

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Malignant brain tumors are accompanied by hypercoagulability. Glioblastoma multiforme (GBM), the most common primary tumor of the central nervous system (CNS), is associated with heightened coagulation and venous thromboembolism (VTE). The circulating substance inducing the hypercoagulability is uncertain. Anticoagulants are frequently administered to GBM patients, although these agents increase the risk of intracerebral hemorrhage [1].
VTE is a common complication in patients with glioma [2]. VTE may be a prognostic factor for these patients [3].
Thrombin, an enzyme in blood plasma, causes the clotting of blood by converting fibrinogen to fibrin. In lower grade gliomas, thrombin has multiple effects. Intracerebral infusion of argatroban, a specific thrombin inhibitor, reduces brain edema and neurologic deficits in a rat glioma model. Thrombin immunoreactivity is found in cultured rat glioma cells and human glioblastoma. In addition, thrombin induces glioma cell proliferation in vitro; whereas argatroban reduces glioma mass [4].
Another clotting factor, von Willebrand factor (VWF), is a highly adhesive procoagulant molecule that mediates platelet adhesion to endothelial and subendothelial surfaces. Normally VWF is expressed exclusively in endothelial cells and megakaryocytes. However, a few studies have reported VWF detection in cancer cells of non-endothelial origin, including osteosarcoma and glioma [5]; and VWF is a prognostic factor in GBM [6].
In the current analysis, we examined The Cancer Genome Atlas (TCGA) data to assess the VWF gene in patients with lower grade gliomas.
MATERIALS AND METHODS
For newly diagnosed gliomas, we evaluated the association between VWF and overall survival in the Genomic Data Commons (GDC) TCGA Lower Grade Glioma (LGG) dataset in TCGA. To access and analyze the data we used:
GDC Data Portal (https://portal.gdc.cancer.gov/);
UCSC Xena browser (https://xenabrowser.net);
Oncomine (https://oncomine.org);
cBioPortal (http://cbioportal.org).
Survival data of the glioma subgroup were extracted for analysis and generation of Kaplan-Meier curves for overall survival. The optimal cutoff was identified by methods described in the R2 web-based application (http://r2.amc.nl); the method divides the sample, ascending order gene expression, into equal-sized groups. Further details have been published [7].
Gene expression is quantitated as Fragments Per Kilobase of transcript per Million mapped reads upper quartile (fpkm-uq), which is an RNA-Seq-based expression normalization method [8].
Simple statistics were calculated to identify patterns of mutual exclusivity or co-occurrence of mutations. For each pair of query genes (e.g., VWF and ATRX), an odds ratio (OR) is calculated (Equation 1) that indicates the likelihood that the mutations in the two genes are mutually exclusive or co-occurrent across the selected cases:
where A=number of cases altered in both genes; B=number of cases altered in VWF but not ATRX; C=number of cases altered in ATRX but not VWF; and D=number of cases altered in neither gene. Each pair was then assigned to one of five categories indicative of a tendency toward mutual exclusivity, of a tendency toward co-occurrence, or of no association. To determine whether the identified relationship is significant for a gene pair, Fisher's exact test was performed [9].
RESULTS
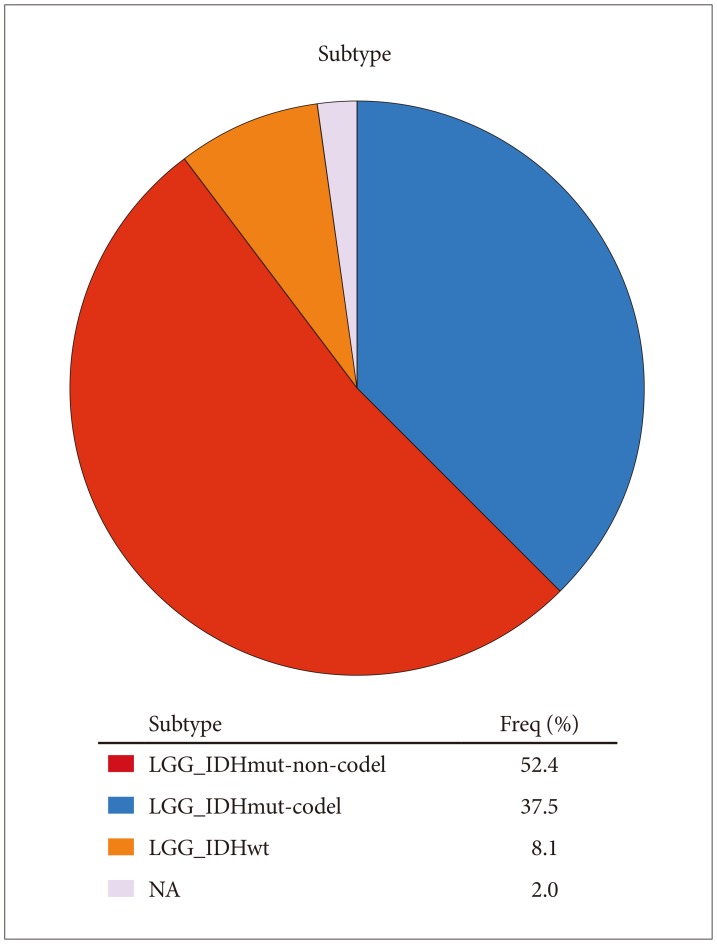
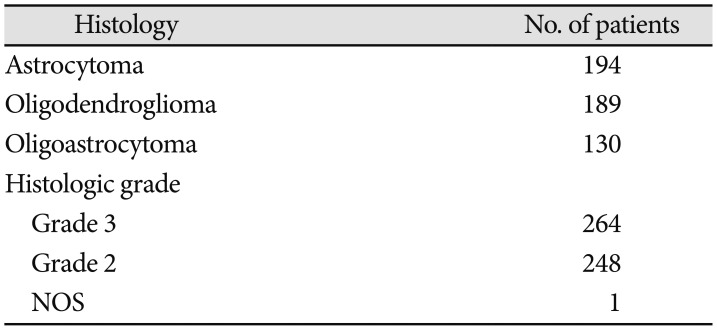
We analyzed data from 513 patients with primary lower grade glioma. The patients' mean age was 43±14 years (mean±SD). 55% of the patients were male, 45% female. 92.1% were white, 4.1% African-American, 1.6% Asian, 0.2% American Indian or Alaska native, 1.9% unclassified. Mean survival was 7.8 years. Histology and histologic grade are shown in Table 1. Molecular subtype information [10] is in Fig. 1.
VWF was significantly overexpressed in lower grade gliomas, especially in astrocytomas (p=0.008, t=2.471, Fold Change: 1.084, data from RefSeq Genes, UCSC refGene, July 2009, hg18, NCBI 36.1, March 2006) (Fig. 2).
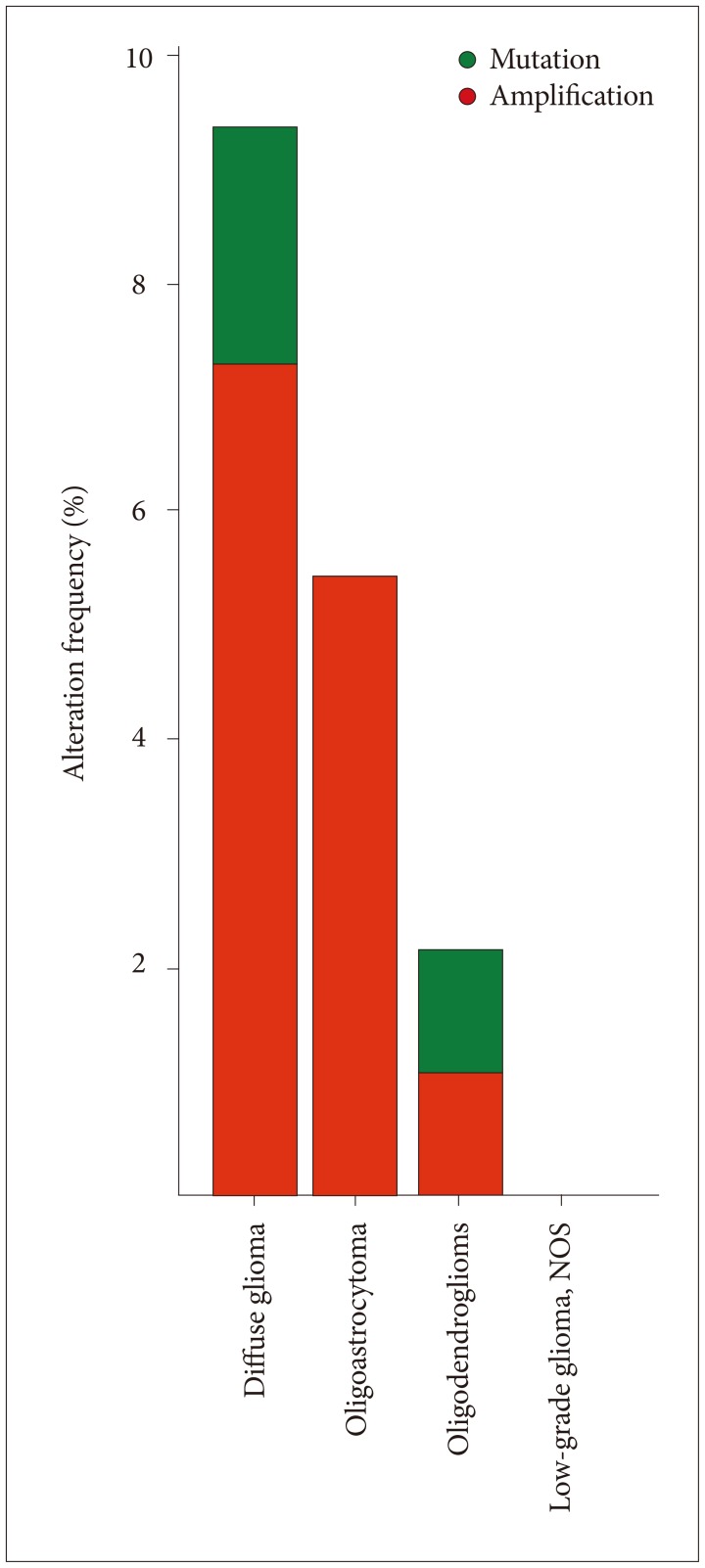
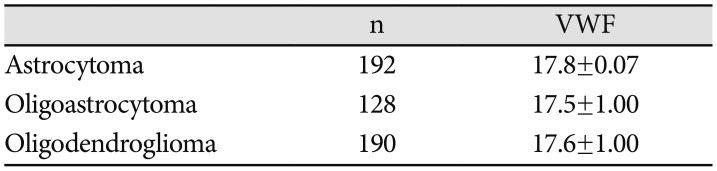
Histology of tumors and VWF expression in the current analysis are listed in Table 2. There was significant variability of VWF expression in astrocytomas, oligodendrogliomas and oligoastrocytomas (p=0.045, one way analysis of variance). VWF was most often mutated and amplified in diffuse gliomas (grade II gliomas, also known as diffuse low-grade glioma) (Fig. 3) [11]. A previous study suggested that percentage of VWF expressing tumor cells is higher in GBM and osteosarcoma than astrocytic tumors [5].
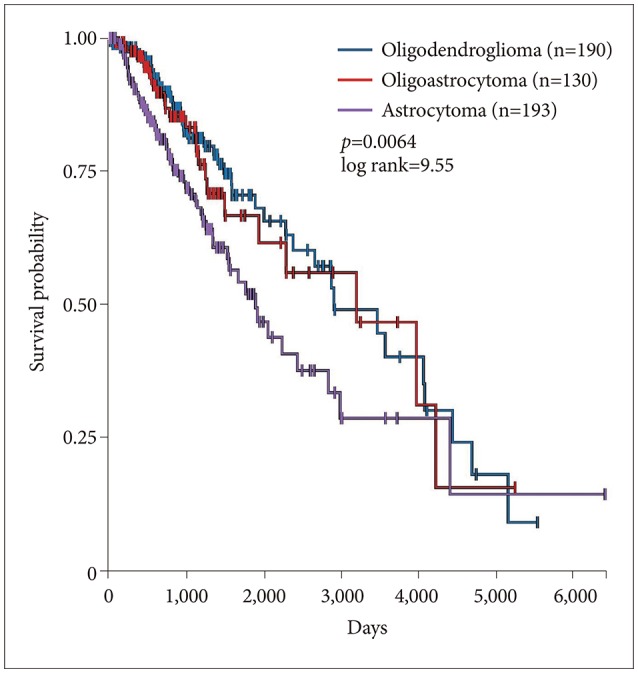
Survival of patients with astrocytomas was significantly worse than survival of patients with oligodendroglioma or oligoastrocytoma (p=0.0064, log rank test) (Fig. 4). Note that in the 2016 CNS WHO classifications, oligodendrogliomas must carry both an isocitrate dehydrogenase (IDH) mutation and a 1p/19q codeletion. Gliomas with an IDH mutation but intact 1p/19q genomic regions are classified as astrocytomas, as are those that lack an IDH mutation [1213]. Much of the TCGA data we present and analyze here was collected before the 2016 WHO classification change.
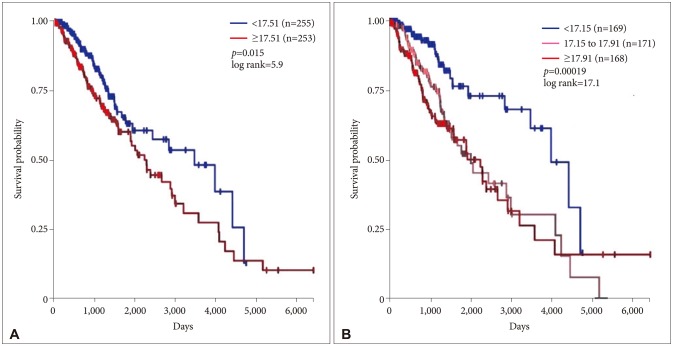
Survival versus VWF gene expression is shown in Fig. 5. Lower grade gliomas with less VWF gene expression had significantly better survival than those with more VWF gene expression (hazard ratio 0.64, 95% confidence interval 0.44 to 0.92, p=0.015 log rank test). The effect of VWF gene expression on survival was even more evident when the sample was analyzed as three groups (p=0.00019).
IDH1, TP53 and ATRX mutations are present in 40% or more adult lower grade gliomas [141516]. Among these tumors, as noted above, patients with astrocytomas have poorer survival than patients with oligoastrocytomas or oligodendrogliomas; prognosis of oligoastrocytomas or oligodendrogliomas is approximately equivalent. When we analyzed the data with Cox regression, VWF expression had a significant effect on survival (p=0.02) that was unrelated to the effect of IDH1 expression (p=0.062), TP53 expression (p=0.135), independent of ATRX expression (p=0.021) and histology (astrocytoma versus oligoastrocytoma and oligodendroglioma, p=0.002).
VWF mutations significantly co-occur with mutations in TP53 and ATRX (p<0.001) (Table 3, Fig. 6). The gene pair TP53/ATRX had 191 significantly co-occurrent alterations; the pair VWF/TP53 had 26 significantly co-occurrent alterations; the pair VWF/ATRX had 23 significantly co-occurrent alterations.
VWF is not an enzyme and its primary function is binding to other proteins, in particular Factor VIII. In addition, the destruction of VWF is largely mediated by the enzyme ADAMTS 13. Therefore, to address the effects of elevated VWF expression on the pathogenesis of thrombosis in lower grade glioma, we examined the expression of the related genes for Factor VIII and ADAMTS13. We found no correlation with VWF.
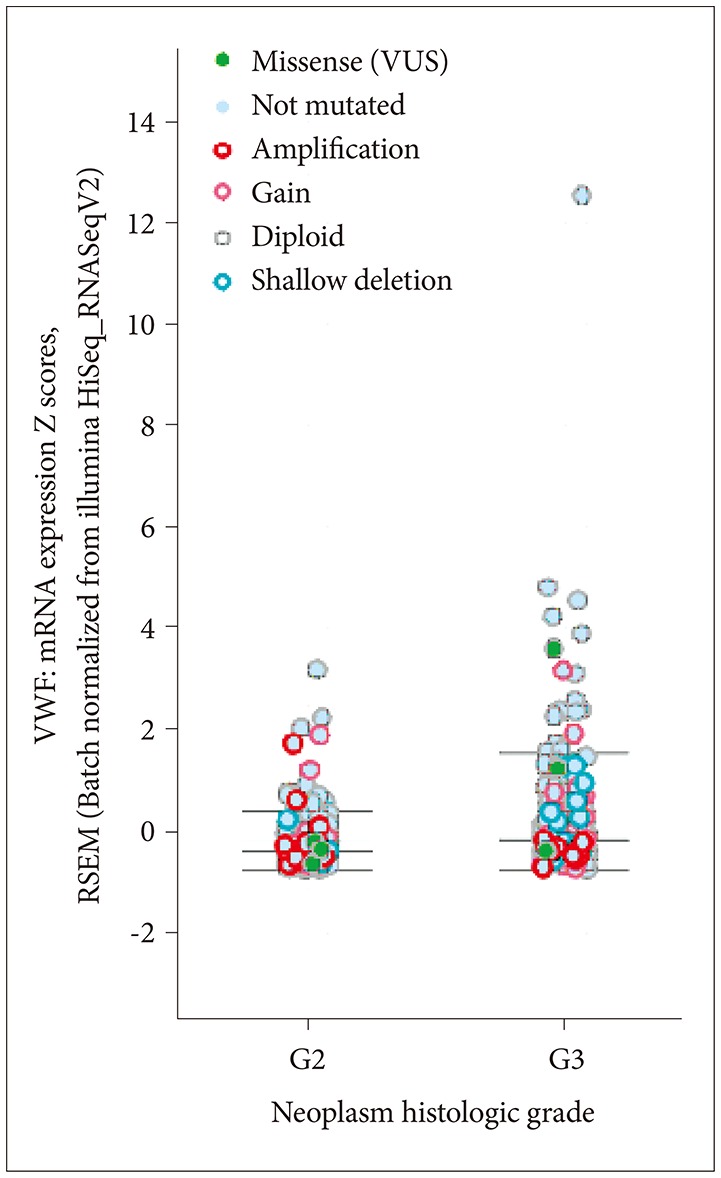
Lower grade gliomas include various types of tumors. IDH1 is the most frequently mutated gene, in about 80% of cases. IDH1 versus VWF mRNA expression by mutation status is shown in Fig. 7. The correlation is significant. Tumor grade and VWF mRNA expression by mutation status is shown in Fig. 8; grade 3 tumors have more mutations than grade 2.
DISCUSSION
Lower grade glioma is a uniformly fatal disease of young adults with survival averaging approximately 7 years [17]. Although lower grade glioma patients have better survival than patients with high grade (WHO grade III/IV) glioma, almost all lower grade gliomas eventually progress to high grade glioma and death. Data from the Surveillance, Epidemiology and End Results (SEER) program of the National Cancer Institute suggest that for the majority of lower grade glioma patients, overall survival has not significantly improved over the past three decades [17].
Multiple prognostic factors have been described: Tumor histology, grade, location, contrast enhancement, patient age, performance status, and seizure history [18]. Survival probability in patients with a glioma having a high median Tumor Blood Flow (mTBF) has been shown to be lower than in patients with a glioma having a low mTBF [19]. Recently, tumor genome has proven to be a prognostic factor [1415], as well as F13A1 copy number segments [20].
Armand Trousseau first reported the relationship of malignant tumors and coagulation in 1865. Trousseau diagnosed the syndrome in himself two years later, dying soon afterward of gastric cancer. Recent findings suggest that genetic pathways within tumor cells might trigger thrombotic phenomena, worsening prognosis [21].
Biological processes or pathways in cancer are often deregulated through different genes or by multiple different mechanisms. But cancer gene mutations usually do not occur at random. Mutations of certain cancer genes tend to co-occur, indicating that they may work in tandem to drive tumor formation and development [9]. This appears to be the case with the co-occurring VWF, ATRX, and TP53 mutations.
The deleterious prognostic effect of VWF expression in lower grade gliomas is not surprising, given its role in other cancers. VWF fibers promote cancer-associated platelet aggregation in malignant melanoma of mice and humans [22]; and cancer cell-derived VWF enhances metastasis of gastric adenocarcinoma [23].
An analysis of lower grade glioma in TCGA has shown IDH, 1p/19q, and TP53 status to be more indicative of prognosis than histologic class. Moreover, lower-grade gliomas with an IDH mutation either had 1p/19q codeletion or carried a TP53 mutation. Most lower-grade gliomas without an IDH mutation were molecularly and clinically similar to glioblastoma [16].
VWF gene expression may be another clinically important prognostic marker in lower grade glioma. The risk of VTE in glioma patients is high, and extends beyond the postoperative period. The procoagulant molecule tissue factor appears to play an important role, but other markers are needed [24]. VWF may represent a new marker. Though thromboembolic events lead to worse outcomes, risks of anticoagulant administration should be better defined. Further studies of VWF would be worthwhile.




 XML Download
XML Download