interventional, randomized, comparator-controlled, and multicenter study was conducted across 15 sites in the United Arab Emirates, Kuwait, Kingdom of Saudi Arabia, Oman, and Lebanon.
Study population
Between December 2016 and October 2017, infants were recruited from outpatient clinics at 15 participating hospitals. Infants aged six months or less, fully formula-fed, and meeting modified Rome IV criteria (at least one of the following: two or fewer defecations per week; a history of excessive stool retention; painful/hard bowel movements) were eligible for inclusion. Patients were excluded if they were exclusively breastfed or mixed-fed, diagnosed with infant dyschezia, had an organic cause of constipation, or on laxative treatment. Infants with a significant developmental delay associated with a musculoskeletal or neurologic condition affecting the gastrointestinal tract were excluded as well. Infants with constipation secondary to endocrine, metabolic, neurologic, organic, autoimmune disorders, surgery, or drugs as well as those with clinically significant cardiac, vascular, liver, pulmonary, or psychiatric disorders, severe renal insufficiency, human immunodeficiency virus or acquired immunodeficiency syndrome, hepatitis B or hepatitis C were also excluded. Finally, infants with clinically significant abnormalities of hematology, urinalysis, or blood biochemistry at the time of screening, known cow milk protein allergy, allergy to investigational formulae, and anemic infants under oral iron supplementation were excluded.
Ethics
The protocol and consent form were reviewed and approved by the Institutional Review Board/Independent Ethics Committee of each participating site prior to study initiation. The study was not registered in a central database. Written informed consent was obtained from the parents or guardians of infants meeting the inclusion criteria prior to study initiation.
Treatments
Consenting patients were randomized in a 1:1 ratio to receive either the Mg-rich formula (Novalac IT 1; United Pharmaceuticals SAS, Paris, France) or the control starter formula (Similac Comfort 1; Abbott Nutrition, Columbus, OH, USA) treatment for 30 days, as per a computer-generated random sequence. A summary of formula compositions is provided in Table 1. Subjects were fed exclusively with the study formulae, according to each formula's standard feeding schedule provided by the manufacturer. Dosing as well as preparation and storage of formula were in accordance with the manufacturer's recommendations. If constipation continued for three days after starting either of the formula treatment, rescue medication was permitted. Rescue medication was the administration of 2.5 mL lactulose (Duphalac®) or if constipation persisted for further two days despite lactulose treatment, infants were given a micro-enema (Microlax®), PEG 3350 (Movicol®), or other laxatives, at the physician's discretion. Use of rescue medication, including dose, route, frequency, indication, and duration of use were recorded in the patient case report form (CRF). In the 30-day study period, the use of medications influencing intestinal motility was not allowed, unless necessary for the infants' wellbeing; in which case, information regarding the type of medication, dose, route, frequency, indication, and duration of use was recorded in the CRF.
Table 1
Summary of the composition of the tested formulae
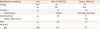
Mg: magnesium, Mg-rich formula: Novalac IT, Control formula: Similac Comfort™ 1; GOS: galactooligosaccharide.
![]()
Data collection
Three physician visits per patient were scheduled at day 0 (baseline), 8, and 30. At the baseline visit, a CRF was completed by the physician and the information relating to patient demographics (age, gender, and ethnicity), birth weight and length, head circumference, gestational age at birth, mode of delivery, number of siblings, number of infants born in the same pregnancy, medical history, and feeding history was obtained. At the 2 follow-up visits, on days 8 and 30, further CRFs were completed, which recorded details of the clinical examination of the patient, concurrent medications, assessment of constipation symptoms, adherence to formula, and occurrence of adverse events.
Parents completed the patient diaries on days 1 to 7 and 23 to 29, to describe the patient's gastrointestinal symptoms. Information regarding the number of stools, stool consistency, crying during defecation, pain during defecation (using Faces Pain Scale), withholding stools, use of rescue medication, food intake, medication use, number and duration of crying episodes, adverse events, and parent satisfaction with treatment were reported at each follow-up visit.
Outcomes
Primary endpoints were improved stool consistency and increased stool frequency. Stool consistency was reported as per a pre-specified stool scale of three groups wherein group 1 consisted of "hard stools" and was defined as pellets/separate hard lumps like nuts or sticky dough-like consistency, group 2 consisted of “normal stool” which was defined as soft stool with smooth consistency, and group 3 consisted of watery stool. An improvement consisted of a change from a constipated stool to stool with normal consistency. Stool frequency was defined as the maximum number of stools reported per day over the observed period as described in the patient's diary. Secondary endpoints were changes in pain during defecation, need for rescue medication, parents' satisfaction with treatment, and parents' willingness to continue formula beyond seven days. At day 7, complete responders were infants achieving both primary endpoints, i.e. improved stool consistency and increased stool frequency; partial responders were infants achieving either of the primary endpoints; and non-responders were infants not achieving either of the primary endpoints. At day 29, complete responders were infants sustaining both the primary endpoints (having achieved both endpoints at day 7); partial responders were infants achieving either of the primary endpoints (irrespective of having achieved either of the endpoints at day 7); and non-responders were infants not achieving either of the primary endpoints.
Statistics
Descriptive analysis using counts and percentages was performed for primary and secondary study endpoints for the full analysis set population, which included all randomized patients receiving at least one dose of formula. For percentage calculations, patients with missing information relating to the study endpoints were not included in the denominator. Missing data were treated as missing, no imputations were performed. Differences between the treatment groups were analyzed using χ2 or Fisher's exact tests for categorical variables and 2-sample t-test for continuous variables. Statistical analysis was performed using SAS software (version 9.4; SAS Institute, Cary, NC, USA).
Sample size
To detect a difference of 20% between the 2 treatment groups for both the primary endpoints with 80% power and 5% 2-sided significance level, a sample size of 128 patients were required in each group, assuming an efficacy rate of 40% in the control group. We considered a dropout rate of 10% and concluded that 142 patients needed to be included in each treatment group.
RESULTS
Patients
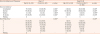
A total of 286 patients were recruited between December 2016 and October 2017; one patient was withdrawn from the study prior to receiving treatment due to possible lactose intolerance and was excluded from the analysis. The reasons why a small number of infants (n:7) were lost to follow-up are unknown. No significant differences with respect to baseline characteristics were found between the 2 groups (Table 2). Seven patients were lost to follow-up at the day 8 visit (Fig. 1). Final analysis of the 285 randomized patients receiving at least one dose of formula was undertaken: 143 patients (53.9% male; median [standard deviation; SD], age 6.1 [3.43] months) in the Mg-rich group and 142 (47.2% male; median [SD], age 5.2 [2.95] months) in the control group.
Table 2
Patient demographics and baseline characteristics

Data are presented as mean±standard deviation or number (%) unless specified.
Mg: magnesium.
The p-values calculated using *χ2 test; †Fisher's exact test; ‡2-sample t-test.
![]()
 | Fig.1Study participants.
*One patient was withdrawn from the study prior to receiving treatment due to lactose intolerance; †Five patients in the control group were lost to follow-up after their day 8 visit due to the absence of improvement in their condition reported at their day 8 visit; ‡Two patients in the Mg-rich formula group were lost to follow-up after their day 8 visit as the patients were traveling.
|
Stool consistency and frequency
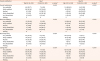
Normal stool consistency was significantly more common in the Mg-rich group (n=117, 81.8%) compared to the control group (n=58, 41.1%; p<0.001) at day 7 after initiation of treatment (Table 3). Similarly, at day 29, normal stool consistency was more common in the Mg-rich group (n=135, 95.7%) compared to the control group (n=89, 65.0%; p<0.001).
Table 3
Stool consistency and frequency throughout the study in the treatment groups
Values are presented as number (%). For percentage calculations, patients with missing information were not included in the denominator.
Mg: magnesium.
*Stool consistency was reported as per a pre-specified stool scale wherein constipation was defined as pellets/separate hard lumps like nuts or sticky dough-like consistency; normal stool was defined as a soft stool with a smooth consistency. Stool consistency type represents at least 1 report of a type of consistency over the observed period; patients can report more than 1 consistency type over the observed period, therefore types are not mutually exclusive; †Stool frequency is the maximum number of stools reported per day over the observed period; ‡The p-value has been calculated by the χ2 test; §The p-value has been calculated by the Fisher's exact test.
![]()
Stool frequency was also greater in the Mg-rich compared to the control group (p<0.001) at day 7 after initiation of treatment, with 124 (86.7%) infants fed Mg-rich formula having passed one or more stools per day compared to 96 (68.1%) infants fed the control formula (Table 3). Similarly, at day 29, stool frequency was greater in the Mg-rich group compared to the control group (p<0.001), with 140 (99.3%) infants fed the Mg-rich formula having a stool frequency of one or more stools per day compared to 128 (93.4%) infants fed the control formula. None of the children presented with large diameter stools.
Greater numbers of complete responders to treatment (i.e. infants with improved stool consistency and increased stool frequency) were observed in the intervention group at day 7 (n=38, 26.6%; control n=6, 4.3%; p<0.001) and day 29 (n=36, 25.5%; control n=5, 3.7%; p<0.001) following treatment (Fig. 2). Numbers of complete or partial responders to treatment were greater in the Mg-rich formula group (n=116, 81.1% vs. n=89, 63.1%) at day 7.

Change in pain during defecation
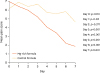
The enhanced decrease in mean pain score was observed over the first 7 days of treatment in the Mg-rich group (day 0: 6.97; day 7: 1.86; mean change: –4.85) compared to the control group (day 0: 6.17; day 7: 4.65; mean change: –2.30). Significant differences between the groups were observed from day 3 of treatment (Fig. 3).
Need for rescue medication
Rescue medication was required in the first 7 days following initiation of the different formula for 5 infants in both the groups (3.50% intervention group; 3.52% control group). Rescue medications received were specified in nine of the ten infants: lactulose (n=1) and glycerin suppositories (n=8).
Parent satisfaction with treatment
Overall satisfaction, as shown in Table 4, was significantly higher in the intervention group (32.2% very satisfied) compared to the control group (4.9% very satisfied) after 7 days. Satisfaction in terms of stool consistency, stool frequency, and crying time were all significantly higher in the intervention (35.7%, 34.3%, and 36.4% very satisfied, respectively vs. 3.52%, 8.45%, and 4.93% very satisfied, respectively). Similarly, at day 29, overall satisfaction was significantly higher in the Mg-rich formula group (80.9% very satisfied vs. 10.2%). Satisfaction in terms of stool consistency, stool frequency, and crying time were all significantly higher in the treatment group (80.1%, 72.3%, and 72.3% very satisfied, respectively vs. 18.3%, 6.57%, and 11.0%, respectively). There was no difference in intake between both the groups, resulting in a comparable, normal weight gain. In both groups, adverse effects were not observed.
Table 4
Parent satisfaction with treatment
Values are presented as number (%). For percentage calculations, patients with missing information were not included in the denominator.
Mg: magnesium.
*The p-value has been calculated by Fisher's exact test.
![]()
Parents willingness to continue the formula
After 7 days of treatment, 99.3% (n=142) of parents in the intervention group were willing to continue formula treatment compared to 95.8% of parents in the control group (p=0.07). However, after 29 days of treatment, almost all the parents were willing to continue with the Mg-rich formula (n=138, 97.9% vs. n=72, 52.6%; p<0.001) in the control group.
DISCUSSION
The present study clearly shows that the Mg-rich formula significantly improved stool consistency and increased stool frequency in constipated and young infants compared to the control formula after 7 days of intake and the observed differences were maintained over a period of 30 days. Over a period of 7 days, more than a quarter of patients were complete responders, i.e., having both improved stool consistency and increased stool frequency, while a further 55% were partial responders. A reduction in pain during defecation, high level of parent satisfaction with treatment, and willingness of parents to continue with the treatment were also observed. The Mg-rich formula ensures a Mg intake of 12.8 mg per 100 kcal which is in line with the European Regulation (Directive 2006/141/EC), the maximum level of Mg in infant formula being 15 mg per 100 kcal.
This study provides daily practice information regarding the efficacy of the Mg-rich infant formula in constipated infants across the Middle East by confirming the data obtained with the same formula in Taiwan [24]. A major study limitation of this study is the presence of potential bias in the estimation of treatment effect resulting from the open-label nature of the study.
A randomized controlled trial conducted in Taiwan demonstrated a reduction in constipation symptoms with use of the presented formula in a group of 93 formula-fed infants aged 2–6 months of age [24]. Furthermore, the same formula was also reported to reduce constipation in 91.6% of children in an observational multicenter study conducted in Spain involving 604 constipated infants younger than 5 months of age [25]. Finally, another study conducted in Spain including 30 constipated infants aged 4–10 weeks demonstrated that a two-week treatment with the same formula resulted in the greater water content of feces and improvement in the passage of stools [26].
Studies have demonstrated that the inclusion of nutritional compounds such as fatty acids, saccharides, proteins, and probiotics may improve symptoms of constipation. The addition of prebiotic oligosaccharides, palmitic acid, and partially-hydrolyzed whey in infant formula resulted in softening of feces but without any change in the frequency of defecation [27]. The addition of prebiotics such as galactooligosaccharides and fructooligosaccharides to infant formula promote the growth of healthy bacterial species, Bifidobacteria and Lactobacilli, within the digestive tract which induces softer feces in healthy infants [28-34]. Administration of probiotics, such as Lactobacillus reuteri, in infants with constipation, has been shown to increase the frequency of stools but without any change in consistency of stools [35]. Although there is no evidence that a partial hydrolysate and prebiotic oligosaccharides are effective in infants with constipation, there exists evidence that they soften the stools in non-constipated infants and increase stool frequency [3036].
This study provides important information regarding the effectiveness of the Mg-rich infant formula in a large group of infants. The study had an interventional design with patients randomized to either of the treatment group and the presented approach enables control over the confounders and results in comparable baseline characteristics between the 2 groups. Use of the Rome IV criteria, although modified for use in young infants, provides a robust measure of constipation treatment which is comparable to other studies.
In conclusions, the Mg-rich formula improved stool consistency and increased stool frequency in a group of constipated infants aged 6 months or younger compared to a control formula containing a lower amount of Mg, albeit containing oligosaccharides and a partial whey hydrolysate. The Mg-rich formula provides a solution for infants with functional constipation, which might reduce the need for rescue medication, use of oral laxatives, or suppositories for disimpaction. The findings of his study are in agreement with a recent consensus that reassurance and dietary treatment should be recommended as first-line management in infants with functional gastrointestinal disorders [37].
 XML Download
XML Download