

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The global spread of carbapenemase-producing Enterobacteriaceae, P. aeruginosa, and Acinetobacter species is a critical medical and public health issue causing both nosocomial and community-acquired infections [12]. Carbapenems are key antimicrobials in the clinical field, as they are considered the final line of defense against multidrug-resistant (MDR) gram-negative bacilli (GNB) infections [345]. Resistance to carbapenems mediated by the acquisition of carbapenemase production is increasingly reported [6]. Carbapenemese production by bacterial hosts induces resistance to nearly all β-lactam drugs and is associated with MDR phenotypes [7]. Therefore, the dissemination of carbapenemase-producing organisms (CPO) is considered a public health emergency in Korea, especially following outbreaks of Klebsiella pneumoniae carbapenemase-2 (KPC-2)-producing Klebsiella pneumoniae in 2011 and carbapenemase-producing carbapenem-resistant Acinetobacter baumannii in 2004 [89]. The potential for further escalation of this scenario should not be ignored, as these genes are associated with mobile genetic elements, and the emergence of novel enzyme types and variants is expected [7]. Thus, rapid and accurate detection of antimicrobial resistance and resistance mechanisms is important to prevent the dissemination of MDR bacteria [10].
Carbapenemases are usually classified into three classes of β-lactamases (according to their amino acid identity): Ambler class A (serine-β-lactamases), B (metallo-β-lactamases; MBLs), and D (oxacillinases; OXAs) β-lactamases. In addition, Ambler Class C β-lactamase (AmpC β-lactamase) could induce resistance to carbapenems in bacterial hosts, when accompanied with additional resistance mechanisms such as porin loss [111213].
Ceftazidime-avibactam was recently introduced as a new compound combining ceftazidime and a novel β-lactamase inhibitor with activity against various β-lactamases produced by MDR GNB [14]. Avibactam was first reported in 2003; it is a β-lactamase inhibitor against Ambler class A and C β-lactamases, and this agent also possesses activity against some of Ambler class D enzymes [1516]. The addition of avibactam to ceftazidime improves its in vitro activity against Enterobacteriaceae and Pseudomonas aeruginosa [17]. Recent study has revealed that ceftazidime-avibactam exhibits a good outcome to treat patients infected with KPC-producing strains [18].
The BD Phoenix NMIC-500 panel (BD Diagnostic Systems, Sparks, MD, USA) has been designed with advantageous properties for determining carbapenem minimum inhibitory concentrations (MICs), as well as CPO detection, compared with a previous panel [GN-27 NMIC203 (BD Diagnostic Systems)] [19]. By including CPO detection and ceftazidime-avibactam MIC determination in routine antimicrobial susceptibility testing (AST), the BD Phoenix NMIC-500 panel could offer valuable support for clinical studies examining different therapeutic strategies for infections caused by CPOs. To our knowledge, the performance of this panel has not been evaluated so far. We evaluated the performance of the BD Phoenix NMIC-500 panel for AST and CPO detection with clinical GNB isolates.
Go to : 
METHODS
Bacterial strains
A total of 450 non-duplicate clinical GNB isolates collected from six general hospitals in Korea from May 2016 to April 2017 were used (409 Enterobacteriaceae isolates [225 K. pneumoniae, 133 E. coli, 36 Enterobacter, nine Citrobacter freundii, five Raoultella, and one Klebsiella oxytoca isolates] and 41 glucose-non-fermenting gram-negative bacilli [GNFB] isolates, including 21 P. aeruginosa and 20 A. baumannii isolates). The isolates were inoculated in a cryotube containing 20% (w/v) skimmed milk and stored at −80℃, and then transferred for the analysis; the performance of the BD Phoenix NMIC-500 panel was evaluated at a single center from January 2018 to May 2018. This study was exempted from approval by the Ethics Committee on Human Research of the Health Ministry in Korea.
BD Phoenix analysis
AST was conducted according to the manufacturer's instructions. Briefly, the identification (ID) broth was inoculated with bacterial colonies from pure cultures adjusted to 0.5–0.6 McFarland (McF) standard using a Phoenix spectrophotometric device. The standardized ID broth suspension (25 µL) were transferred to the Phoenix AST broth, which was supplemented with one drop of the Phoenix AST indicator for detecting organism growth before being added to the panels. The panels were sealed, logged, and loaded into the Phoenix device. The results were interpreted using Epicenter data management software version 7.22A (BD Diagnostic Systems) after 16 hours of incubation.
Reference methods
The meropenem (range: 0.5–256 mg/L), imipenem (range: 0.5–256 mg/L), ertapenem (range: 0.125–16 mg/L), ceftazidime (range: 0.125–16 mg/L), and ceftazidime-avibactam (range: 0.125/4–8/4 mg/L) MICs of 450 GNB isolates were determined using the broth microdilution (BMD) method following the CLSI guidelines with Mueller-Hinton broth (Difco Laboratories, Detroit, MI, USA) [20]. E. coli ATCC 25922 and P. aeruginosa ATCC 27853 were used as control strains, as recommended by the CLSI.
PCR and sequencing were performed for the carbapenem-resistant GNB isolates to identify the carbapenemase genes including KPC, New Delhi metallo-β-lactamase (NDM), imipenemase (IMP), Verona integron-borne metallo-β-lactamase (VIM), OXA-48-like, and OXA-23. PCR was performed using the following amplification conditions: 94℃ for five minutes, followed by 30 cycles of 94℃ for 30 seconds, 58℃ (KPC) or 60℃ (OXA-48-like, IMP, VIM, and NDM) for 30 seconds, and 72℃ for 30 seconds, followed by a final extension at 72℃ for five minutes. To confirm the amplified products, they were directly sequenced using an automatic sequencer (model 3730xl; Applied Biosystems, Weiterstadt, Germany). The oligonucleotide sequences of the primer used are summarized in Table 1.
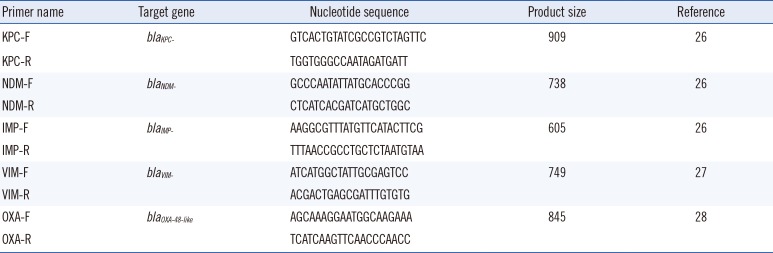
Table 1
Oligonucleotide sequences of the primers used in this study
![]()
Data analysis
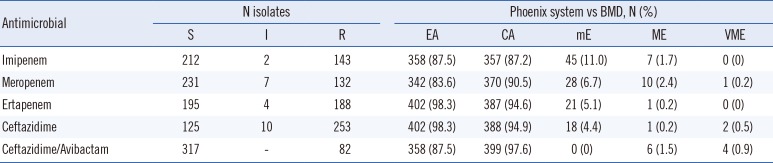
The accuracy of the BD Phoenix NMIC-500 panel was calculated using categorical agreement (CA), essential agreement (EA), minor error (mE), major error (ME), and very major error (VME), which were determined by comparing its MIC results to the BMD results according to the CLSI breakpoints [21]. The Phoenix system results were considered CA if they agreed with the susceptible, intermediate, and resistant categories of the BMD results. Results were deemed EA when the MIC results using the BD Phoenix NMIC-500 panel and BMD were identical or 2-fold different. Results were deemed mE when one set of the AST results was intermediate while the other set was resistant or susceptible. Results were deemed ME when the Phoenix system MIC results were resistant, while the BMD results were susceptible. Results were deemed VME when the Phoenix system indicated susceptibility and the BMD indicated resistance.
The accuracy of CPO detection was determined as follows: carbapenemase production was considered positive when the Phoenix system results showed “carbapenemase producer,” “class A carbapenemase producer,” “class B carbapenemase producer,” or “class D carbapenemase producer”; otherwise, it was considered negative. In terms of CPO classification, “carbapenemase producer” were considered as “not classified.” In addition, “class A carbapenemase producer,” “class B carbapenemase producer,” and “class D carbapenemase producer” were considered as correctly classified when corresponding to the same class determined by conventional PCR, but were considered as incorrectly classified when corresponding to a different class.
Go to :
RESULTS
Enterobacteriaceae
Table 2 and Fig. 1 detail the AST results obtained using the BD Phoenix NMIC-500 panel and BMD with 409 clinical Enterobacteriaceae isolates. Most antimicrobials showed high CA and EA rates (>90%), except for imipenem, which showed a CA rate of 87.2%. In addition, only seven VME were observed, and the ME rates were 3%.
 | Fig. 1Enterobacteriaceae MICs determined using broth microdilution and the BD Phoenix NMIC-500 panel. The MICs of meropenem (A), imipenem (B), ertapenem (C), ceftazidime (D), and ceftazidime-avibactam (E) were determined using 409 clinical isolates; dark gray indicates identical agreement, and light gray indicates 2-fold difference between the BMD and NMIC-500 panel MICs. Dotted lines indicate the clinical breakpoints for each antimicrobial.Abbreviations: MIC, minimum inhibitory concentration; BMD, broth microdilution.
|
Table 2
AST results for Enterobacteriaceae
![]()
GNFB
Table 3 and Fig. 2 detail the CAs, EAs, as well as mE, ME, and VME numbers and rates for 41 clinical P. aeruginosa and A. baumannii isolates. High agreement was observed between the results of BD Phoenix NMIC-500 panel and BMD. The CA and EA rates were all >90%, ranging from 92.7% to 100% and from 97.6% to 100%, respectively, except for the EA of imipenem, which was 87.8%. Only one ME was identified for imipenem.

 | Fig. 2MICs of glucose-non-fermenting gram-negative bacilli determined using the broth microdilution method and the BD Phoenix NMIC-500 panel. The MICs of meropenem (A), imipenem (B), and ceftazidime (C) was determined with 20 Acinetobacter and 21 P. aeruginosa isolates. In the case of ceftazidime-avibactam (D), only P. aeruginosa was assessed. Dark gray indicates identical agreement, and light gray indicates 2-fold difference between the MICs determined using BMD and the BD Phoenix NMIC-500 panel. Dotted lines indicate the clinical breakpoints for each antimicrobial.Abbreviations: MIC, minimum inhibitory concentration; BMD, broth microdilution.
|
Table 3
AST results for glucose-non-fermenting gram-negative bacilli
![]()
CPO detection
Table 4 details the CPO results obtained by PCR/sequencing and the BD Phoenix NMIC-500 panel. The rates of correct identification in carbapenemase production were 98.6% (70/71) for the class A carbapenemase-producers, 98.1% (101/103) for class B carbapenemase-producers, and 96.7% (59/61) for class D carbapenemase producers. The rates for correct classification were 73.6% (184/250) in the carbapenemase-producers. In the 15 dual carbapenemase producers, 86.7% (13/15) were positive for carbapenemase production; however, the Phoenix system could identify only one class of carbapenemase between the two types of carbapenemases or could not identify the class of carbapenemase. In addition, most carbapenemase-nonproducers (99.5%, 199/200) were negative for carbapenemase production.
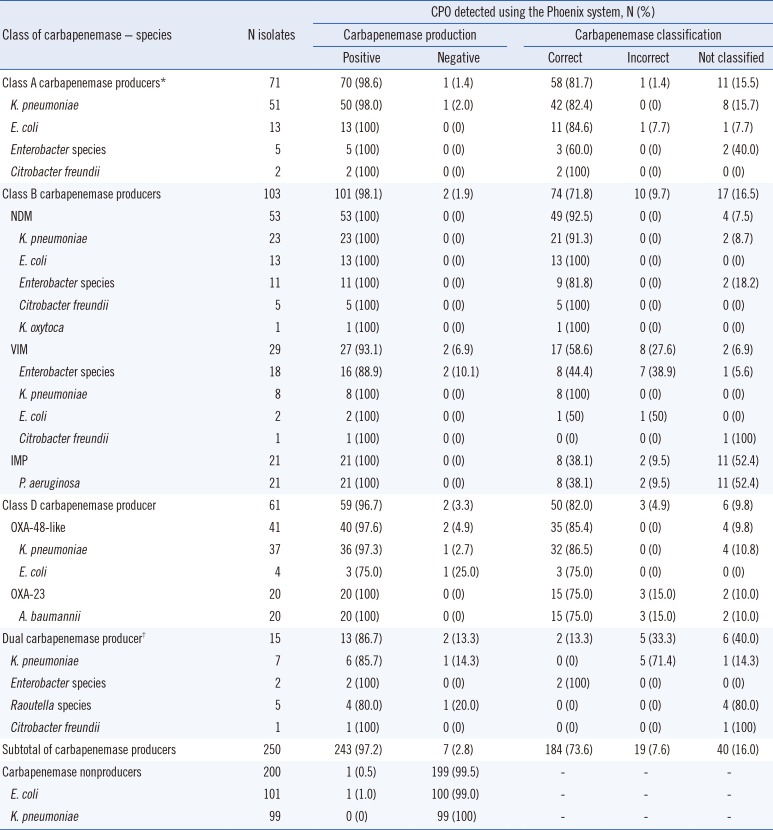
Table 4
CPO detection using the Phoenix system and PCR+sequencing
*All Class A carbapenemase producers were KPC-producers; †The 15 dual carbapenemase producers included seven KPC and NDM coproducers (one K. pneumoniae, one Citrobacter freundii, and five Raoutella species), six NDM and OXA-48-like coproducing K. pneumoniae, one IMP and VIM coproducing Enterobacter species, and one NDM and VIM coproducing Enterobacter species.
Abbreviations: CPO, carbapenemase producing organisms; KPC, Klebsiella pneumoniae carbapenemase; NDM, New Delhi metallo-beta-lactamase; VIM, Verona integron-borne metallo-beta-lactamase; IMP, imipenemase; OXA, oxacillinase.
![]()
Go to :
DISCUSSION
The carbapenem MICs obtained using the BD Phoenix NMIC-500 panel were higher than those obtained by BMD. The ME rates were slightly elevated, while VME was identified in only 1.5% (7/450) of all isolates. These results indicate high sensitivity of carbapenem resistance detection. Consistent with our results, Menozzi et al. [22] evaluated the previous AST panel of BD Phoenix system with identical bacterial species and reported that the EA and CA were 87.6% and 98.7%, 96.0% and 99.5%, and 95.8% and 98.7% for imipenem, meropenem, and ceftazidime, respectively, with clinical Enterobacteriaceae isolates, and 93.5% and 94.8%, 90.0% and 98.7%, and 94.8% and 97.4% for imipenem, meropenem, and ceftazidime, respectively, with clinical GNFB isolates.
The BD Phoenix NMIC-500 panel showed high performance for CPO detection. Consistent with our results, Thomson et al. [23] evaluated the BD Phoenix CPO Detect system (BD Diagnostic Systems), which is an AST panel similar to the BD Phoenix NMIC-500 panel, and showed that 97.3% (107/110) of class A carbapenemases, 95.6% (87/91) of class B carbapenemases, and 100% (35/35) of class D carbapenemases were positively identified. However, although the dual carbapenemase producers were positively identified, the system could not classify them. In the same study, Carba NP (bioMérieux, St. Louis, MO, USA) could positively identify 98.2% of class A, 98.9% of class B, and 94.3% of class D producers, as well as the dual carbapenemase producers. Although Carba NP showed high CPO detection performance, this kit required extra time for AST. In addition, Carba NP requires a chromogenic medium, which exhibits different shades of color that could be challenging for laboratory staff to interpret. In contrast, the BD Phoenix NMIC-500 panel was easier to interpret as it does not require a chromogenic medium, and CPO detection was more rapid.
The BD Phoenix NMIC-500 panel could identify carbapenemase production in 86.7% (13/15) of the dual carbapenemase-producing isolates; however, it could identify only one class of carbapenemase out of two in dual carbapenemase producers. Moreover, the remaining two isolates, which were correctly identified by the BD Phoenix NMIC-500 panel, harbored two carbapenemase genes within the same class. Thomson et al. [23] also suggested that most dual carbapenemase producers were not correctly identified using the BD Phoenix CPO Detect and that this should be improved in subsequent panels.
Ceftazidime-avibactam is the most active compound tested against KPC-producing isolates. Ceftazidime-avibactam was introduced to treat infections caused by KPC-producers, and its ability has been demonstrated [2425]. Our results showed that ceftazidime-avibactam could suppress the action of 94.4% (67/71) of KPC-producing isolates. Thus, ceftazidime-avibactam has potential to combat carbapenem-resistant Enterobacteriaceae.
A limitation of this study was that carbapenemase-non-producing carbapenem-resistant organisms were not included to evaluate the accuracy of CPO detection. This should be further investigated to confirm the accuracy of this panel.
In conclusion, the BD Phoenix NMIC-500 panel showed promising ability for MIC determination and CPO detection in a large number of clinical GNB isolates. The BD Phoenix NMIC-500 panel showed high agreement with conventional methods. By including carbapenemase detection and ceftazidime/avibactam MIC determination in routine AST, the BD Phoenix NMIC-500 panel offers valuable support for clinical studies examining different therapeutic strategies for infections caused by such organisms. This capability, in conjunction with good infection control, can help ensure that medical institutions are at minimal risk of a CPO pandemic.
Go to :
 XML Download
XML Download