

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Maxillofacial injuries from trauma cause large deficits in bone, specifically in the mandible which require surgical restoration. Automobile accidents in the civilian population, gunshot wounds in armed conflict, and various battlefield injuries cause significant trauma to the maxillofacial skeleton and recent studies have shown that the mandible is most affected12. The treatment required to return structure and function to these injuries is often achieved at great cost. In order to reduce the restorative burden, many regenerative therapies are currently in development to promote bone regeneration and engraftment. Synthetic bone graft substitutes comprise a rapidly expanding field that aims to address the drawbacks of autologous bone grafting to repair bony non-unions.
Non-unions are translationally assessed by their ability to regenerate critical-sized bone defects in animal models; that are otherwise not expected to heal significantly over the life of the animal. A critical size defect (CSD) in bone is defined as a defect of a size that heals predominantly with fibrous tissue, not bone, during the life span of the animal3. The calvarial CSD model in rats45 and rabbits67 is commonly used to gauge therapy safety before evaluating the efficacy of therapy in larger animal models (canine8 or porcine910). However, the limitations associated with cost and use of companion animals in the large animal studies and the insufficiency of cranial models to account for mandible specific requirements limits the effective assessment of novel therapeutics. It is important to develop an appropriate animal model that can regenerate bone in the maxillofacial skeleton to account for the unique challenges presented by the anatomy of the mandible. The difficulties of regenerating bone in mandibular defects include soft tissue in growth11, insufficient blood supply12, and the forces of flexation and mastication13. There is thus a clear need for well-characterized small animal mandible specific bone regeneration models to effectively assess regenerative therapeutics14.
While mandible segmental continuity defect models have been evaluated in rabbits, mechanical instability of the mandibular complex after defect creation requires additional fixturing for stabilization. This fixturing, including miniplates15 and bicortical screws16, leads to a complex biomechanical model, which detracts from the simple screening models that would allow for quick transition into large animal models. Additionally, these models have often involved defect creation in the anterior third of the mandible in locations that have less physiological relevance in humans16.
Partial thickness bone defect models of the rabbit mandible are biomechanically stable but are not stringent enough and lack direct physiological relevance. In these models, the regeneration of bone is induced in areas that are typically populated with bone marrow17. The defect site is completely protected from microstrains due to the retention of the lingual cortex, potentially affecting the regenerative process. Partial thickness defects have also resulted in significant bone regeneration compared to full thickness defects18. In terms of evaluating therapies for implant fixation and treatment of edentulous patients, the alveolar full thickness model is potentially the most physiologically relevant19; however, current models may not be relevant in evaluating tooth-extraction type or periodontal cell driven regeneration scenarios18. More recent models involve the use of trephines to create full thickness2021 or partial thickness22 windows in the mandible that are then used to evaluate bone regeneration materials. While these sometimes lead to alveolar ridge collapse and continue to need metallic plate fixators for stabilization and to avoid iatrogenic fractures23, they are also similar to calvarial models in that they heal by the radial in-growth of bone. This is not typical of bone defects in the mandible of traumatic injuries or cancer resections which are usually 3 wall defects.
Thus the mandibular notch defect model in rabbits offers a potential model for simple yet effective therapy safety evaluation for bone regeneration if a CSD is appropriately set up and characterized. However, multiple sizes of defects have been created in this model ranging (from 90 to 450 mm3)242526. Additionally, these models are sometimes created bilaterally and sometimes need additional stabilization with stainless steel wires to either keep the scaffold therapy in place or to ensure mechanical integrity2728. In many cases, significant instances of spontaneous bone regeneration have been observed2526, or an untreated empty defect was not a part of the study design282930, raising questions regarding whether this model can serve as an appropriate CSD. The lack of standardization in the rabbit mandible notch model detracts from the extrapolation of results observed in previous studies for clinical translation or comparison to results in similar studies in the field for alternate therapeutics. To address these concerns, the objective of the current study was to identify the bone defect size in the inferior mandibular body which maintains biomechanical competence and to then establish whether a 3 wall notch defect functions as a CSD when the bone edges are cauterized.
Go to : 
II. Materials and Methods
1. Experimental design
Mandibles from skeletally mature New Zealand White rabbits in an unconnected study were harvested for mechanical testing. Notch type defects of various dimensions were made in the body of the mandible and the flexural properties of the hemi-mandibles were tested in a 3-point bending mode. The defect size which did not significantly compromise mechanical strength and modulus of the hemi-mandible was chosen for further in vivo evaluation. Bone regeneration in untreated mandibular notch defects either with or without cautery of the bone margins was evaluated for a period of 6 or 12 weeks using micro-computed tomography (micro-CT) and histomorphometry to determine if the model was a CSD.
2. Mechanical testing
Mandibles from 23 New Zealand White rabbits were harvested, cleaned of connective tissues and split along the symphysis to create two hemi-mandibles. Three sizes of bony defects were generated in the mandibular body: 12 mm×5 mm, 12 mm×8 mm, and 15 mm×10 mm to match defect sizes previously reported to be CSDs24253132. The contralateral hemi-mandibles with no defects were used as controls for flexural testing. All hemi-mandibles were tested to failure in a 3-point flexure mode at a constant strain rate of 1 mm/min while supported across a 30 mm span on a universal testing machine (Lloyd LRX; Lloyd Instruments, West Sussex, UK). The lingual side of the mandible was facing down and a 5-mm thick foam rubber was placed between each sample and the loading supports to evenly distribute the load using methods previously reported for rabbit mandible flexural testing3334. The flexural modulus and strength were calculated from the test data collected (n=8 samples/group, n=7 samples for the 15 mm×10 mm defect size).
3. Animal model
The 12 mm×5 mm defect size was chosen for the in vivo study of bone regenerative potential in the rabbit mandible. Twenty-six female New Zealand White rabbits, at least 5 months of age and ranging in weight between 4–5 kg underwent unilateral surgery to evaluate bone regenerative potential. These animals were divided into 3 groups: 6 animals underwent defect creation with no cautery of the defect edges and were evaluated at 6 weeks; 10 animals underwent defect creation with cautery of the bone defect margin and were evaluated after 6 and 12 weeks respectively. The animals were given a pre-anesthetization analgesic (0.025–0.05 mg/kg buprenorphine hydrochloride subcutaneously) and anesthetized using Telazol (12.5 mg/kg intramuscularly) for induction and isoflurane (1.5%–4%) in oxygen for maintenance of general anesthesia. An incision was created along the inferior border of the rabbit mandible and the periosteum was elevated. Using a bone saw, cooled with copious sterile saline, a measured osseous defect was created along the inferior border of the mandible, immediately anterior to the antegonial notch, measuring 5 mm in depth×12 mm in length×full thickness, resulting in a 3-wall defect.(Fig. 1) To guide the surgical defect formation and histological analysis, gutta-percha was placed into small holes created in the cortical bone 10 mm from the inferior border of the mandible at 3 points (0, 6, and 12 mm). This defect was positioned anatomically anterior to the masseter muscle, posterior to the digastric muscle insertion (on the medial mandible surface) and inferior to the mental foramen. In the model with cautery, the superior bone margin of the defect was cauterized (Loop tip surgical cautery; Ahco Dealers, Nashville, TN, USA). The soft tissues were then approximated and closed in layers with resorbable 3-0 Vicryl sutures. At the conclusion of the surgery, a 25 µg/hr transdermal fentanyl patch was affixed to the dorsum in the interscapular region and maintained in place for 3 days for continued analgesia. After 6 weeks in the non-cautery group or 6 and 12 weeks in the groups with cautery, animals were euthanized via intravenously administered Fatal-Plus (1 mL/4.5 kg; Vortech Pharmaceuticals, Dearborn, MI, USA) and both hemi-mandibles were harvested and stored in neutral buffered formalin for further evaluation and analysis.
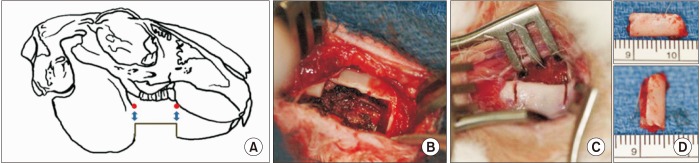 | Fig. 1Bone defect creation in the mandibular body. A, B. The 12 mm×5 mm defect was created in the region just anterior to the antegonial notch and gutta-percha markers were included 5 mm above the initial defect corners as radiographic markers. C, D. The bone defect is created by making two vertical cuts 12 mm apart and 5 mm deep using an oscillating saw to remove the inferior cortex and marrow of the mandibular body.
|
4. Radiography and micro-CT evaluation
Radiographs were acquired using a Faxitron MX20 X-ray Digital System (Faxitron X-ray, Wheeling, IL, USA) for each mandible after extraction. The images were captured at 25 kV in a 15 seconds exposure time and imported into Faxitron DR software (ver. 3.2.2; Faxitron Bioptics LLC, Tuscon, AZ, USA). Micro-CT analysis was performed using a Skyscan 1072 scanner (Bruker, Kontich, Belgium) at a resolution of 17.0 µm pixel on samples hydrated with formalin. The images were reconstructed using NRecon software (Bruker-MicroCT) to generate grayscale images ranging from 0 to 255. DataViewer was used to re-align the hemi-mandible images so that the primary axes were the principal physiological axes of the mandible. Global thresholding was performed on the samples across all the groups in the study using the Otsu algorithm to identify mineralized tissue. The defect created was then located to define the region of interest 12 mm in length along the full thickness of the mandible and the border of this region of interest was determined using the borders of the contralateral hemi-mandible. The three-dimensional (3D) mineralized volume, bone mineral density, and mineralized area distribution analysis along the 12 mm defect length were carried out on CT images using CT analyzer. These analyses were carried out for all the experimental groups in the study as well as their respective contralateral hemi-mandibles.
5. Histological evaluation
The excised mandibles were prepared for histology as previously described. Briefly, samples were dehydrated in ascending grades of ethanol, followed by xylene at 4℃ and then embedded in poly(methyl methacrylate). The specimens were then cut and ground to 30 µm thick sections using a diamond saw and MicroGrinder (Exakt Technologies, Oklahoma City, OK, USA). This was performed for 4 samples in the 6-week group without cautery, 6 samples in the 6-week group with cautery, and 7 samples in the 12-week group with cautery. The sections were mounted on slides and stained with Sanderson's Rapid Bone Stain and counterstained with van Gieson's picrofuchsin to stain soft tissue blue and bone pink/red. Cellular tissue debris was stained black.
Histology slide images of 2.0× magnification were acquired on an Olympus SZX16 Research High-Class Stereo Microscope (Olympus, Center Valley, PA, USA) with an Olympus DP71 Microscope Digital Camera and compiled using Photoshop (v7.0.1; Adobe Systems, San Jose, CA, USA). High magnification images (40× and 100×) were acquired on a Nikon Eclipse 55i Research Microscope with a DS-f11 Digital Camera (Nikon Instruments, Melville, NY, USA). The entire defect area was selected by manually tracing the outer boundary and the number of pixels was quantified. Mineralized tissue was selected within the defined defect area by a color threshold of the pink/red stain and the number of bone pixels was measured. The percentage of the mineralized tissue was calculated as the ratio of the mineralized tissue to the defect area. The presence of mineralization in the bone canals and the presence of cellular/tissue debris at the defect edges was scored and reported as a percentage of the number of samples in the group.
6. Statistical analysis
All data are represented as the mean±standard error of the mean. Significance in flexural mechanical testing and micro-CT bone volume measures reported was determined using a paired t-test between the experimental and contralateral groups. Significance in the bone area fill from the histomorphometric analysis was determined using one-way ANOVA with Tukey's test for post hoc analysis. A significant level of differences between observed proportions of cellular debris and canal mineralization was determined using the z-test and applying the Yates correction for sample size. The level of significance was set at P<0.05 for all statistical measures reported. All statistical analysis was performed on Sigmaplot software (ver. 14.0; Systat Software, San Jose, CA, USA).
Go to :
III. Results
1. Mechanical testing
In terms of flexural stress to failure, the 12 mm×5 mm defects (163±9 MPa) were not significantly different from their contralaterals (191±10 MPa); while the 12 mm×8 mm (169±10 MPa vs 253±32 MPa) and 15 mm×10 mm (122±9 MPa vs 215±15 MPa) groups carried significantly less load than their respective contralateral controls (P<0.05). The flexural stiffness of the hemi-mandibles had similar trends. (Table 1) No differences were observed between the control and the 12 mm×5 mm defect size while both groups of hemimandibles with 12 mm×8 mm and 15 mm×10 mm defects had significantly poorer flexural properties than their intact contralateral hemi-mandibles (P<0.05). This study demonstrated that the 12 mm×5 mm defect did not significantly compromise the mechanical integrity of the mandible and this size of defect was chosen to further evaluate whether spontaneous regeneration of bone occurred in the mandible when defects of this size were created.

Table 1
Mechanical flexural properties of hemi-mandibles with different sized defects
| Size | Strength (MPa) | Stiffness (MPa) | ||
|---|---|---|---|---|
| Defect side | Contralateral | Defect side | Contralateral | |
| 12 mm×5 mm | 163±9 | 191±10 | 41±3 | 55±7 |
| 12 mm×8 mm | 169±10* | 253±32 | 44±5* | 58±7 |
| 15 mm×10 mm | 122±9* | 215±15 | 24±3* | 50±3 |
Flexural strength and flexural stiffness of hemi-mandibles with defects of different sizes at the inferior margin of the mandibular body compared to matched contralateral controls.
Asterisk indicates defect side has significantly reduced biomechanical properties compared to the contralateral, *P<0.05.
![]()
2. Radiography and micro-CT evaluation
Radiographic analysis revealed that opaque bridging of the defect site was present in the defect without cautery at 6 weeks, although the quality of the opacity was less than that in the cortex of the contralateral hemi-mandibles. Very limited opacity was observed in the defect site of the groups with cautery after 6 weeks, however, the opacity increased at the 12-week time point.(Fig. 2) Representative micro-CT cross sections of the groups indicating the defect site are also presented.(Fig. 2) The micro-CT data was used to quantify the bone volume in 3D. Without cautery at 6 weeks, no difference in bone volume within the defect was detected between the surgical mandible and its contralateral control.(Fig. 3) In terms of regenerated bone volume, significantly less bone was regenerated at 6 weeks with cautery (70.5±9 mm3) of the defect margins when compared to the group without cautery (93.6±6 mm3) at 6 weeks. After 12 weeks, the group with cautery showed increased bone volume (93.1±5 mm3) equivalent to the 6 weeks group without cautery.(Fig. 3) For comparison, the contralateral hemi-mandibles had an average of 120.4±7 mm3 of bone and the total volume of the defect was 264.5±13 mm3. In terms of regenerated bone volume, the micro-CT analysis showed significantly less bone was regenerated at 6 weeks in the hemi-mandibles with cautery compared with their respective contralaterals (P<0.05).(Fig. 3)
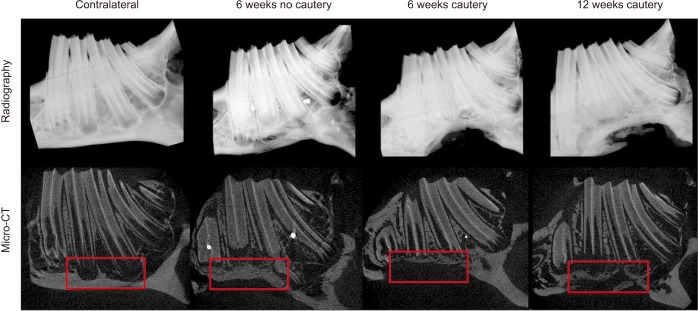 | Fig. 2Radiographic and micro-computed tomography (micro-CT) assessment of hemi-mandibles. Radiographs of the contralateral hemimandibles showing intact architecture and representative images from the three experimental groups showing regenerated bone after 6 or 12 weeks post defect creation. Micro-CT longitudinal sectional images of representative animals from each of the experimental groups showing bone regeneration within defect sites (boxed) compared to non-surgical control sites shown in the contralateral hemi-mandible (boxed).
|
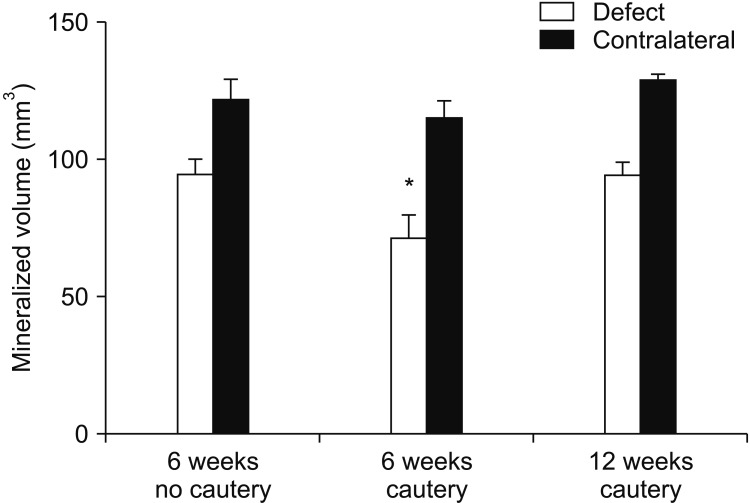 | Fig. 3Bone volume at defect site in micro-computed tomography (micro-CT) analysis. The bone volumes in the defect groups without cautery at 6 weeks and with cautery at 12 weeks were not significantly different from their contralateral controls, but the bone volume in the defect group with cautery was significantly lower compared to the contralateral hemi-mandible after 6 weeks (*P<0.05).
|
The regenerated bone mineral density within the defect space was 91.1%±1% of the contralateral hemi-mandibles for the group without cautery after 6 weeks, and 88.3%±2% of the contralateral hemi-mandibles for the group with cautery after 6 weeks, and 86.8%±1% after 12 weeks, with no significant difference between groups. None of the experimental hemi-mandibles were found to be significantly different in terms of BMD from the contralateral hemi-mandibles either. The evaluation of the bone at every cross-section along the defect length indicated that not only did the group without cautery at 6 weeks and the group with cautery at 12 weeks regenerate a greater bone area than the group with cautery at 6 weeks, they did so at every location along the anterior-posterior axis of the defect.(Fig. 4) Additionally, it was clearly observed from the bone regeneration patterns at the defect site that bone in-growth occurred from each of the three walls of the defect.
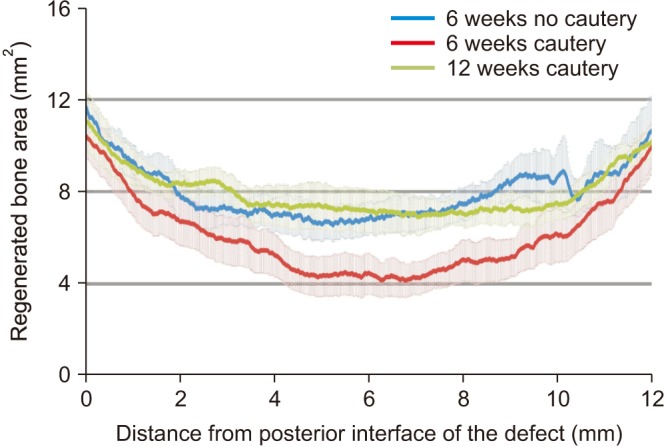 | Fig. 4Bone regeneration patterns within the defect in micro-computed tomography (micro-CT) analysis. The bone volume regenerated within each group was evaluated at every 17 µm along the defect from the posterior to the anterior margin. This evaluation showed that while there was no difference in regeneration patterns between the defect with no cautery at 6 weeks (in blue) and the defects with cautery after 12 weeks (in green), significantly less bone was regenerated at every location in the defects with cautery after 6 weeks (in red) compared to the other two groups.
|
3. Histological evaluation
Gross histological examination of the experimental groups indicated similar trends to those indicated in micro-CT analysis. Bridge-like bone-fronts spanned the defect site margins in the 6-week group without cautery and the 12-week group with cautery, whereas limited bone growth was seen within the defect in the 6-week group with cautery. The histological sections also revealed localized inflammatory tissue debris present at the interface of the apex of teeth and the superior defect border in groups when cauterization was used, at both 6 and 12 weeks.(Fig. 5) No such cellular debris was seen in the non-cautery group. Also noted in the histology was the presence of bone growth into the root canals of the cut teeth.(Fig. 5) The proportion of animals within each group in which either cellular debris or canal mineralization was observed are listed in Table 2. While there was no statistical significance in the prevalence of inflammation or bone in the root canals, there was a strong trend (P=0.054 in the 6-week no cautery vs 6-week cautery) that cauterization resulted in the presence of increased cell debris and impacted the quality of healing. The histomorphometry data showed similar trends to that of the micro-CT, but no significant differences between surgical groups were found.(Fig. 6)
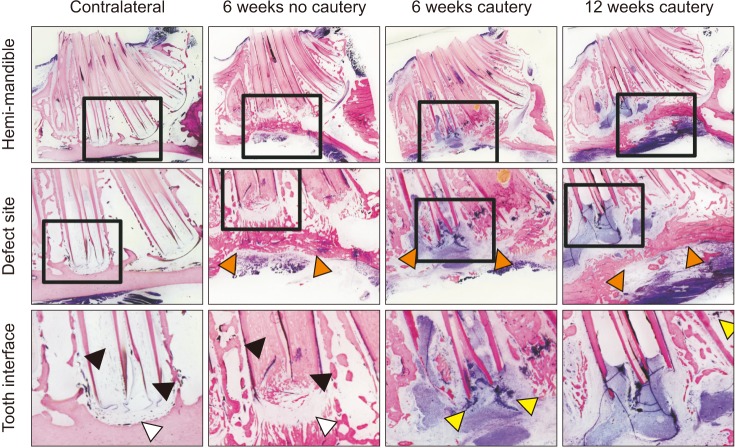 | Fig. 5Histological evaluation showing bone regeneration, intercanal ossification, and cellular debris. Histological sections were prepared along the longitudinal axis of the hemi-mandibles and stained with Sanderson's Rapid Bone stain and counterstained with van Geison's stain to label mineralized tissue pink and soft tissue blue (×2). While a ridge of bone regenerated the cortex in the defects without cautery at 6 weeks and in the defects with cautery at 12 weeks, no such regeneration was seen in the defects with cautery after 6 weeks (orange arrows). At the defect margins, cellular debris was observed in the groups with cautery of the margins (yellow arrows). While the hemimandibles had clear tooth canals, the tooth canals in the defects without cautery had ossification after 6 weeks (black arrows), possibly due to a robust regenerative response from the periodontal tissues (white arrows).
|
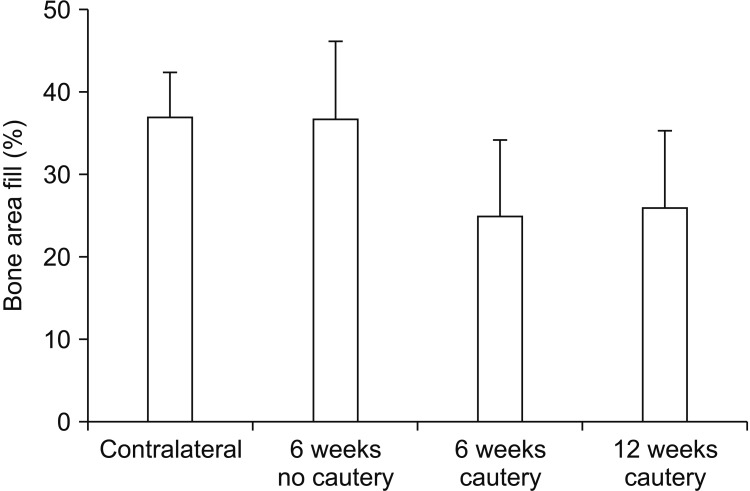 | Fig. 6Histomorphometric analysis of bone area regenerated at the defect site. While no significant differences were observed between the different groups in terms of the area of bone regeneration, a strong trend (P=0.16) of lower mineralized area was observed in the groups with cautery compared to the group without cautery or the contralateral hemi-mandible.
|

Go to :
IV. Discussion
This study investigated defects, previously claimed to be CSDs, in the rabbit mandible in terms of their effect on the biomechanical properties of the mandible. Defects that were 12 mm×5 mm32, 12 mm×8 mm2935, and 15 mm×10 mm2430 in size were created and hemi-mandible flexural properties were evaluated. The 12 mm×5 mm size allowed the simulation of a physiologically stabilized defect without the need for additional fixation while the larger defect sizes were significantly weaker in terms of flexural strength and modulus. Mechanical stability is one of the crucial elements required for bone regeneration36 and if the mandibular bone is compromised due to the creation of the defect, fixation through stainless steel wire2735, plating1821 or usage of bicortical screws16 is essential for rigid fixation. However, rigid fixation of the mandible also leads to potential stress shielding and poor bone regeneration at the defect site. Not plating the mandible can also be seen as a benefit to bone healing as described in a recent study by Zoumalan et al.37. They speculated that stresses on the mandible are required for bone formation and that plating of the mandible may act as a stress shield to the healing bone which, in turn, results in insufficient boney healing37. The 12 mm×5 mm defect size was chosen for further evaluation in this study to reduce the need for mechanical fixation in the model and to easily evaluate novel therapeutics in a large volumetric bone defect. A similar strategy is used in the case of the rabbit radius CSD model for extremity trauma where the presence of the fused ulna provides anatomical internal fixation and stability without the need for further support38. An additional advantage of the notch defect site at the inferior margin of the mandibular body is that it avoids damage to muscles of mastication and eliminates the chance of infection from intra-oral flora. Defects with communication to the oral cavity could have potential complications due to excessive soft tissue prolapse and infection21.
In the case of notch type defect models in the rabbit model, multiple studies have evaluated defects of various sizes at different locations in the mandible with little consistency, leading to great difficulty in comparing results across these studies24252627282930313235394041. In Table 3, these studies are compared in terms of the size and location of the defect, age of the animal, type of fixation if any and methods of evaluation used. In comparison, skeletally mature rabbits weighing between 4–5 kg and greater than 21 weeks of age42 were used for unilateral defect creation in the current study. The evaluation of bone regeneration at the defect site indicated that significant bone regeneration occurred over 6 weeks in the 180 mm3 defect when the defect margins were not cauterized and over 12 weeks when the defect margins were cauterized. Thus, contrary to other reports of 180 mm3 defects being considered CSDs283032 we observed that this defect size did not meet the requisite criteria to be used as a CSD in the rabbit mandible.
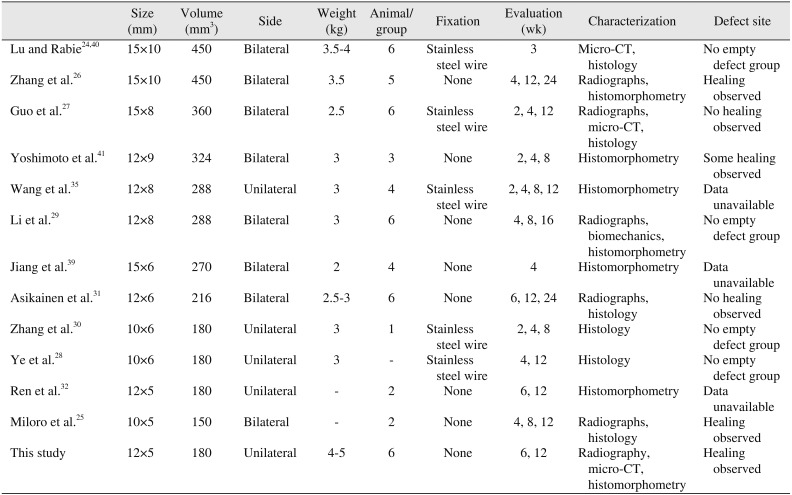
Table 3
Variations in defect size and volume in literature reports of critical-sized notch defects in the rabbit mandible
| Size (mm) | Volume (mm3) | Side | Weight (kg) | Animal/group | Fixation | Evaluation (wk) | Characterization | Defect site | |
|---|---|---|---|---|---|---|---|---|---|
| Lu and Rabie2440 | 15×10 | 450 | Bilateral | 3.5-4 | 6 | Stainless steel wire | 3 | Micro-CT, histology | No empty defect group |
| Zhang et al.26 | 15×10 | 450 | Bilateral | 3.5 | 5 | None | 4, 12, 24 | Radiographs, histomorphometry | Healing observed |
| Guo et al.27 | 15×8 | 360 | Bilateral | 2.5 | 6 | Stainless steel wire | 2, 4, 12 | Radiographs, micro-CT, histology | No healing observed |
| Yoshimoto et al.41 | 12×9 | 324 | Bilateral | 3 | 3 | None | 2, 4, 8 | Histomorphometry | Some healing observed |
| Wang et al.35 | 12×8 | 288 | Unilateral | 3 | 4 | Stainless steel wire | 2, 4, 8, 12 | Histomorphometry | Data unavailable |
| Li et al.29 | 12×8 | 288 | Bilateral | 3 | 6 | None | 4, 8, 16 | Radiographs, biomechanics, histomorphometry | No empty defect group |
| Jiang et al.39 | 15×6 | 270 | Bilateral | 2 | 4 | None | 4 | Histomorphometry | Data unavailable |
| Asikainen et al.31 | 12×6 | 216 | Bilateral | 2.5-3 | 6 | None | 6, 12, 24 | Radiographs, histology | No healing observed |
| Zhang et al.30 | 10×6 | 180 | Unilateral | 3 | 1 | Stainless steel wire | 2, 4, 8 | Histology | No empty defect group |
| Ye et al.28 | 10×6 | 180 | Unilateral | 3 | - | Stainless steel wire | 4, 12 | Histology | No empty defect group |
| Ren et al.32 | 12×5 | 180 | Unilateral | - | 2 | None | 6, 12 | Histomorphometry | Data unavailable |
| Miloro et al.25 | 10×5 | 150 | Bilateral | - | 2 | None | 4, 8, 12 | Radiographs, histology | Healing observed |
| This study | 12×5 | 180 | Unilateral | 4-5 | 6 | None | 6, 12 | Radiography, micro-CT, histomorphometry | Healing observed |
![]()
Previous studies also state that the location within the mandible is of critical importance in determining the extent of bone regeneration at the defect site. Guo et al.27 demonstrated that the presence of greater marrow adjacent to the defect leads to a more robust regenerative response possibly because of a greater number of stem cells. Similarly, in our study, we observed a robust regenerative response from the base of the teeth roots, where the defect had been created. Histological evidence of periodontal like tissue was also observed in the group without cautery of the defect margin. Although not directly investigated in this study, it is possible that the periodontal ligament and mandibular bone marrow stem cells could have played a role in the robust regenerative response at the defect site. The bone regenerative capacity of periodontal ligament and bone marrow stem cells has been previously reported in other in vivo models4344.
Cauterization of the bone defect margins as a technique to inhibit regeneration and create non-union models has been previously employed in rat femoral defects4546. Since the 12 mm×5 mm defect created in the present study healed spontaneously over 6 weeks, cautery of the defect margins was employed in order to make the defect model more challenging. However, even after inhibition of bone growth by cauterization, the regenerated bone increased from 6 to 12 weeks reaching a level similar to the non-cauterized bone at 6 weeks. Cauterization of the defect margins did; however, result in a delay of the bone growth and demonstrably increased tissue debris at the defect margins. The presence of tissue debris and decreased regeneration at the defect site suggests that the cauterization limited the vascular infiltration from the bony margins and delayed the recruitment of stem cell populations to the defect site. It should be noted that only electrocautery was tested in this study and not the effect on the local responsive cell population if a different form of inhibition (such as chemical cauterization47) were to be employed.
Bone growing into the exposed root canals may be a further indicator of an aggressive osteogenic response from periodontal and dental stem cells due to the alteration in the local microenvironment as a result of creating a non-segmental defect without tooth extraction. Traumatic injuries to immature teeth have been reported to result in the in-growth of mineralized tissues within the dental canal and pulp chamber4849. Wang et al.50 described multiple histologic responses, including intercanal bone in immature canine teeth following the use of antibiotic paste, suggesting a possible relationship between inflammatory responses and canal mineralization.
While several groups have previously reported the performance of bone regenerative therapies in the rabbit mandible, many have chosen to not include an empty defect group282940 or have poorly described the regenerative outcomes of such a group3239. Given the spontaneous regeneration of the defect site observed in this study and reported by others for mandibular defects in rabbits19, it is recommended that future studies comprehensively characterize the chosen defect model, resort to well-characterized CSDs in the rabbit calvaria, or choose larger animal models to evaluate regenerative efficacy at mandibular sites.
Go to :
V. Conclusion
Contrary to multiple literature reports that have used the full thickness notch defect model in the rabbit mandible to evaluate regenerative therapies, this study showed that a 12 mm×5 mm defect is biomechanically stable and cannot be considered critical-sized even with cauterization. Since cauterization was found to delay healing by 6 weeks, a potential application of this model could be to evaluate bone regenerative therapeutics that accelerate bone re-growth rather than simply the success or failure of therapy.
Go to :
 XML Download
XML Download