

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
As dental implant surgery for edentulous patients became a gold standard, bone grafts such as guided bone regeneration and sinus lift were widely operated in Korean dentist. There has been increased in the number of bone substitute products available to the dental clinician. Still the autologous bone is considered to gold standard, because of its three properties with osteoconduction, osteoinduction and osteogenesis. Osteogenesis is, the property of autogenous graft, generation of new bone from osteogenic cells within the graft. Osteoinduction is the property of the autogenous graft, allogenic graft and intrinsic bone matrix proteins such as transforming growth factor and bone morphogenetic proteins (BMP) to recruit of host stem cells. Osteoconduction is the property of a mechanical structure with biocompatibility for the migration of osteogenetic cells12.
Allograft has been widely used and is an attractive alternative as it avoids donor site morbidity. It has the following advantage: (1) donor site is not needed, (2) abundant supply, and (3) little risk of transmission of infectious diseases3. The ideal alloplastic bone substitutes is biologically stable and maintain its volume with allowing cell infiltration and remodeling process4. The alloplastic bone substitutes has various osteoconductive capabilities depending on the manufacturing methods, crystal structure, size of pores, mechanical properties, composition and absorption rate5.
Hydroxyapatite (HA) is the main mineralized of bone tissue and it exerts an osteoconductive ability when grafted in the defect. Synthetic calcium phosphate ceramics (β-tricalcium phosphate [β-TCP] and HA) could be altered to autogenous graft, allogenic graft and xenogenic graft and it was used as block, cement, pastes, powder, granules and putty type with carboxymethyl cellulose or hyaluronic acid6. In Korea, the development of implant dentistry has led to the development of many dental synthetic bone substitute in many domestic companies.
As dental implant surgery for edentulous patients became a gold standard, bone grafts such as guided bone regeneration and sinus lift were widely operated in Korean dentist. All bone substitutes used commercially in Korea are firstly evaluated by the Ministry of Health and Welfare (MOHW) for safety and efficacy of the product. They are commercialized after being priced, classified, and registration by the Health Insurance Review and Assessment Service (HIRA). The post-application management is obligatory for the manufacturer (or representative importer) to receive a certificate of Good Manufacturing Practice (GMP) by Ministry of Food and Drug Safety (MFDS).
According to Korea Food and Drug Safety (KFDS) No. 2016-156 of ‘medical device manufacturing and quality control standards’, after the approval of commercially use, the manufacturer or importer is required to renew the conformity certification every three years or immediately if the information of product changed7. If any information of the product changed, the certificate of conformity should be issued or reissued by the manufacturer or the importer. Therefore, the manufacturer or importer of registered in the MFDS could be important factors in terms of quality control of currently available bone substitutes.
However, it is difficult for clinicians to know whether the certification or the quality of product is properly managed. Therefore, the purpose of this study is to analyze ingredients, manufacturers, importers, current status and reference levels of dental synthetic bone listed in MOHW notification No. 2018-248.
Go to : 
II. Materials and Methods
Commercially available dental alloplastic bone substitute which was approved MOHW notification (No. 2018-248)8 is analyzed the details of manufacturer, importer, composition, available form, Food and Drug Administration (FDA, USA) approval.
This review of literature included studies that detailed the use of bone graft substitute in dental situation, animal, in vivo, and in vitro studies. We excluded studies in the orthopedic and neurosurgery field and those not published in English or Korean. The Google Scholar, ISI Web of Knowledge, PubMed, EMBASE (1980–2019) and Cochrane Databases were searched in February 2019 using the criteria of registered or trademarked product name. The authors read the full text of the studies and classified it according to the ‘level of evidence’ presented by Wright et al.9.(Table 1)
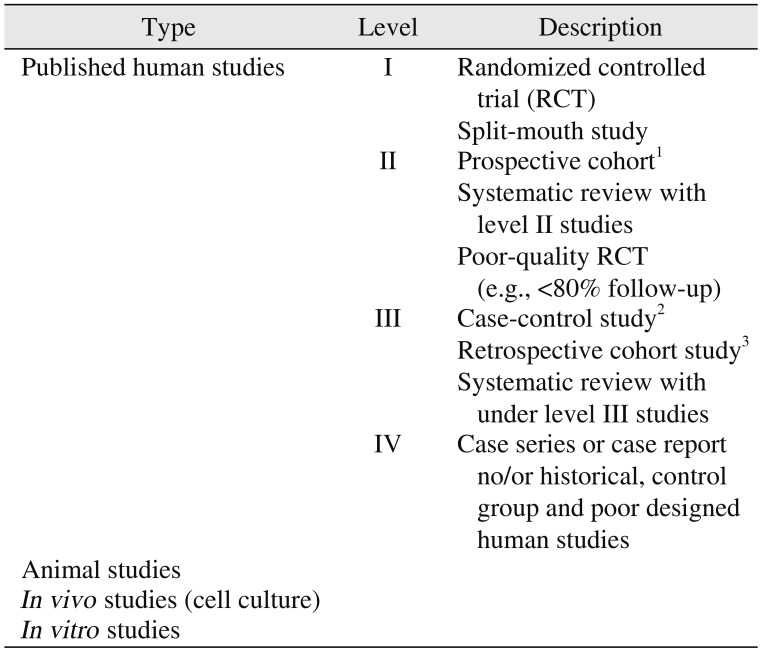
Table 1
Level of evidence for research questions9
![]()
Human study level I evidence is a prospective, randomized, or splint-mouth study with definite results that support the use of alloplastic bone substitute in clinical condition. The case report was classified as level IV. Clinicial studies used alloplastic bone substitute as carrier of osteoinductive growth factors or as comparison of membrane efficacy have not been evaluated for osteoconductive capacity, but have been assigned to human study level IV as showing clinical stability. The animal, in vivo, and in vivo study were separately indicated. All authors reviewed each paper and independently assigned evidence levels. If there is a disagreement on the assigned level, discussion and resolution were made. All studied with human study level I, II, III, or IV were included to be citation10.
Go to :
III. Results
In December 2018, thirty-seven dental alloplastic substitutes were registered in MOHW and HIRA8. However, there were two products (BIO-C [Cowellmedi, Busan, Korea] and OssPol-Dental [Genewel, Seongnam, Korea]) that were not commercially available and one product of DualPor COLLAGEN D-INJECTION (OssGen, Daegu, Korea) that was discontinued in the market. Of the remaining 34 alloplastic substitutes, 28 products (82.4%) could be obtained information and included in this review. To approve certificate of GMP from MOHW and MFDS, the company should submit the researches for safety and efficacy of its product, as same procedure as U.S. FDA.(Table 2) The researches, however, were not published and the authors could not include in this review. The available information regarding the delivery form, component, indications, morphology (porosity, biomechanical structure, particle size), and property are shown in Tables 3, 4, 5, 6, 7, 8.
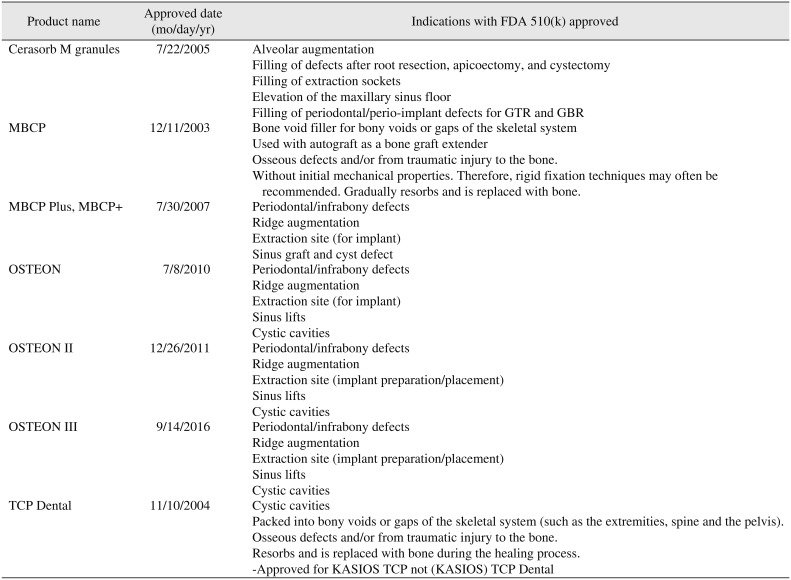
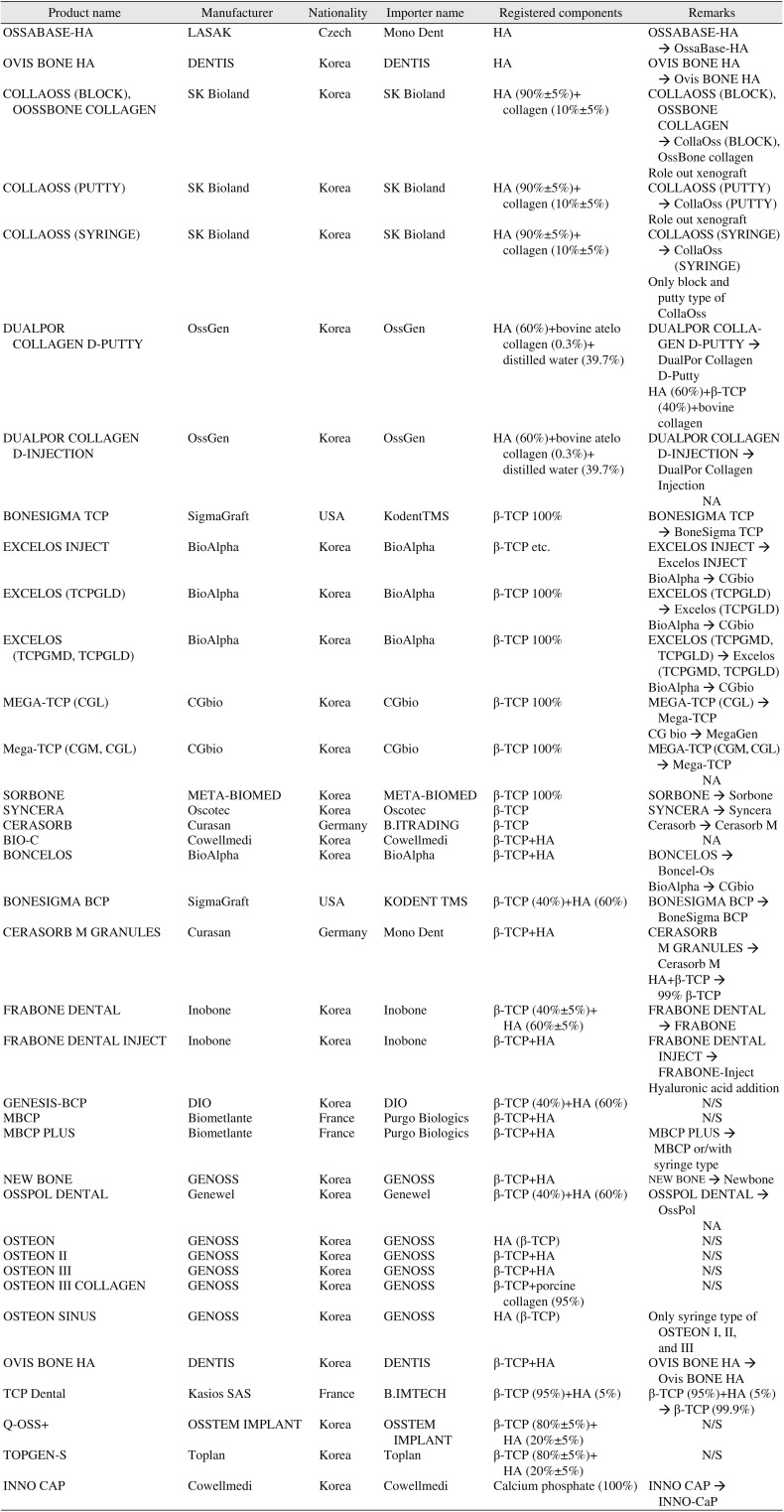
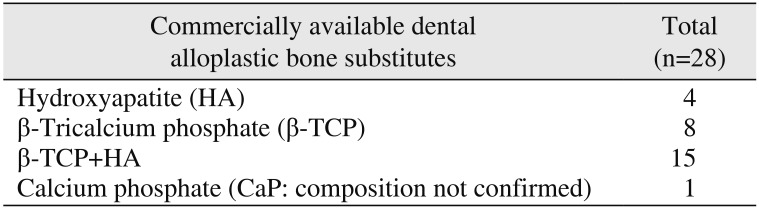
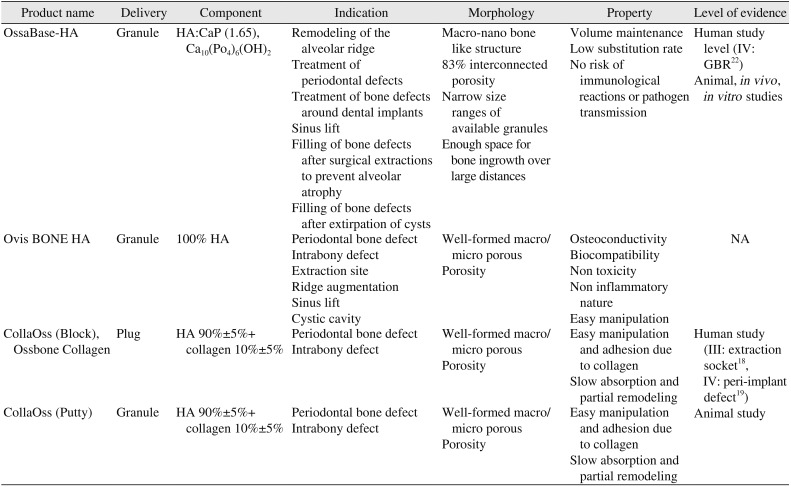
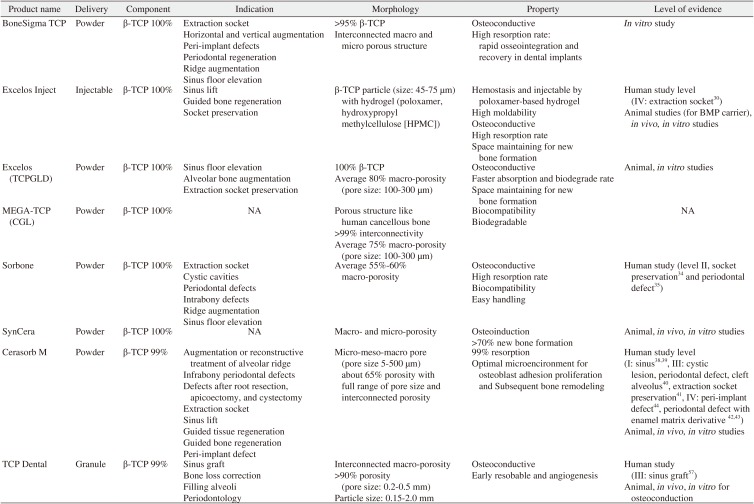
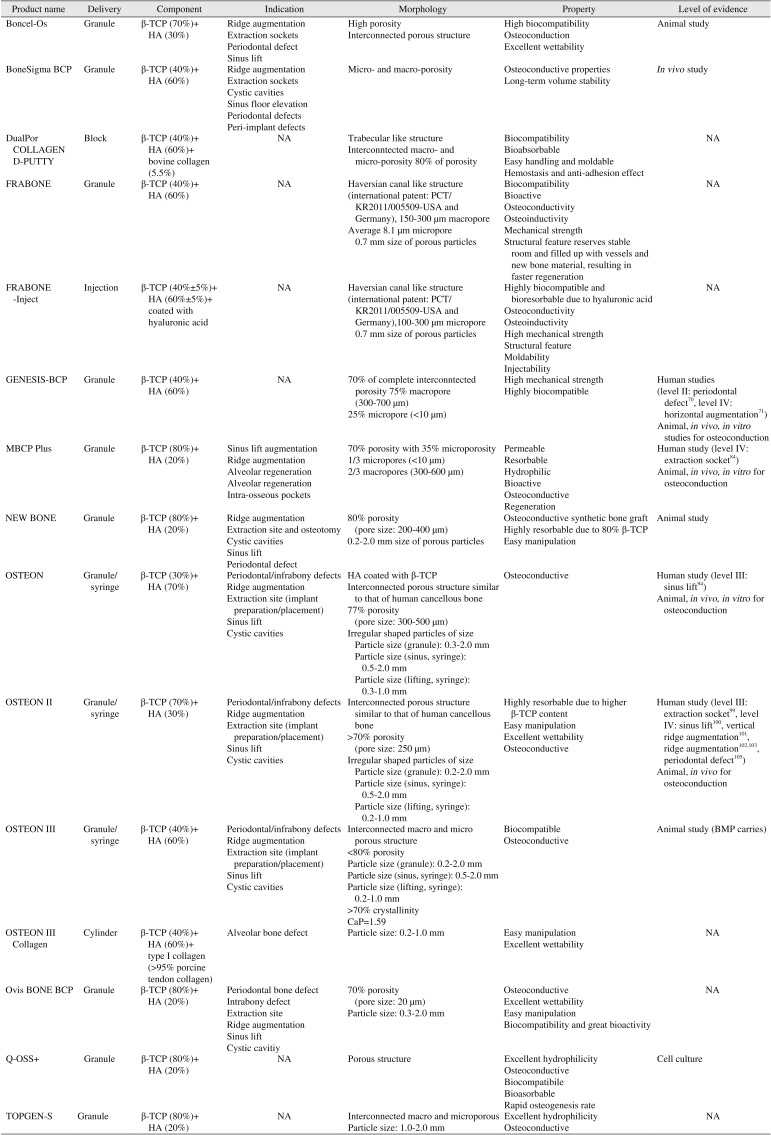

Table 2
Dental bone graft substitutes which Food and Drug Administration (FDA) 510(k) approved
![]()
Table 3
Dental bone graft substitutes with manufactures, importer, components and inconsistency with registered in Korean Ministry of Health and Welfare and Korean Health Insurance Review and Assessment Service
![]()
Table 4
Commercially available dental alloplastic bone substitutes according to components
| Commercially available dental alloplastic bone substitutes | Total (n=28) |
|---|---|
| Hydroxyapatite (HA) | 4 |
| β-Tricalcium phosphate (β-TCP) | 8 |
| β-TCP+HA | 15 |
| Calcium phosphate (CaP: composition not confirmed) | 1 |
![]()
Table 5
Dental bone graft substitutes which was consisted with hydroxyapatite (HA)
| Product name | Delivery | Component | Indication | Morphology | Property | Level of evidence |
|---|---|---|---|---|---|---|
| OssaBase-HA | Granule | HA:CaP (1.65), Ca10(Po4)6(OH)2 | Remodeling of the alveolar ridge | Macro-nano bone like structure | Volume maintenance | Human study level (IV: GBR22) |
| Treatment of periodontal defects | 83% interconnected porosity | Low substitution rate | Animal, in vivo , in vitro studies | |||
| Treatment of bone defects around dental implants | Narrow size ranges of available granules | No risk of immunological reactions or pathogen transmission | ||||
| Sinus lift | Enough space for bone ingrowth over large distances | |||||
| Filling of bone defects after surgical extractions to prevent alveolar atrophy | ||||||
| Filling of bone defects after extirpation of cysts | ||||||
| Ovis BONE HA | Granule | 100% HA | Periodontal bone defect | Well-formed macro/micro porous | Osteoconductivity | NA |
| Intrabony defect | Porosity | Biocompatibility | ||||
| Extraction site | Non toxicity | |||||
| Ridge augmentation | Non inflammatory nature | |||||
| Sinus lift | Easy manipulation | |||||
| Cystic cavity | ||||||
| CollaOss (Block), Ossbone Collagen | Plug | HA 90%±5%+ collagen 10%±5% | Periodontal bone defect | Well-formed macro/micro porous | Easy manipulation and adhesion due to collagen | Human study (III: extraction socket18, IV: peri-implant defect19) |
| Intrabony defect | Porosity | Slow absorption and partial remodeling | ||||
| CollaOss (Putty) | Granule | HA 90%±5%+collagen 10%±5% | Periodontal bone defect | Well-formed macro/micro porous | Easy manipulation and adhesion due to collagen | Animal study |
| Intrabony defect | Porosity | Slow absorption and partial remodeling |
![]()
Table 6
Dental bone graft substitutes which was consisted with β-tricalcium phosphate (β-TCP)
| Product name | Delivery | Component | Indication | Morphology | Property | Level of evidence |
|---|---|---|---|---|---|---|
| BoneSigma TCP | Powder | β-TCP 100% | Extraction socket | >95% β-TCP | Osteoconductive | In vitro study |
| Horizontal and vertical augmentation | Interconnected macro and micro porous structure | High resorption rate: rapid osseointegration and recovery in dental implants | ||||
| Peri-implant defects | ||||||
| Periodontal regeneration | ||||||
| Ridge augmentation | ||||||
| Sinus floor elevation | ||||||
| Excelos Inject | Injectable | β-TCP 100% | Sinus lift | β-TCP particle (size: 45-75 μm) with hydrogel (poloxamer, hydroxypropyl methylcellulose [HPMC]) | Hemostasis and injectable by poloxamer-based hydrogel | Human study level (IV: extraction socket30) |
| Guided bone regeneration | High moldability | Animal studies (for BMP carrier), in vivo, in vitro studies | ||||
| Socket preservation | Osteoconductive | |||||
| High resorption rate | ||||||
| Space maintaining for new bone formation | ||||||
| Excelos (TCPGLD) | Powder | β-TCP 100% | Sinus floor elevation | 100% β-TCP | Osteoconductive | Animal, in vitro studies |
| Alveolar bone augmentation | Average 80% macro-porosity (pore size: 100-300 μm) | Faster absorption and biodegrade rate | ||||
| Extraction socket preservation | Space maintaining for new bone formation | |||||
| MEGA-TCP (CGL) | Powder | β-TCP 100% | NA | Porous structure like human cancellous bone | Biocompatibility | NA |
| >99% interconnectivity | Biodegradable | |||||
| Average 75% macro-porosity (pore size: 100-300 μm) | ||||||
| Sorbone | Powder | β-TCP 100% | Extraction socket | Average 55%-60% macro-porosity | Osteoconductive | Human study (level II, socket preservation34 and periodontal defect35) |
| Cystic cavities | High resorption rate | |||||
| Periodontal defects | Biocompatibility | |||||
| Intrabony defects | Easy handling | |||||
| Ridge augmentation | ||||||
| Sinus floor elevation | ||||||
| SynCera | Powder | β-TCP 100% | NA | Macro- and micro-porosity | Osteoinduction | Animal, in vivo, in vitro studies |
| >70% new bone formation | ||||||
| Cerasorb M | Powder | β-TCP 99% | Augmentation or reconstructive treatment of alveolar ridge | Micro-meso-macro pore (pore size 5-500 μm) about 65% porosity with full range of pore size and interconnected porosity | 99% resorption | Human study level (I: sinus3839, III: cystic lesion, periodontal defect, cleft alveolus40, extraction socket preservation41, IV: peri-implant defect44, periodontal defect with enamel matrix derivative 4243) |
| Infrabony periodontal defects | Optimal microencironment for osteoblast adhesion proliferation and Subsequent bone remodeling | Animal, in vivo, in vitro studies | ||||
| Defects after root resection, apicoectomy, and cystectomy | ||||||
| Extraction socket | ||||||
| Sinus lift | ||||||
| Guided tissue regeneration | ||||||
| Guided bone regeneration | ||||||
| Peri-implant defect | ||||||
| TCP Dental | Granule | β-TCP 99% | Sinus graft | Interconnected macro-porosity | Osteoconductive | Human study (III: sinus graft57) |
| Bone loss correction | >90% porosity (pore size: 0.2-0.5 mm) | Early resobable and angiogenesis | Animal, in vivo , in vitro for osteoconduction | |||
| Filling alveoli | Particle size: 0.15-2.0 mm | |||||
| Periodontology |
![]()
Table 7
Dental bone graft substitutes which was composed with hydroxyapatite (HA) and β-tricalcium phosphate (β-TCP)
| Product name | Delivery | Component | Indication | Morphology | Property | Level of evidence |
|---|---|---|---|---|---|---|
| Boncel-Os | Granule | β-TCP (70%)+HA (30%) | Ridge augmentation | High porosity | High biocompatibility | Animal study |
| Extraction sockets | Interconnected porous structure | Osteoconduction | ||||
| Periodontal defect | Excellent wettability | |||||
| Sinus lift | ||||||
| BoneSigma BCP | Granule | β-TCP (40%)+HA (60%) | Ridge augmentation | Micro- and macro-porosity | Osteoconductive properties | In vivo study |
| Extraction sockets | Long-term volume stability | |||||
| Cystic cavities | ||||||
| Sinus floor elevation | ||||||
| Periodontal defects | ||||||
| Peri-implant defects | ||||||
| DualPor COLLAGEN D-PUTTY | Block | β-TCP (40%)+HA (60%)+bovine collagen (5.5%) | NA | Trabecular like structure | Biocompatibility | NA |
| Interconntected macro- and micro-porosity 80% of porosity | Bioabsorbable | |||||
| Easy handling and moldable | ||||||
| Hemostasis and anti-adhesion effect | ||||||
| FRABONE | Granule | β-TCP (40%)+HA (60%) | NA | Haversian canal like structure (international patent: PCT/KR2011/005509-USA and Germany), 150-300 μm macropore | Biocompatibility | |
| Average 8.1 μm micropore0.7 mm size of porous particles | Bioactive | |||||
| Osteoconductivity | ||||||
| Osteoinductivity | ||||||
| Mechanical strength | ||||||
| Structural feature reserves stable room and filled up with vessels and new bone material, resulting in faster regeneration | ||||||
| FRABONE-Inject | Injection | β-TCP (40%±5%)+HA (60%±5%)+coated with hyaluronic acid | NA | Haversian canal like structure (international patent: PCT/ KR2011/005509-USA and Germany),100-300 μm micropore 0.7 mm size of porous particles | Highly biocompatible and bioresorbable due to hyaluronic acid | NA |
| Osteoconductivity | ||||||
| Osteoinductivity | ||||||
| High mechanical strength | ||||||
| Structural feature | ||||||
| Moldability | ||||||
| Injectability | ||||||
| GENESIS-BCP | Granule | β-TCP (40%)+HA (60%) | NA | 70% of complete interconntected porosity 75% macropore (300-700 μm) | High mechanical strength | Human studies (level II: periodontal defect70, level IV: horizontal augmentation71) |
| 25% micropore (<10 μm) | Highly biocompatible | Animal, in vivo, in vitro studies for osteoconduction | ||||
| MBCP Plus | Granule | β-TCP (80%)+HA (20%) | Sinus lift augmentation | 70% porosity with 35% microporosity | Permeable | Human study (level IV: extraction socket84) |
| Ridge augmentation | 1/3 micropores (<10 μm) | Resorbable | Animal, in vivo, in vitro for osteoconduction | |||
| Alveolar regeneration | 2/3 macropores (300-600 μm) | Hydrophilic | ||||
| Alveolar regeneration | Bioactive | |||||
| Intra-osseous pockets | Osteoconductive | |||||
| Regeneration | ||||||
| NEW BONE | Granule | β-TCP (80%)+HA (20%) | Ridge augmentation | 80% porosity (pore size: 200-400 μm) | Osteoconductive synthetic bone graft | Animal study |
| Extraction site and osteotomy | 0.2-2.0 mm size of porous particles | Highly resorbable due to 80% β-TCP | ||||
| Cystic cavities | Easy manipulation | |||||
| Sinus lift | ||||||
| Periodontal defect | ||||||
| OSTEON | Granule/syringe | β-TCP (30%)+HA (70%) | Periodontal/infrabony defects | HA coated with β-TCP | Osteoconductive | Human study (level III: sinus lift94) |
| Ridge augmentation | Interconnected porous structure similar to that of human cancellous bone | Animal, in vivo, in vitro for osteoconduction | ||||
| Extraction site (implant preparation/placement) | 77% porosity (pore size: 300-500 | |||||
| Sinus lift | Irregular shaped particles of size | |||||
| Cystic cavities | Particle size (granule): 0.3-2.0 mm | |||||
| Particle size (sinus, syringe): 0.5-2.0 mm | ||||||
| Particle size (lifting, syringe): 0.3-1.0 mm | ||||||
| OSTEON II | Granule/syringe | β-TCP (70%)+HA (30%) | Periodontal/infrabony defects | Interconnected porous structure similar to that of human cancellous bone | Highly resorbable due to higher β-TCP content | Human study (level III: extraction socket99, level IV: sinus lift100, vertical ridge augmentation101, ridge augmentation102103, periodontal defect105) |
| Ridge augmentation | >70% porosity (pore size: 250 μm) | Easy manipulation | Animal, in vivo for osteoconduction | |||
| Extraction site (implant preparation/placement) | Irregular shaped particles of size | Excellent wettability | ||||
| Sinus lift | Particle size (granule): 0.2-2.0 mm | Osteoconductive | ||||
| Cystic cavities | Particle size (sinus, syringe): 0.5-2.0 mm | |||||
| Particle size (lifting, syringe): 0.2-1.0 mm | ||||||
| OSTEON III | Granule/syringe | β-TCP (40%)+HA (60%) | Periodontal/infrabony defects | Interconnected macro and micro porous structure | Biocompatible | Animal study (BMP carries) |
| Ridge augmentation | <80% porosity | Osteoconductive | ||||
| Extraction site (implant preparation/placement) | Particle size (granule): 0.2-2.0 mm | |||||
| Sinus lift | Particle size (sinus, syringe): 0.5-2.0 mm | |||||
| Cystic cavities | Particle size (lifting, syringe): 0.2-1.0 mm | |||||
| >70% crystallinity | ||||||
| CaP=1.59 | ||||||
| OSTEON III Collagen | Cylinder | β-TCP (40%)+HA (60%)+type I collagen (>95% porcine tendon collagen) | Alveolar bone defect | Particle size: 0.2-1.0 mm | Easy manipulation | NA |
| Excellent wettability | ||||||
| Ovis BONE BCP | Granule | β-TCP (80%)+HA (20%) | Periodontal bone defect | 70% porosity (pore size: 20 μm) | Osteoconductive | NA |
| Intrabony defect | Particle size: 0.3-2.0 mm | Excellent wettability | ||||
| Extraction site | Easy manipulation | |||||
| Ridge augmentation | Biocompatibility and great bioactivity | |||||
| Sinus lift | ||||||
| Cystic cavitiy | ||||||
| Q-OSS+ | Granule | β-TCP (80%)+HA (20%) | NA | Porous structure | Excellent hydrophilicity | Cell culture |
| Osteoconductive | ||||||
| Biocompatibile | ||||||
| Bioasorbable | ||||||
| Rapid osteogenesis rate | ||||||
| TOPGEN-S | Granule | β-TCP (80%)+HA (20%) | NA | Interconnected macro and microporous | Excellent hydrophilicity | NA |
| Particle size: 1.0-2.0 mm | Osteoconductive |
![]()
Table 8
Dental bone graft substitutes which was consisted with calcium phosphate
![]()
1. The products approved in FDA
Seven products were approved in FDA11121314151617.(Table 2) Although TCP Dental (Kasios SAS, L'Union, France) was not licensed for dental indication in intended use of FDA17. However, the authors included TCP Dental in this category because manufacturer did not distinguish between KASIOS TCP and (KASIOS) TCP Dental.
2. Registered in MOHW and commercially available information for product name, manufacturer, importer, and component
The details of dental alloplastic bone substitute which was approved by MOHW notification No. 2018-248 were analyzed8.(Table 3) Among them, BIO-C and OssPol-dental were officially discontinued. CollaOss (SK Bioland, Cheonan, Korea) is registered as 60% of HA, 0.3% of bovine-derived collagen (0.3%) and 39.7% of distilled water and as block, syringe and putty types. Currently, only bock and putty type are available in the manufacturer. DualPor COLLAGEN D-PUTTY and DualPor COLLAGEN D-INJECTION is available as DualPor Collagen D-Putty and DualPor Collagen Injection, but no any information could be found.
There are seven products that do not match the manufacturer or importer registered in MOHW: (1) MBCP+ (Biometlante, Vigneux-de-Bretagne, France; sold only as MBCP and MBCP syringe type, not MBCP+), (2) Excelos Inject (Bio-Alpha, Seongnam, Korea; produced by CGbio, Seongnam, Korea), (3) Excelos (TCPGLD) (BioAlpha; produced by CGbio, sold exclusively by Excelos), (4) Boncel-Os (BioAlpha; produced by CGbio), (5) Mega-TCP (manufactured by CGbio; MegaGen, Seoul, Korea, sold as a single product without discrimination between CGM and CGL), (6) Cerasorb and Cerasorb M granule (sold only by Curasan, Kleinostheim, Germany: Cerasorb M, registered as importer) BI Trading currently available is not available), and (7) OSTEON Sinus (GENOSS, Suwon, Korea: sold as syringe type of OSTEON I, II, or III).(Table 3)
CollaOss is listed as a dental synthetic bone in the MOHW and HIRA data. Although it was represented as xenograft in the journal18192021; however, it was included in this review.(Table 3)
There are three products that do not match in the component registered in MOHW: (1) Cerasorb M granules (99% β-TCP not β-TCP combined with HA; Curasan), (2) FRABONE-Inject (Inobone, Cheonan, Korea: hyaluronic acid addition with HA+β-TCP), and (3) TCP Dental (99% β-TCP not 95% β-TCP combined with 5% HA).(Table 3)
As a result, out of the 33 dental bone substitutes that are currently registered in MOHW and HIRA, 28 products could be commercially available when considering the products that are different form registered information as below: Excelos (TCPGLD) and Excelos (TCPGMD, TCPGLD) are sold exclusively by Excelos, Mega-TCP (CGL) and Mega-TCP (CGM, CGL) are sold only by Mega-TCP, Cerasorb and Cerasorb M granules are sold by Cerasorb M, Cerasorb M is 99% β-TCP, FRABONE-Inject is sold by adding hyaluronic acid, CollaOss is sold in putty and block form without syringe type, DualPor COLLAGEN D-INJECTION is not produced, and TCP Dental (99% β-TCP).
3. Analysis of dental alloplastic bone substitutes according to constituents
The main components of dental alloplastic bone substitute are tricalcium phosphate (Ca3(PO4)2, β-TCP), calcium phosphate (CaP), and hydroxiapatitie (Ca10(PO4)6(OH)2, HA) which is crystalline form of CaP.(Table 4)
1) Dental alloplastic bone substitutes consist of hydroxyapatite
HA is an inorganic material which account for 65% of bone matrix and can be classified as dense and porous, sintered ceramic and non-ceramic, and bovine, coralline and synthetic depending on the origin. Typical characteristics are as below. (1) As large as the particle size, it remains for a long time with slow absorption. (2) The higher the porosity, the easier the penetration of new bone and the quicker absorbed. (3) The larger the crystallinity, the longer the absorption period. (4) Rigid and dense block-form products have high compressive strength but are susceptible to fracture. (5) The higher the porosity, the lower the strength5.
Among the dental alloplastic bone substitutes allowed for use in Korea, there were four products that consisted of HA. OssaBase-HA (LASAK, Praha, Czech) has a retrospective study of guided bone regeneration in 2018, but it was obtained human study level IV due to a poor study design22. However, many other animal, in vivo, and in vitro studies for osteoconductivity23242526. No journals were found for Ovis BONE HA (DENTIS, Seoul, Korea). CollaOss consists of 90% porcine-deriven HA and 10% porcine deriven collagen. It was classified as alloplastic graft in MOHW and HIRA, on the other hands, it was introduced as xenograft in many studies18192021. In the manufacturer (SK Bioland), it is commercially available in plug type and putty type. In comparison with the collagenated bovine bone (Bio-Oss collagen; Geistlich Biomaterials, Woulhusen, Switzerland) into the extraction socket, it was received the human study level III because there was no difference in the efficacy18. Human study level IV was received in a clinical study to comprare the effects of membranes on peri-implant defect19. Animal studies showed osteoconductivity2021.(Table 4)
2) Dental alloplastic bone substitutes consist of tricalcium phosphate
TCP has a composition of calcium and phosphorus in ratio of 3 and 2. It was known as partially transition into HA and absorption in vivo, but various absorption periods of three to 24 months have been reported depending on the products. The rate of absorption varies according to the chemical structure, porosity and particle size of the material5. The general characteristics suggested by the manufacturer of TCP are as follows. (1) Use with platelet-rich plasma is effective. (2) It is absorbed at the same time as new bone graft. (3) Due to the interconnection of the pores, bone fibers are rapidly penetrated and could promote the regeneration. (4) Since the particle is rounded, there is little mechanical irrigation in surrounding tissues and little inflammatory reaction. (5) High mechanical stability prevents early collapse and inhibits undesirable macrophage activity.
Of the approved products for Korean dental alloplastic bone substitute, seven products that consist with TCP were commercialization. BoneSigma TCP (SigmaGraft, Fullerton, CA, USA) has been described as one of the in vitro studies27, and clinically available products2829 but no clinical studies have been published. Excelos is registered as β-TCP etc. in MOHW and has two types of powder and injection and registered. Injection type is a mixture of biodegradable polymers such as poloxamer and hydroxypropyl methylcellulose (HPMC) to enhance injectable property, moldability and hemostasis. A clinical study comparing putty type Excelos with extraction and using as BMP carriers received a human study level IV30. Excelos has animal studies for BMP carrier3132 and in vivo study for osteoconduction33. No journals were found for Mega-TCP. Sorbone (META-BIOMED, Cheongju, Korea) was validated and received human study level II by a split-mouth study as a control of cockle-shell bone substitute in socket preservation34, and used as a control material for the effect of alendronate on periodontal intra-osseous defect35. SynCera (Oscotec, Seongnam, Korea) had animal and in vivo study for osteoconductivity3637. Cerasorb was approved by the FDA and commercially available to Cerasorb M which reduced porosity from 80% to 65%11. It was received human study level I by randomized controlled trial and systematic review that was equivalent to an autogenous graft in sinus lift3839. It was received human study level III in cystic lesion, periodontal defect and cleft alveolus40. Also, as a result of histologically sufficient alveolar bone regeneration, human study level III was obtained in extraction socket41. As human study level IV, it was used with an enamel matrix derivative in the periodontal defect4243, peri-implant defect after immediately implantation after extraction44, every lots of animal, in vivo, and in vitro studies for osteoconduction6454647484950515253545556. TCP Dental was registered as 5% of HA and 95% of β-TCP in MOHW and HIRA. However, the manufacturer (Kasios SAS) and importer (B.IMTECH, Yongin, Korea) advertised as 99% of β-TCP. Many studies and FDA 510(k) also represented as β-TCP17575859606162636465. It was received human study level III by successful histologic and clinical result comparing Xenograft (BonePlus-xs; Integros, Adana, Turkey) in sinus lift57. Animal, in vivo, and in vitro studies for osteoconductivity5859606162636465.
3) Dental alloplastic bone substitutes consist with hydroxyapatite and tricalcium phosphate
The mixing ratio of HA and TCP varies from 2:8 to 7:3. It has the following characteristics. (1) It has micropore and macropore. They could induce effective tissue reaction and growth of new bone tissue. Micropores could enable ion exchange and form new contact surfaces for cell adhesion through the deposition of bone crystals. Macropores could help in angiogenesis and remodeling and growth of new bone. (2) HA acts as a mechanical support until the new bone tissue could be remolded for structural stability, and TCP could spread the adhesion surface of osteoblast by ion exchange through rapid resorption. (3) It has porosity of 70% to 90%5.
Boncel-Os (CGbio) consists with 30% of HA and 70% of β-TCP. It was introduced as one of the clinically available products66, and there is an animal study used as a BMP carrier56. BoneSigma BCP (SigmaGraft) consists with 60% of HA and 40% of β-TCP. In vivo study has been published that it inhibited osteoclast formation with plate-rich fibrin67. Dualpore Collagen D-Putty was registered as 60% of HA, 0.3% of bovine-derived collagen, and 39.7% of distilled water by the MOHW and HIRA. On the other hand, the manufacturer (OssGen) advertised the product as 60% HA and 40% β-TCP in 94.5% of biphasic CaP, and with an additional 5.5% bovine collagen but there are no reports of any evaluations of the evaluating its information provided. In MOHW and MFDS, Inobone has registrated its products as FRABONE DENTAL and FRABONE DENTLA INJECT, but they are commercially available as FRABONE and FRABONE-Inject. FRABONE (Inobone) consists with 60% of HA and 40% of β-TCP and it was received patent in USA, Germany, and Korea as mimic the harversian canal structure6869. FRABONE-Inject (Inobone) is a product of hyaluronic acid addition to FRABONE, which advertised to increase moldability and absorption rate by act as soluble granules of hyaluronic acid. However, there was no related researched were found. GENESISBCP (DIO, Busan, Korea) consists with 60% of HA and 40% of β-TCP. It was received human study level II by prospective controlled clinical trial which results good outcome in periodontal defect70. In horizontal augmentation, it was showed successful result with NanoBone (HA and silica gel matrix; Artoss GmbH, Warnemünde, Germany) in case report and it obtained human study level IV71. There were many animal, in vivo, and in vitro studies for osteoconductivity727374757677. Manufacturers have the two types of MBCP as combination of HA and β-TCP as ratio as 60:40 and 20:80, and a moldable MBCP (In'Oss) made by mixing hydrogel to MBCP. However, represented importer (Purgo Biologics, Seongnam, Korea) only has granule or syringe type of MBCP+ which consists with 20% of HA and 80% of β-TCP. MBCP and MBCP+ were received in FDA 510(k) approved1216. There were many clinical studies from MBCP which consists with 60% of HA and 40% of β-TCP78798081828384. On the other hand, MBCP+ was published only animal studies85868788 and in vitro studies8990. Although not introduced as MBCP+, a combination of 20% of HA and 80% of β-TCP was as same resorption and bone growth as combination of 60% of HA and 40% of β-TCP in retrospective clinical trial for extraction socket and it could be human study level IV84. Newbone (GENOSS) consists with 20% of HA and 80% of β-TCP. Although there were animal and in vivo studies for osteoinductivity919293, no clinical studies were found. Boncel-Os consists with 30% of HA and 70% of β-TCP. It was introduced as one of clinically available products66 and used as BMP carrier in animal study56.
OSTEON series (GENOSS) were available as vial, sinus, and lift type. OSTEON, OSTEON II, and OSTEON III were received FDA 510(k) approval131415. In registration of MOHW and HIRAO, OSTEON and OSTEON Sinus were separated but OSTEON Sinus is not available product to commercially use. The manufacture (GENOSS) has classified OSTEON Sinus and OSTEON Lifting according to the size of syringe. In FDA 510(k), there also received approval as same as OSTEON, OSTEON Sinus, and OSTEON Lifting13. OSTEON consists with 70% of HA and 30% of β-TCP. In retrospective clinical study for sinus lift, OSTEON alone could result well-developed lamellar bone as same as Xenograft (Bio-Oss; Osteohealth, Shirley, NY, USA) and it could be received human study level III94. There were many animal and in vivo studies for osteoconductivity95969798. OSTEON II consists with 30% of HA and 70% of β-TCP. In retrospective clinical study for extraction socket, OSTEON II and OSTEON II Collagen were significantly more effective than collagen or native defect and the histological result was shown in animal studies99. Therefore, it could be received human study level III in extraction socket. It was received human study level IV by retrospective study as control group for sinus lift100, 6 months after vertical augmentation which particulated OSTEON II was showed no significantly difference on volume change and peri-implant marginal bone loss compared with autogenous block and allogenous block bone101, successful results on clinical and histologically in ridge augmentation102103, successful outcome on graft after implant removal104, and clinically effective on periodontal defect105. Many animal and in vivo studies for osteoconductivity959697106107. OSTEON III consists with 60% of HA and 40% of β-TCP. There was animal study as BMP carrier108. Although there was no OSTEON III Collagen related study, OSTEON II Collagen had animal and in vivo studies for osteoconductivity109110. Ovis BONE BCP (DENTIS) consists with 20% of HA and 80% of β-TCP. No journals were found for Ovis BONE BCP. Q-Oss+ (OSSTEM IMPLANT, Seoul, Korea) consists with 20% of HA and 80% of β-TCP. It was received human study level IV by the clinical study on peri-implant defect111. There were in vivo study for osteoconductivity112 TOPGEN-S (Toplan, Seoul, Korea) consists 20% of HA and 80% of β-TCP and there could not be found for journals for TOPGEN-S.
Go to :
IV. Discussion
Commercially available dental alloplastic bone substitute which was approved MOHW notification No. 2018-248 were broadly divided into 4 groups as C group (bone union and fixation group), L group (general materials), T group (human tissue), and non-insurance group. In the subcategory, there were C0 group (bone substitutes: xenograft, alloplastic graft), L7 group (dental material: dental xenograft, dental alloplastic graft), TB group (bone, demineralized bone matrix, bone block, bone chip, bone powder), non-insurance group (treatment material, human-derived bone, bone substitute containing bone morphogenetic protein [rhBMP-2])8. Among them, dental alloplastic bone substitutes in L7 of L group were included in this study.
The post-application management is obligatory for the manufacturer (or representative importer) to receive a certification of GMP by MFDS. According to FKDS No. 2016-156 of ‘medical device manufacturing and quality control standards’, the certification of GMP of human tissue or functional replacement product should be renewed every three years in article 9. According to article 10 of KFDS No. 2016-156, the certification of GMP should be reissued when any information for the products changed (change of the name of the importer or manufacturer, change of location of the importer or manufacturer). In article 12 and 15, the quality control examination agency reports periodic on the compatibility of medical device to director of KFDA7. Therefore, the manufacturer or importer of registered in the MFDS could be important factors in terms of quality control of currently available bone substitutes.
However, nineteen products (51.4%) were different information among the 37 products registered in MOHW. Four products (10.8%) were different registered ingredients from journal or advertisement including DualPor COLLAGEN D-PUTTY (OssGen), Cerasorb M granules, FRABONE-Inject, and TCP Dental. Nine products (24.3%) were differ in product name or not available including CollaOss (Syringe), Mega-TCP (CGL), Cerasorb, Cerasorb M granules, BIO-C, Excelos (TCPGMD, TCPGLD), MBCP Plus (Biometlante), OssPol DENTAL, and OSTEON Sinus. Especially, CollaOss (Block) and CollaOss (Putty) were registered as dental alloplastic bone substitute in MOHW but they were introduced as xenograft in advertisement and journals. Five products (13.5%) had different manufacturer or importer including Excelos Inject (CGbio), Excelos (TCPGLD), Excelos (TCPGMD, TCPGLD), Mega-TCP (CGM, CGL), Boncel-Os.
For a successful clinical outcome, it cannot be overemphasized that the quality of the materials or medical device should be constant and strictly controlled. Unfortunately, it is hard to identify the certification of GMP or to verify the quality in every clinical situation. Therefore, it is necessary to leave certificate to the government agency or the company which is responsible for the product. In addition the related dental institute or academy should to consider the security on quality of the product.
Implant dentistry has become a common treatment in Korea, many studies and development have been made on implant and bone graft materials. Among dental alloplastic bone substitutes which were registered in MOHW, twenty-nine (78.4%) products were domestically produced, of which three out of seven approved by FDA were made in Korea11121314151617. However, there are only ten products (27.0%) have been published with clinical study, of which six are Korean products. In the view of reference, the reference level could not be as directly same as the efficiency of the product, but it could be the basis of product selection for the clinician since minimal safety and efficiency can be regarded as verified. Reference level I received Cerasorb M (β-TCP 99%) as a sinus lift3839. Reference level II received Sorbone (β-TCP 100%) in extraction socket and periodontal defect3435, GENESIS-BCP (β-TCP 40% and HA 60%) in periodontal defect70. Reference level III received Cerasorb M (β-TCP 99%) in cystic cavity, periodontal defect, cleft defect and extraction socket4041, CollaOss (HA 90% and collagen 10%) in extraction socket18, OSTEON (β-TCP 30% and HA 70%) in sinus lift94, OSTEON II (β-TCP 70% and HA 30%) in sinus lift99, TCP Dental (β-TCP 99.9%) in sinus lift57. Reference level IV is insufficient to verify the efficiency, could be seen as a step that clinically confirms safety. Cerasorb M was in peri-implant and periodontal defect424344, CollaOss was in peri-implant defect19, OssaBase-HA (HA 100%) was in guided bone regeneration22, Excelos (β-TCP 100%) was in extraction socket30, MBCP+ (β-TCP 80% and HA 20%) was in extraction socket84, GENESISBCP was in ridge augmentation71, OSTEON II was in sinus lift100, ridge augmentation101102103, periodontal defect105 achieved for reference level IV. In addition, there were many animal, in vivo, and in vitro studies for osteoconductivity or role as carrier of osteoinductive growth factors or control material. In order to obtain MOHW and MFDS approval for commercial use in Korea, a data based on research or experiments should be required, but these data could not be included in this study because they were not publicly available. Because dental bone graft surgery has been performed in various environments such as sinus lift, ridge augmentation, cystic lesion, periodontal defect, peri-implant defect, extraction socket, it could be difficult to obtain high reference level in all dental bone grafting fields. However, it is nevertheless necessary to demonstrate the clinical level of Korean dental operation and the development level of bone graft substitutes.
In conclusion, there is not enough information about the effectiveness and safety of currently available alloplastic bone substitute in dental performance. Further clinical trials including well designed RCTs are necessary to evaluation the clinical efficacy of dental alloplastic bone substitutes in Korea. It should be aware of the limited information and developed the clinical evidences and regulations for clinicians.
Go to :
 XML Download
XML Download