

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Kap Jung Kim, M.D. , Kwang-Won Lee, M.D., Jong Shin Lee, M.D.
, Kwang-Won Lee, M.D., Jong Shin Lee, M.D.
, Kwang-Won Lee, M.D., Jong Shin Lee, M.D.
Abstract
Giant cell tumor is a benign but locally aggressive tumor with common recurrence. Most cases occur around the knee joint. Giant cell tumor of the foot is rare and very few cases involving the first metatarsal have been reported. Its characteristics and treatment in adult patients remain unclear. This paper reports a case of recurrent giant cell tumor at the first metatarsal that was excised surgically and subsequently reconstructed with non-vascularized fibula graft.
Figures and Tables
 | Figure 1(A) Plain radiograph showing an expansile and osteolytic lesion at the first metatarsal of the left foot. The lesion was multi-septated, lobulated, and combined with cortical thinning. Stress fracture of the fifth metatarsal neck area was also visible. (B) Computed tomography scan showing the entire expansive osteolytic lesion with marked cortical thinning of the peripheral shell and subtle cortical destruction of the first metatarsal. No transarticular extensions into the adjacent proximal phalanx and medial cuneiform bone were observed. (C) T1-weighted enhanced image of a coronal scan showing multiple septated, lobulated and osteolytic masses replacing the first metatarsal bone with multiple fluid-fluid levels. Each septum showed high signal wall enhancement and intermediate signal within each septum. Stress fractures with callus formation were also visible at the fifth metatarsal neck.
|
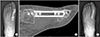
 | Figure 2(A) Intraoperative photograph showing an en-bloc excision of the first metatarsal through the previous incision. (B) Intraoperative photograph showing the non-vascularized fibula graft at the defect that was fixed with plates at both sides; medial cuneiform-fibula graft and fibula graft-proximal phalanx. (C) Postoperative plain radiograph showing a successful en-bloc excision of the recurrent tumor followed by nonvascularized fibula graft.
|
 | Figure 3(A, B) Plain radiograph and computed tomography scan showing good maintenance and incorporation of the graft between both sides at postoperative 6 months. (C) Plain radiograph showing implant removal at postoperative 18 months. Sound incorporations between the fibula graft and host bones (medial cuneiform and proximal phalanx) were visible.
|
References
1. Campanacci M, Baldini N, Boriani S, Sudanese A. Giant-cell tumor of bone. J Bone Joint Surg Am. 1987; 69:106–114.


2. Rajani R, Schaefer L, Scarborough MT, Gibbs CP. Giant cell tumors of the foot and ankle bones: high recurrence rates after surgical treatment. J Foot Ankle Surg. 2015; 54:1141–1145.
3. Siddiqui YS, Zahid M, Bin Sabir. Giant cell tumor of the first metatarsal. J Cancer Res Ther. 2011; 7:208–210.
4. Ly JQ, Arnett GW, Beall DP. Case 122: giant cell tumor of the second metatarsal. Radiology. 2007; 245:288–291.
5. Turcotte RE. Giant cell tumor of bone. Orthop Clin North Am. 2006; 37:35–51.
6. Murphey MD, Nomikos GC, Flemming DJ, Gannon FH, Temple HT, Kransdorf MJ. From the archives of AFIP. Imaging of giant cell tumor and giant cell reparative granuloma of bone: radiologic-pathologic correlation. Radiographics. 2001; 21:1283–1309.
7. O'Keefe RJ, O'Donnell RJ, Temple HT, Scully SP, Mankin HJ. Giant cell tumor of bone in the foot and ankle. Foot Ankle Int. 1995; 16:617–623.
8. Unni KK, Dahlin DC. Dahlin's bone tumors: general aspects and data on 11,087 cases. 5th ed. Philadelphia: Lippincott-Raven;1996. p. 263–283.
9. Balaji GG, Roy AC, Justin SV. Techniques in recurrent giant cell tumour of the first metatarsal in adolescents - A rare report of 2 cases. Foot Ankle Surg. 2013; 19:e1–e4.
 XML Download
XML Download