

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pituitary tumors constitute 10–15% of all primary intracranial neoplasms. Among sellar lesions, pituitary adenomas are the most frequent finding [1]. Surgical intervention is the first-line treatment for most patients with pituitary adenomas, with the exception of prolactinomas, in which dopamine agonists remain the best treatment option [2]. The endoscopic endonasal approach (EEA) is a minimally invasive surgical technique for the removal of sellar and parasellar lesions. It has been introduced over the last twenty years as an alternative to the traditional microscopic surgery [3]. EEA imparts superior exposure of the sella and the advantages include a wide panoramic view and enhanced visualization of relevant anatomical structures [4].
While the endoscopic approach has demonstrated a notable decrease in overall complication rate, the need for large dural openings and arachnoid can result in large skull base defects with moderate to high flow cerebrospinal fluid (CSF) leaks [567]. As a consequence of suprasellar extension distending the diaphragma sellae, postoperative CSF rhinorrhea is more common with resection of macroadenomas than microadenomas [8]. Complications involving CSF leakage can result in bacterial meningitis, pneumocephalus, and intracranial hypotension, and also increase hospital cost and length of stay [9].
It is recognized that success of the reconstruction method following dissection is a principal determinant of postoperative CSF leak incidence [10]. The introduction of pedicled, vascularized skull base repair, also known as the nasoseptal flap, is now widely used due to its versatility and capability of covering an area averaging 17.12 cm2 as determined by radiographic and anatomical studies [11]. In addition, it has dramatically decreased the incidence of postoperative CSF leaks following EEA, from more than 20% to less than 5%. This level is approximate to that of open cranial base surgery [121314].
In this study, we sought to investigate our institutional experience using pedicled nasoseptal flaps for reconstruction of the skull base after EEA where an intraoperative CSF leak was identified during resection of a pituitary tumor. We focused the study on postoperative complications, emphasized on approach-related factors related to these complications, and compared our experience with reports in the literature.
MATERIALS AND METHODS
Patient population
Under an IRB approved protocol (IRB #00092610), medical records of patients with a diagnosis of pituitary macroadenoma or microadenoma that subsequently underwent EEA resection were retrospectively reviewed from 2008 to 2015 at Johns Hopkins Hospital. The review included demographic, clinical, operative, radiographic, and pathological information.
Collected data
The following baseline admission data were collected: age, gender, race, common comorbidities, symptoms and signs at presentation, symptom duration (months), Karnofsky Performance Status (KPS) score, and follow-up time (months). These comorbidities included hypertension, diabetes mellitus, obesity, coronary artery bypass grafts/stents, sleep apnea, and coronary artery disease. Data collected on symptoms and signs included presence of headache, decreased vision, diplopia, gait and/or balance problems, nausea and/or vomiting, Cushing's syndrome, and cranial nerve deficits.
Preoperative and post-operative laboratory results were collected, consisting of serum prolactin, serum adrenocorticotropic hormone (ACTH), serum thyroid-stimulating hormone (TSH), serum free thyroxine 4 (T4), serum growth hormone, and serum cortisol levels. The timing between pre- and post-operative laboratory sample testing at our institution is between 24–48 hours. All aforementioned data was collected for each admission, if available. Number of admissions (n) is used to designate the total number of admissions with the data point in question used to calculate overall percentages. The closest available laboratory values to the date prior to surgery and following surgery were used as pre- and postoperative values. Radiologic data obtained included the largest dimension for each macroadenoma or microadenoma, as measured by MRI prior to surgery. In this study, microadenomas were defined as tumors measuring 10 mm or less, and macroadenomas as those exceeding 10 mm.
The primary outcome measure was the incidence of a postoperative CSF leak following surgery with use of a nasoseptal flap for skull base reconstruction. The incidence of intraoperative CSF leaks and post-operatively acquired diabetes insipidus was also recorded. At Johns Hopkins, there is a tertiary care referral practice for pituitary tumors which encompasses many difficult-to-resect tumors referred by other neurosurgeons (suprasellar extension, tumors adherent to the arachnoid, revision cases, and secreting tumors), which generally can result in higher CSF leak rates compared to published rates. All CSF leaks were reported, including pinpoint or extremely low flow leaks. Our institution does not have a specific grading system other than using pinpoint/low flow, moderate flow, or high flow (opening a cistern or ventricle).
RESULTS
Patient characteristics
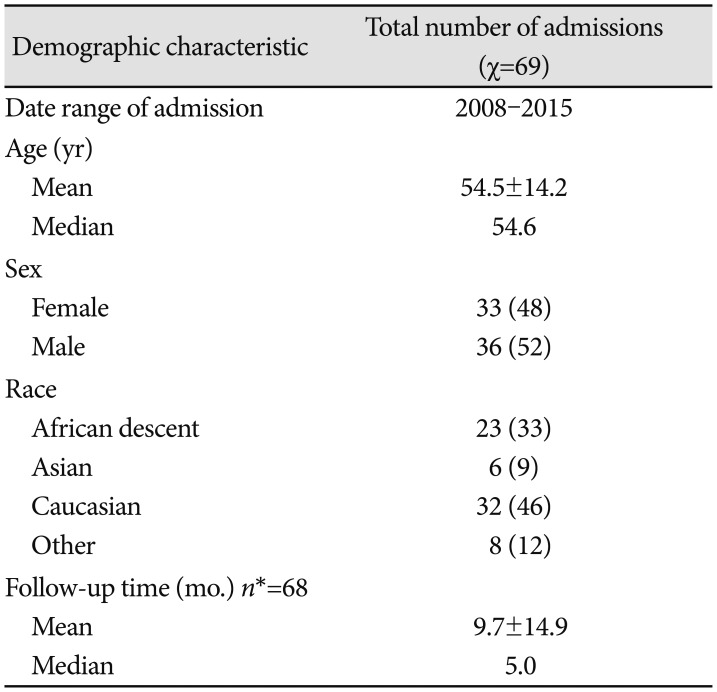
A total of 67 patients (69 hospital admissions) diagnosed with pituitary adenomas undergoing EEA surgical resection were identified (Table 1). The average age at time of surgery was 54.5 years (range 14–91), and the sex distribution was evenly distributed with 52% male and 48% female. There was a heterogeneous racial makeup patients, with 46% Caucasian, 33% of African descent, 9% Asian, and 12% belonging to other racial groups.
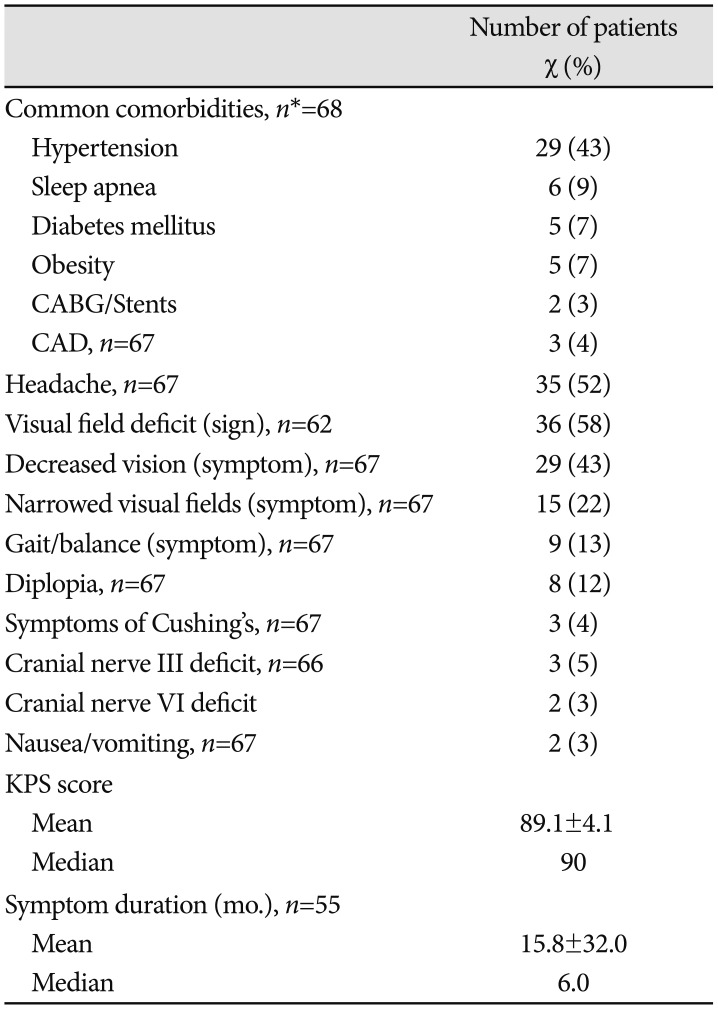
The most common comorbidity at presentation was hypertension, with 43% of patients, followed by sleep apnea (9%), diabetes mellitus (7%), and obesity (7%). 52% of patients presented with headache as a symptom, and 58% had a documented visual field deficit as determined by physical examination. The median symptom duration was six months, and the median KPS score was 90 (Table 2).
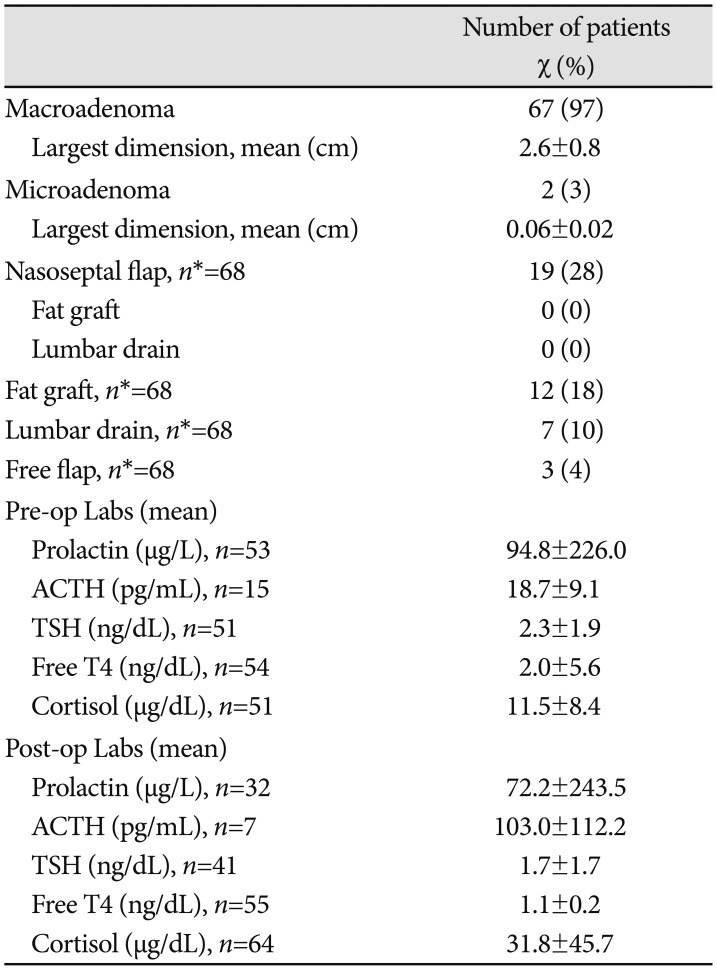
The majority (97%) of patients had a macroadenoma with a mean largest dimension of 2.6 cm (Table 3). Of all patients who underwent surgical resection, 28% had a nasoseptal flap, 18% had fat grafts and packing of the sella, 10% had a lumbar drain, and 4% had a free mucosal graft from the middle turbinate. Of those with nasoseptal flaps, 2% had accompanying fat grafts/packing, and none had a lumbar drain.
With reference to laboratory values, there was a remarkable mean decrease in prolactin levels preoperatively and postoperatively (94.8 µg/L vs. 72.2 µg/L). There was also a decrease in TSH levels, from 2.3 ng/dL to 1.7 ng/dL and in free T4 levels (2.0 ng/dL to 1.1 ng/dL). In contrast, there was a marked mean increase in ACTH (18.7 pg/mL vs. 103 pg/mL) and in cortisol levels (11.5 µg/dL vs. 31.8 µg/dL). The level of postoperative cortisol and ACTH were much higher than preoperative status. This increase may be correlated to the perioperative use of steroids, as well as the fact that hormones are highly susceptible to changes based on time of day in which labs are drawn.
DISCUSSION
The introduction of EEA for tumor resection has dramatically transformed the surgical treatment of complex pituitary pathologies. As a result, skull base tumors necessitating extensive resection with resultant dural defects led to the development of more robust repair techniques, including free vascular grafts, free synthetic non-cellular grafts, and vascularized pedicled nasoseptal flaps [11]. Regardless of the reconstructive technique applied, reviews indicate that postoperative CSF leak hovers at approximately 8.5% [15]. When the data are stratified for defect location, defect size, and degree of intraoperative CSF leak, the evidence demonstrates that vascularized reconstruction is super to avascular techniques. In a vast systematic review, Harvey et al. [16] analyzed 38 studies with 609 patients with large dural defects, in which approximately half underwent vascularized reconstruction and the other half underwent free graft reconstruction. This resulted in a statistically significant difference in CSF leak rate (6.7% vs. 15.6% respectively).
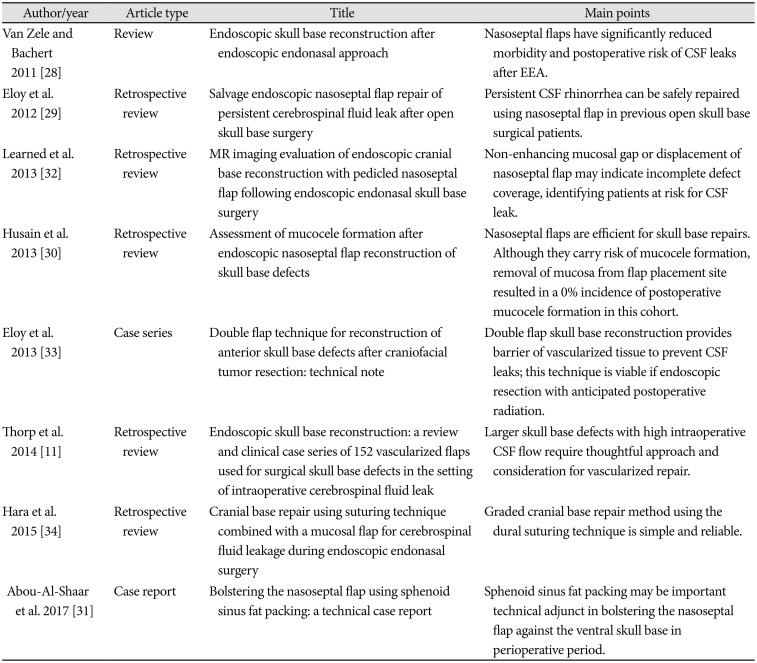
Nasoseptal flaps offer notable flexibility to the surgeon in skull base repair, and their potential to overlay such a significant area has led to its widely accepted use. It has been noted that in patients who experienced high intraoperative CSF flow, postoperative CSF leak rates remain at 5.7% with the use of a nasoseptal flap [17]. In addition, Thorp et al. [11] noted a 3.3% perioperative CSF leak rate and zero postoperative CSF leak rate among 152 vascularized flaps used for surgical skull base defects.
CSF fluid leakage can be categorized into low-flow type and high-flow type. Luginbuhl et al. [18] first described the term of “high-flow” leakage, which referred to regular CSF flow out intraoperatively due to a cisternal or ventricular opening defect. Low-flow CSF leaks have been previously defined as solely a few drops in the context of transitory increased intracranial pressure, such as coughing, standing up, or straining. The majority of CSF leakage following endoscopic sellar region surgery is low flow [19]. Lumbar drains are often applied intraoperatively, postoperatively, and on occasion even preoperatively to control or prevent CSF leaks, yet their placement remains controversial [202122].
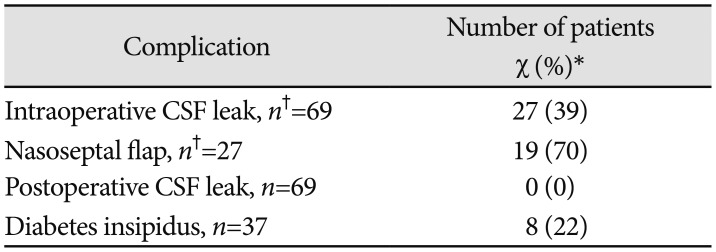
Our analysis of 69 hospital admissions revealed that the use of a nasoseptal flap for skull base reconstruction in EEA surgical resection for pituitary adenomas is effective at fixing intraoperative CSF leaks in the absence of a lumbar drain. Our results demonstrating no incidence of postoperative CSF leakage following use of a nasoseptal flap are also consistent with the existing neurosurgical literature. For patients who underwent an alternative form of repair, to include sphenoid fat packing and/or a lumbar drain, there were similarly no postoperative CSF leaks. This practice is well-documented and also in keeping with the literature on this topic [232425]. Fat grafts are generally not preferable to use in circumstances of intraoperative CSF leaks, as they can cause difficulty at re-operation, are challenging to follow-up via MRI, and can result in hydrocephalus in high flow leaks [2627].
Van Zele and Bachert [28] conducted a review of nasoseptal flap use for skull base reconstruction and determined that they are responsible for a significant reduction in risk and morbidity of postoperative CSF leaks following EEA. Eloy et al. [29] found that the integration of a vascularized pedicled nasoseptal flap to prevent persistent CSF rhinorrhea in patients who have undergone past open skull base surgery has the benefit of avoiding revision craniotomy whilst providing healthy tissue to reconstruct the skull base.
One concern during repair with a nasoseptal flap is that it may carry an innate risk of mucocele formation when deposited over mucosalized bone, and such it is important to meticulously remove all sellar and sphenoid mucosa before laying down a flap. However, Husain et al. [30] ascertained that strategic and diligent removal of the mucosa for the flap placement site produced a 0% incidence of postoperative mucocele formation in their cohort of 70 patients, and a 2.9% postoperative CSF leak rate. Furthermore, Abou-Al-Shaar et al. [31] reported on the use of sphenoid sinus fat packing during skull base reconstruction as a support to the nasoseptal flap. They determined that it may serve as a significant technical addition to sustain the nasoseptal flap against the ventral skull base during the early perioperative period.
In addition, Learned et al. [32] determined that EEA skull base reconstruction that employs a nasoseptal flap has a characteristic MRI appearance. Identifying patient at risk for CSF leaks can be accomplished via MRI, as a non-enhancing mucosal gap or displacement of the nasoseptal flap may indicate incomplete defect coverage [32].
In conclusion, the implementation of the pedicled nasoseptal flap for skull base reconstruction after EEA for resection of pituitary adenomas has resulted in a significant decrease in the incidence of postoperative CSF rhinorrhea. In this retrospective analysis, we present our institutional experience utilizing the nasoseptal flap and describe its effectiveness in preventing CSF leaks after EEA.
 XML Download
XML Download