

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In pediatric dentistry, minimizing anxiety in children is an extremely challenging but is necessary. A child's cooperation with a dental procedure usually requires various behavioral management strategies conveyed by the entire dental team. If these strategies prove inadequate, the application of some form of pharmacological sedation or general anesthesia is indicated.
The benefits of administering general anesthesia must always be weighed against the risks. Its previously reported post-operative complications include arrhythmias, dislodged or obstructed endotracheal tube, IV infiltration or disconnection, edema of the tongue or lips, and nasal bleeding, which could range from negligible to severe (90%) [1]. However, nowadays, the rise of sedation, anxiety, and unwanted movement of children during dental procedures has markedly reduced [2]. Sedation depresses the level of consciousness but allows the patient to respond appropriately to verbal commands and light tactile stimulation [3]. In dentistry, it has been used in the treatment of children or adults with high anxiety levels, thus optimizing the success of dental procedures.
Currently used sedatives include midazolam, chloral hydrate, ketamine, nitrous oxide, promethazine, propofol, hydroxyzine, sevoflurane, and opioids. In pediatric sedation, these drugs have been administered alone or in combination, for decades. Despite their efficiency, associated adverse effects limit their use in pediatric dental procedures. Thus, the quest for a sedative that can provide minimal to moderate sedation in children is ongoing.
α2-ADRENORECEPTOR AGONISTS
1. Classification of α2-adrenoreceptor agonists
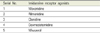
There are several α2-adrenergic receptor agonists, including clonidine, guanfacine, tizanidine, methyldopa, guanabenz, medetomidine, methyl norepinephrine, levonordefrin, and dexmedetomidine [4]. They can be classified as nonselective and selective α2-adrenoceptor agonists, based on their affinity to α2-adrenoceptors [5] (Table 1).
Dexmedetomidine is a short-acting central α2-adrenoceptor agonist with a ratio of selectivity of 32 and 1300 for α-2a-to-imidazoline and α-2a-to-α-1, respectively. Like mivazerol and clonidine, it has a strong affinity for α2-adrenoceptors. However, it also has a slight affinity for non-adrenergic imidazoline receptors [5] (Table 2). Eleven and twelve imidazoline receptor binding sites have been identified in the brain, and the pancreas and kidneys, respectively [5].
2. Dexmedetomidine
It has been reported that α2-adrenoreceptor agonists cause sedation, anxiolysis, analgesia, an antisialogogue effect, sympatholytic, and postoperative reduction of nausea and vomiting better than benzodiazepines. Orally and intranasally administered clonidine has a slow onset of action, resulting in a half-life of 12.5 h [67]. In children, its plasma concentration peaks 60–90 min post oral administration. Hence, clonidine needs to be administered at least 1 h before the induction of anesthesia [89].
Dexmedetomidine was first approved by the Food and Drug Administration in 1999 for the sedation of intensive care unit patients and for premedication. In 2005, it was introduced to dentistry [310]. Dexmedetomidine is a more selective and specific α2-adrenoreceptor agonist than clonidine [6]. Dexmedetomidine is 8 times more specific than clonidine and has a shorter half-life. Consequently, dexmedetomidine has more favorable pharmacokinetic properties than clonidine [37].
The properties dexmedetomidine include sedation, anxiolysis, and analgesia without significant respiratory depression [3]. These make it a preferable sedative in adult and pediatric dental procedures [11]. A few recent studies have investigated the various routes of administrating dexmedetomidine, and its safety and efficiency, to develop a protocol that results in minimal to moderate sedation in pediatric dental patients [12].
1) Chemical formula of dexmedetomidine
Dexmedetomidine is the dextrorotatory S-enantiomer of medetomidine chemically described as [+]-4-[2, 3-dimethylphenyl]ethyl-1H-imidazole monohydrochloride, with a molecular weight of 236 [13]. It is a highly selective and potent α2-adrenoceptor agonist [α2 : α1 magnitude relation = 1620 : 1]. Its empirical formula is C13H16HCl [1013] (Fig. 1).
2) Mechanism of action of dexmedetomidine
The central effect of dexmedetomidine is the inhibition of noradrenaline release by acting on the α2-adrenoceptors in the locus ceruleus. Thus, it produces a state similar to natural sleep, where the patient can be easily aroused by external stimulus [5]. Its primary mechanism of action is stimulation and cessation of parasympathetic and sympathetic outflows, respectively. Sedation is primarily induced by the activation of post-synaptic α2-adrenergic receptors. Because dexmedetomidine attaches to the α2 receptors of the locus ceruleus and spinal cord, it brings about effects such as sedation and analgesia [13]. Dexmedetomidine has a low affinity for beta muscarinic, adrenergic, serotonin, and dopaminergic receptors [13].
3) Pharmacodynamics and pharmacokinetics of dexmedetomidine
Dexmedetomidine is a potent drug; at plasma concentrations less than 1.0 µg, it can produce profound physiological alterations [5]. There are 3 subtypes of α2-adrenoreceptors: α2A, α2B, and α2C, with different pharmacological properties and physiologic functions. They are found within the blood vessels, vital organs, and the autonomic, peripheral, and central nervous systems. Dexmedetomidine binds to this G-Protein-coupled α2-adrenoreceptor. Its associated vagomimetic effects such as bradycardia and vasodilatation result from its high affinity to α2-adrenoceptors. Dexmedetomidine also displays a nonlinear concentration-dependent pharmacokinetic effect [5].
Dexmedetomidine has a distribution half-life of about 6 min and a terminal elimination half-life of about 2 h (2-compartment model). It has a quick onset and short duration of action. Dexmedetomidine is extremely lipophilic and about 94% protein bound. It is nearly completely biotransformed, and is excreted in feces (4%) and urine (95%) [13]. Biotransformation involves both direct glucuronidation (the major pathway) via direct N-glucuronidation, aliphatic hydroxylation (principally by CYP2A6), and N-methylation, as well as cytochrome P450 mediated metabolism [413]. Its metabolites are considered inactive and there is no chiral conversion to the levo-isomer.
4) Properties of dexmedetomidine
Dexmedetomidine exerts sedative, anxiolytic, and analgesic effects, with insignificant respiratory system distress [13]. It aids in the additional induction of anesthesia induced by other drugs and causes preoperative sympatholytic effects and hypotension, due to its stimulation of central α2 and imidazoline receptors. Unlike midazolam, other benzodiazepines and opioids, dexmedetomidine does not have an affinity for GABA or opioid receptors and does not result in respiratory depression. Thus, it creates a compliant and semi-arousable kind of sedation [4]. Also, its effects can be reversibly reversed by its specific antagonist atipamezole [13].
5) Advantages of dexmedetomidine
In 2002, Tobias et al. [14] stated that dexmedetomidine was a safe sedative for children and infants. It induces minimal respiratory depression and inhibits tachycardia [13]. During its sedative action, it prevents hypoxia by maintaining the airway and enabling spontaneous respiration. It also preserves CO2 reactivity and increase. Due to its low effect on respiratory function, dexmedetomidine could be a very valuable pediatric sedative [38].
6) Routes for administering dexmedetomidine for sedation
Dexmedetomidine can be administered orally, buccally, intravenously, intranasally, and intramuscularly (Table 3).
(1) Oral route
One of the simplest and popular routes for drug administration is the oral route. Its advantages include simplicity and ease of administration, affordability, risk free, and worldwide acceptance. In pediatric dental care, the ease of administration by this route makes it favorable. The rate of drug absorption via the oral mucosa is influenced by multiple factors, including the duration of its contact with the mucosa, its pKa, lipophilicity, quantity of saliva, and physiochemical characteristics at the site of action [1516]. At physiological pH, dexmedetomidine is present in a nonionized form and has a pKa value of 7.1. Being a highly lipophilic drug, it is easily transported into tissues [17].
Multiple studies have reported that in approximately 90 min post administration, it permeated the oral mucous, achieved a buccal bioavailability of 82%, and achieved its highest concentration [18]. However, the most widely used oral pediatric sedative, midazolam, is more lipophilic. At a pH of 4.0–4.5, the closing of its imidazole ring occurs. This high pH leads to its high lipid solubility in and fast absorption via the oral mucosa [19]. When 0.5 mg/kg midazolam is orally administered as a premedication, its mucosal absorption is likely to be reliant on its pH [6]. Some of the adverse effects associated with its 70% oral bioavailability include restlessness and postoperative respiratory depression [6].
It has been reported that the high hepatic first pass metabolism associated with oral drug administration is responsible for the low (16%) bioavailability of dexmedetomidine post oral administration, compared with 82% post buccal administration [1820]. As a result, the benefits of orally administered dexmedetomidine are low compared with those of midazolam [21]. Oral administration reportedly leads to few side effects such as gastric disturbances and change in taste, and shortcomings such as longer recovery time, high first pass metabolism, and slow onset of action [22].
Time of onset
Oral dexmedetomidine needs to be administrated at most 40 min before the induction of anesthesia, to attain the most favorable sedative effect. Previously, it has been demonstrated that with midazolam, moderate sedation is achieved about 20 min post administration [23].
(2) Intravenous route
Post intravenous administration, the half-life of dexmedetomidine and its terminal elimination half-life are about 6 min and 2 h, respectively. The administration of 0.2–0.7 µg/kg/h dexmedetomidine over a 24 h period leads to the linear expression of its pharmacokinetic effects.
Dexmedetomidine exerts a biphasic effect on blood pressure; as its concentration decreases, vasodilatation increases, due to its central effect. Doses of 0.25–1 µg/kg in adults and 0.5–6 µg/kg/h in children decrease blood pressure by 13–16% and 20%, respectively. Therefore, dexmedetomidine should be administered slowly as it results in unwanted blood pressure changes [524].
(3) Intranasal route
Intranasal route is popular in pediatric sedation owing to its numerous advantages. It is void of the injections like in the intravenous and intramuscular routes, and the bitter taste associated with oral administration. Intranasal administration is easy, safe, effective, and non-invasive. In children the acquiescence to sedation via intranasal administration is higher than that of oral administration [20].
Intranasal drug delivery is also favorable in children when time is limited [25]. At most, 0.15–0.2 ml should be administered in each nostril, as volumes greater than this will be partly absorbed orally [25]. Dexmedetomidine is best absorbed after sublingual and intranasal administration, with a bioavailability of about 82% post intranasal administration.
However, midazolam has been the preferred intranasally administered premedication in children due to its ease of administration and efficiency [26]. Notwithstanding, its use is restricted by the resulting irritation and burning feeling in the nasal mucosa [20]. Yuen et al. [6] conducted a clinical trial to assess the efficacy of intranasal dexmedetomidine and oral midazolam in pediatric premedication. They reported that premedication by intranasal administration of 1 µg/kg dexmedetomidine produced moderate sedation compared to oral administration of midazolam [6]. Reportedly, the time of onset of the sedative effect after the administration of 1–1.0 µg/kg dexmedetomidine intranasally is about 45 min, with a peak onset at 1.5–2.5 h [427].
A randomized double-blind controlled trial on 2–12-year-old children showed that intranasal administration of 0.5–l µg/kg dexmedetomidine produces a stronger sedative effect than oral administration of 0.5 µg/kg midazolam [27]. Additionally, intranasal dexmedetomidine administration in children results is inadequate hemodynamic effects; however, these actions are clinically irrelevant and no interference is needed [6]. Maximum reduction of systolic blood pressure (14.1%) and heart rate (16.4%) were observed after the intranasal administration of 0.5 and l µg/kg dexmedetomidine, respectively.
The nasal mucosa has an abundant blood supply, leading to quick drug absorption and onset of action. Additionally, the proximity and access to the CSF via the subarachnoid space, and the olfactory nerve and its sheath leads to speedy attainment of desired CNS levels and quicker onset of action [6]. All these make intranasal dexmedetomidine administration more tolerable and favorable in children than oral administration.
(4) Intramuscular route
The intramuscular administration of up to 2.5 µg/kg dexmedetomidine as premedication has previously been reported [13]. Also, it was suggested that the intramuscular route permits a rapid onset of action and offers better predictability because its plasma concentration peaks within 15 min of administration [5].
7) Clinical uses
(1) Premedication
In children, an ideal premedication must: 1) be available in an acceptable form; 2) have a rapid onset of action; 3) provide mild sedation along with the desired anxiolytic effect; 4) exert its effects for a desired time; 5) have no adverse effects; and 6) facilitate post-operative recovery. Midazolam, commonly used as premedication in children, has been reported to significantly ameliorate preoperative anxiety and nervousness [6].
Some studies have recommended the use of dexmedetomidine as a premedication for children, to decrease anxiety and the occurrence of delirium [21]. It is recommended that 0.33–0.67 mg/kg (i.v) or 2.5 µg/kg (i.m) should be administered 15 min before operations [13]. A meta-analysis of dexmedetomidine as a premedication reported that, compared to midazolam, it results in greater preoperative sedation and decreased postoperative pain [28]. Another meta-analysis reported the observation of a similar effect on postoperative pain, significant reduction in the doses of rescue analgesic drugs, decreased anxiety with parental separation and decreased postoperative agitation with dexmedetomidine compare with midazolam [4].
(3) Analgesia
The analgesic effect of dexmedetomidine results from its stimulation of central nervous system α2-adrenergic receptors. A recent systematic review of various randomized control trails on α2-adrenergic receptor agonists stated that the post-operative clinical use of dexmedetomidine was sparsely similar to that of morphine as they both decrease the intensity of pain in the 24 h postoperative period [29].
(4) Anxiolysis
The anxiolytic effect of dexmedetomidine in premedication has been proven comparable to that of benzodiazepines. Overall, dexmedetomidine decreases the requirement of additional sedatives and post-operative delirium [3].
8) Adverse effects of dexmedetomidine
Jannu et al. [21] after orally administering midazolam and dexmedetomidine as premedication to children reported their two most common adverse effects to be decreased blood pressure and bradycardia. Dexmedetomidine can decrease sympathetic outflow by decreasing plasma epinephrine and norepinephrine levels, leading to hypotension and decreased heart rate [30]. Similarly, upon comparison of the hemodynamic parameters (before and during surgery) of midazolam, clonidine, and dexmedetomidine administered as premedication to children, it was found that both clonidine and dexmedetomidine resulted in decreased heart rate and blood pressure [13]. However, Mountain et al. [21] suggested that oral administration of up to 4 µg/kg dexmedetomidine results in no adverse events other than hypotension and bradycardia.
9) α2-adrenoceptors antagonists of dexmedetomidine
α2-adrenoceptors antagonists are a group of drugs capable of crossing the blood-brain barrier and reversing the action of α2-adrenoceptors [5]. The main selective α2-adrenoceptor antagonists are atipamezole, idazoxan, and yohimbine [5]. Previous studies have demonstrated successful reversal of the sedative and hypotensive effects of dexmedetomidine by intravenously administered atipamezole [313233].
Dexmedetomidine is a safe and widely used clinical sedative. Its therapeutic effects include sedation, analgesia, and anxiolysis, and primarily result from its high-affinity binding to α2-adrenoceptors. Its properties therefore make it an efficacious and safe sedative for pediatric dental procedures.


 XML Download
XML Download