

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Esophagogastroduodenoscopy (EGD) is a technique commonly used worldwide for both diagnosis and treatment in pediatric gastroenterology. Although EGD can be performed without sedation in adults, it is usually performed under anesthesia or deep sedation in children [12]. EGD is an invasive procedure that causes anxiety and discomfort in both children and their families. Various sedative agents have been used to reduce endoscopic procedure-related pain and anxiety in children [3]. However, there is no ideal agent with minimal side effects providing optimal comfort for both patients and endoscopist.
Propofol is a sedative-hypnotic drug with rapid onset and a short recovery time easily permitting an appropriate level of sedation [456]. Although it is widely used by anesthesiologists, it can lead to hypotension and respiratory depression when used at high doses [7]. In addition, there is no pharmacological antagonist available for recovery from its adverse effects [8].
Midazolam, a benzodiazepine, is used safely in EGD procedures in children [9]. It exhibits sedative, hypnotic, anxiolytic, and anticonvulsant activities, and also gives rise to anterograde amnesia and possesses muscle-relaxing effects. Midazolam is preferred for endoscopic procedures because it is short-acting and has a better pharmacokinetic profile than other benzodiazepines [1011]. An antidote to midazolam for recovery from its drug effects is also available [11].
The most comfortable and also the most reliable sedation regimen in EGD procedures in children is still the subject of debate. A propofol-midazolam combination is one regimen frequently used for this purpose. Diagnostic EGD procedures are shorter than those performed for therapeutic purposes or colonoscopy procedures. The long-lasting sedative effect of midazolam may, therefore, be less useful in EGD procedures performed for diagnostic purposes in children. The purpose of this study was to compare the use of propofol alone with the efficacy and safety of a propofol-midazolam combination in diagnostic EGDs in children and to identify the most suitable sedation protocol.
MATERIALS AND METHODS
The endoscopic charts of children aged 4 to 17 years undergoing diagnostic EGDs with a propofol-midazolam combination (group A) or with propofol sedation only (group B) at the Pediatric Gastroenterology Department of the Kanuni Training and Research Hospital in Turkey between January 2015 and June 2017, were retrospectively reviewed. Demographic characteristics, vital signs, medication dosages, induction times (defined as the time in minutes from the administration of propofol to the start of the procedure), sedation times (defined as the time in minutes from the start until the termination of the procedure), recovery times (defined as the time elapsed from the end of the procedure to discharge), and any complications observed were examined. This study was conducted according to the principles of the Declaration of Helsinki after approval by the Local Ethics Committee (Registry URL: 2017/42, Identifier: Trabzon Kanuni Training and Research Hospital Clinical Research Ethics Committee).
All procedures were performed within the endoscopy unit by a pediatric endoscopist specialist (Ulas Emre Akbulut) accompanied by an endoscopy nurse (Hulya Kirci). Parental consent was obtained before every procedure. All sedation procedures were performed by experienced anesthesiologist specialists. Our unit does not administer propofol sedation to children with metabolic or neurological diseases or if the anesthesiologist considers that such sedation is inappropriate for the patient. In addition, patients undergoing therapeutic or urgent endoscopies and American Society of Anesthesiologists physical status of 3 or more were not included in this study [12]. All procedures were carried out using an Olympus GIF-H180 device (Olympus Corporation, Tokyo, Japan) with the patient in the left lateral position. Post-procedural follow-up was carried out by a different nurse in the recovery room.
Endoscopic procedures were performed without tracheal intubation. Following a six-hour fasting period, 10% lidocaine spray (Xylocaine spray; AstraZeneca, Silk Rod, UK) was administered to the patient's pharynx in order to minimize procedural pain and discomfort [13]. Oxygen saturation, blood pressure, heart rate, and modified Ramsay Sedation Scores (RSS) were monitored continuously during the procedure and recorded by the anesthesiologists. Oxygen (2 L/min) was administered to all patients during the procedure through a nasal cannula. Major sedation-related complications were defined as cardiac arrest, apnea, and laryngospasm, while minor complications included desaturation, tachycardia, bradycardia, hypotension, arrhythmia, increased oral secretions, flushing, coughing, and vomiting. Desaturation was defined as oxygen saturation below 90% over a period of 30 seconds. Tachycardia was defined as heartbeats 30% above the average for the child's age, bradycardia was defined as heartbeats 30% below the average for the child's age, hypotension after sedation was defined as a decrease in arterial pressure of 20% from baseline values, and increased oral secretions were defined as abundant secretions necessitating suctioning. RSS values from 1 to 6 were based on the subject's response to stimuli (Table 1). Scores of 5 or more indicated sufficient sedation [14]. We also evaluated the endoscopist's satisfaction level using a numeric analog scale (0–10). Scores of 0 to 3 were considered unsatisfactory, 4 to 6 as average, and 7 to 10 as satisfactory.
Table 1
Ramsay scale for the assessment of sedation levels

![]()
Consistent with our unit's standard protocol, an initial intravenous (0.05 mg/kg, maximum 4 mg) bolus dose of midazolam (Zolamid, 1 mg/mL, 5 mL; Defarma Holding, Ankara, Turkey) was administered three minutes prior to propofol administration in the midazolam-propofol group. Propofol (1% propofol, 20 mL; Fresenius Kabi Deutschland GmbH, Bad Homburg, Germany) was administered to both groups in the form of a 1 mg/kg bolus dose by an anesthesiologist. Patients' responses to verbal and tactile stimuli were assessed one minute following propofol administration. In the event that adequate sedation was not established, 0.5 mg/kg propofol was administered at one-minute intervals. Endoscopy procedures were initiated by the endoscopist once no response was observed. Additional doses of propofol were administered if the patients were agitated once the procedure commenced.
Recovery was assessed using modified Aldrete scores from 0 to 10 based on the patient's activity, oxygen saturation, consciousness, respiration, and circulation [15]. Subjects with Aldrete scores of 9 or more were discharged from the endoscopy unit. Complications occurring during recovery, such as agitation, hallucinations, double vision, dizziness, and nausea, were recorded.
The data were analyzed with SPSS 13.0 (SPSS Inc., Chicago, IL, USA) software. Descriptive data were expressed as the median (range) and mean±standard deviation (SD). Normally-distributed variables between the two groups were compared using the independent paired samples t-test, while non-normally distributed variables were compared using the Mann-Whitney U test. The chi-squared test was used to compare categorical variables. The p-values <0.05 were considered to be statistically significant.
RESULTS
Two hundred forty-one diagnostic EGD procedures using a propofol-midazolam combination or propofol sedation only were performed in our hospital's endoscopy unit during the study period. Thirty-six patients were excluded from the study due to unavailability of data (n=22) or the presence of metabolic or neurological diseases (n=14). Two hundred and five patients were finally enrolled (105 in group A and 100 in group B). The median age of the patients was 14 years (range, 4–17 years; mean±SD, 12.81±3.41 years) and the median weight was 47 kg (range, 15–116 kg; mean±SD, 46.37±17.89 kg). The most common indication for endoscopy was chronic abdominal pain (51%). The demographic characteristics of the two groups are presented in Table 2.
Table 2
Patient characteristics
![]()
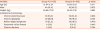
Induction times, sedation times, recovery times, sedative drugs dosages, numbers of propofol booster injections administered, RSS, and endoscopist satisfaction in the two groups are presented in Table 3. The median endoscopic procedure time was four minutes (range, 3–10 minutes; mean±SD, 3.79±1.05 minutes). No significant differences were observed between the two groups in terms of induction times, sedation times, recovery times, RSS, or endoscopist satisfaction. In addition, no differences were found between the mean propofol doses and the number of propofol booster injections.
Table 3
Evaluation of patients during and after endoscopy

![]()
No major procedural complications, such as cardiac arrest, apnea, or laryngospasm, occurred in any case. However, minor complications developed in 22 patients (10.7%), 17 (16.2%) in group A and five (5.0%) in group B (p=0.010). Desaturation was observed in seven patients (6.7%) in group A but none in group B. Oxygen saturation in those seven patients improved rapidly following the administration of additional oxygen (4–6 L/min) and airway positioning. Systolic arterial pressure decreased a maximum of 10% but none of our patients met the criteria for hypotension. None of our patients suffered from arrhythmia during or after sedation. Increased oral secretion was observed in four (3.8%) patients in group A. Although this presents a risk for aspiration and laryngospasm, these did not occur in any of our patients. No procedures were terminated due to insufficient sedation or complications. One hundred sixteen patients (56.6%) developed complications during the recovery period. We found no significant difference between the two groups in terms of recovery period complications. Dizziness was identified as the most common complication (in 90 patients, 43.9%). However, no serious complications, such as emergence reactions (severe agitation in the form of nightmares and delirium), occurred during the recovery period. Sedation-related complications are shown in Table 4.
Table 4
Complications in the 2 groups

Values are presented as mean±standard deviation (range) or number (%). Statistically significant p-values are shown in bold.
N.A.: not applicable.
![]()
DISCUSSION
This retrospective study compared the efficacy and safety of the use of propofol alone with a propofol-midazolam combination in children undergoing diagnostic EGDs. While no difference was determined between the two regimens in terms of efficacy, more periprocedural complications occurred with the propofol-midazolam combination.
Sedation is required for EGD procedures in children in order to reduce potential pain and to establish optimal comfort and cooperation [2]. Propofol-based sedation is a particularly reliable and effective option during pediatric gastrointestinal endoscopic procedures [2716]. Unconsciousness occurs within 30 to 60 seconds and the recovery time is also very short [1017]. However, propofol can lower systemic vascular resistance, cardiac contractility, and cardiac outflow. In high doses, it can cause respiratory depression [71819]. The lack of an antidote to reverse these side-effects is another cause of concern with propofol use [810].
Propofol is used in combination with other sedatives in order to permit administration in lower doses and thus, reduce potential complications [1620]. Midazolam is administered in combination with propofol to permit the effective use of propofol at smaller dosages [2122]. Disma et al. [18] showed that midazolam use together with propofol in EGD procedures in children reduced the propofol dosage. We, too, anticipated that the addition of midazolam would reduce the propofol used to a minimum dose. However, we observed no decrease in the number of additional injections of propofol with the addition of midazolam. Additional propofol injections were administered to approximately half the patients in each group. Additionally, there was no difference between the groups in terms of endoscopist satisfaction and RSS. Although the difference was not statistically significant, endoscopist satisfaction scores were generally higher in the propofol only group. The sedation time was also similar in both groups, at less than 4 minutes. Recovery time was also similar, at approximately 30 minutes in both groups. The lack of benefit from the addition of midazolam may be attributed to the relatively short sedation time in diagnostic EGDs.
Another interesting finding of our study was that more complications were observed in the group receiving midazolam during the procedure. While no desaturation occurred in the group receiving propofol alone, desaturation was observed in seven (6.7%) patients in the midazolam-propofol group. However, desaturation improved following airway positioning and the administration of additional oxygen and the procedures were successfully completed. In addition, no major side effects occurred. Although midazolam can be safely used in children, it can also lead to respiratory depression [23]. Lamireau et al. [24] reported a high level of desaturation in children undergoing EGDs with midazolam sedation. Midazolam increased the inhibitory effect of gamma-aminobutyric acid by binding between the alpha and gamma subunits present on the acid receptors [25]. Intravenous midazolam may cause respiratory depression due to direct suppression of the central respiratory drive, rather than as a result of simultaneous depression of the respiration muscles [26].
There were some limitations to this study showing that propofol alone exhibited similar efficacy as the midazolam-propofol combination in diagnostic EGD procedures in children. The first one was the retrospective nature of the study. Secondly, the study only considered diagnostic upper gastrointestinal endoscopic procedures. The brief sedation time may account for the lack of difference observed between the two groups. The drug dosages employed may also not be sufficient for therapeutic procedures. Patients under four years were excluded from the study. It was, therefore, not possible to consider potential complications in a younger age group, particularly in subjects under one year of age. Finally, this study was conducted in a single center and it is possible that the results might have been affected by factors, such as the nature of the endoscopist or nurse training. Further multicenter studies would be required in order to clarify this.
In conclusion, our study findings showed that the use of propofol alone as a sedative in diagnostic EGD procedures in children provided high endoscopist satisfaction and procedural comfort, together with a low-level side-effect profile. The administration of midazolam conferred no additional benefit in propofol-based sedation. Further studies are now needed to assess the efficacy of this sedation regimen in younger age groups and for therapeutic purposes and colonoscopy procedures.
 XML Download
XML Download