

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sepsis is a life-threatening organ dysfunction caused by a dysregulated host response to infection. Septic shock is a subset of sepsis, in which underlying circulatory and cellular metabolic abnormalities are profound enough to substantially increase mortality [1]. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) identify organ dysfunction as an acute change in the total sequential (sepsis-related) organ failure assessment (SOFA) score ≥2 points [1]. The SOFA scoring system has been used to describe organ dysfunction and failure in septic patients since first introduced in 1996 [2]. A higher SOFA score for each organ is associated with an increased probability of mortality [12].
However, SOFA score could not be used to separate mortality in terms of cardiovascular status and coagulation system in the European-North American Study of Severity Systems [34]. Although it is preferable to avoid treatment-related criteria, the SOFA cardiovascular subscore is based on the requirement for adrenergic support, and the type of adrenergic support may differ across institutions [25]. Considering these innate limitations of the SOFA scoring system, it remains necessary to find a substitute for it or modify its use in evaluating septic patients, by using objective and reliable biomarkers.
Adrenomedullin (ADM), a newly identified neurohormonal system, is a 52-amino acid vasoactive peptide hormone that is encoded by the ADM gene on chromosome 11p15.4, containing four exons and three introns in humans [678]. ADM is expressed in all tissues, mainly by endothelial cells and vascular smooth muscle cells, and can regulate vasodilation and vascular integrity [78]. The endogenous ADM concentration increases nonspecifically under various conditions, such as over-hydration, hypertension, ischemia, septic shock, and endocrine and metabolic disorders [591011]. ADM has emerged as an independent prognostics biomarker especially in heart failure and/or sepsis [5121314].
Recently, a double monoclonal sandwich immunoassay has been developed to measure C-terminal amidated biologically active ADM (bio-ADM) [15]. Recent studies have demonstrated the association between bio-ADM concentration and hemodynamic support requirement, as well as its short-term prognostic values in sepsis [161718]. We explored whether bio-ADM concentration could predict sepsis severity, organ failure, and 30-day mortality in septic patients. We hypothesized that bio-ADM could play a prognostic role in sepsis and serve as a potential substitute for the SOFA score in evaluating septic patients.
METHODS
Study population
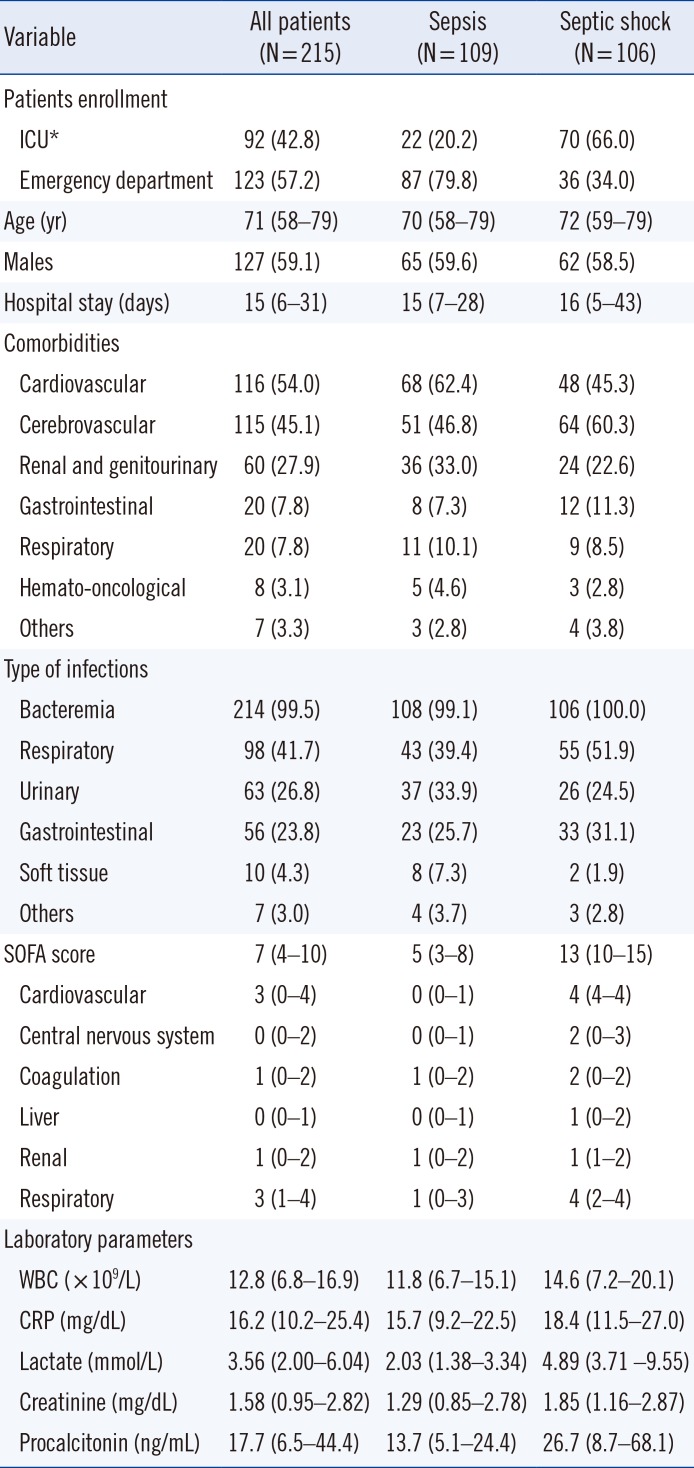
A total of 245 consecutive patients were diagnosed as having sepsis according to the Sepsis-3 definition at Konkuk University Medical Center (KUMC), Seoul, Korea, from August 2016 to August 2017 [1]. After excluding 30 patients without available leftover samples, we recruited 215 patients; 109 patients (50.7%) were diagnosed as having sepsis and 106 patients (49.3%) were diagnosed as having septic shock. These patients received proper and standard-of-care treatment according to the guidelines [1920]. Their medical records were reviewed retrospectively for demographic, laboratory, and clinical data, including age, sex, hospital stay, comorbidities, and clinical outcomes. The baseline characteristics of the study population are summarized in Table 1.
This registry study protocol was approved by the Institutional Review Board of KUMC, prior to the collection of the first sample from the first patient. This study did not require any study-intended blood sampling or other interventions. In all septic patients, routine laboratory parameters were measured on the day when the patients were diagnosed as having sepsis; the SOFA score was assessed on the same day (within 24 hours of sepsis diagnosis) in six different organ systems (respiratory, cardiovascular, hepatic, coagulation, renal, and neurological) and assigned a value from zero (normal) to four (high degree of failure) [2]. Residual blood samples were collected for measuring bio-ADM concentration. Attending clinicians (in the intensive care unit [ICU] or emergency department [ED]) made a clinical diagnosis of sepsis according to the Sepsis-3 definitions [1], decided on the enrollment of the patients in this study, and then informed the laboratory to store residual EDTA plasma after routine blood testing. Therefore, written informed consent from the patients was exempted.
Assay
The samples were split into small aliquots to avoid repeated freezing and thawing, frozen within two hours, and stored at −70℃ until use. Frozen samples were sent to the reference laboratory (Sphingotec GmbH, Hennigsdorf, Germany) after being anonymized and blinded, and then thawed at room temperature and gently mixed for at least 30 minutes just before measuring bio-ADM concentration. Plasma bio-ADM concentrations were measured according to the manufacturer's instructions as described previously [111621]. Briefly, this is a one-step sandwich chemiluminescence immunoassay based on acridinium NHS-ester labeling for the detection of human ADM in unprocessed plasma, which uses two mouse monoclonal antibodies: one directed against the middle region of ADM (solid phase) and the other directed against the amidated C-terminal moiety of ADM (labeled antibody). The immunoassay employs 50-µL plasma samples or calibrators and 200 µL labeled detection antibody (800,000 relative light units per 200 µL). The sample and antibody are added to the coated tubes, incubated for 18 hours at 4℃, and washed five times with washing solution (1 mL each). Next, chemiluminescence is measured for one second using an LB953 Multi-Tube Luminometer (Berthold Technologies GmbH & Co KG, Bad Wildbad, Germany) [22]. The analytical sensitivity is 2 pg/mL; the median concentration of bio-ADM based on 200 reference individuals was 20.7 pg/mL, and the 99th percentile was 43 pg/mL [1623]. The manufacturer-claimed and previously reported medical decision point is 70 pg/mL [16172123].
Statistical analysis
Data were generated as median and interquartile range (IQR) or number and percentage. Mann-Whitney test was used to compare two patient groups according to sepsis severity (sepsis vs septic shock), vasopressor use, and survival. The chi-squared test was used to compare bio-ADM quartile groups (from Q1 to Q4) according to the number of organ failures included in the SOFA scoring system (from zero to six) and SOFA subscores.
The chi-squared test was also used to compare the 30-day mortality rate according to bio-ADM quartiles, SOFA cardiovascular subscores, and lactate quartiles. Kaplan-Meier survival curves and hazard ratios (HRs) with 95% confidence intervals (CIs) were compared between each group created according to bio-ADM quartile, SOFA cardiovascular subscore, and lactate quartile for predicting 30-day mortality. The patients were divided into two groups using the medical decision point of 70 pg/mL, and Kaplan-Meier survival analysis was performed to compare these two groups for predicting 30-day mortality. These analyses were conducted for all patients as well as within the sepsis and septic shock groups.
ROC curves of bio-ADM concentration and SOFA score were used to derive the optimal cut-off values to predict 30-day all-cause mortality; optimal cut-off values were indicated where the sum of the false positive and false negative results was lowest. Using optimal cut-off values, the areas under the curves (AUC) were compared with their 95% CIs. Cox proportional hazard regression was used to analyze the effect of bio-ADM concentration and SOFA score on 30-day all-cause mortality; univariate relative risk (RR) with 95% CI of the variables and P values were obtained.
MedCalc Statistical Software version 18.6 (MedCalc Software Bvba, Ostend, Belgium) and R version 3.3.1 (R Foundation for Statistical Computing, Vienna, Austria) were used for statistical analyses. P values were not adjusted for multiple comparisons and therefore were only descriptive.
RESULTS
Prediction of sepsis severity and organ failure
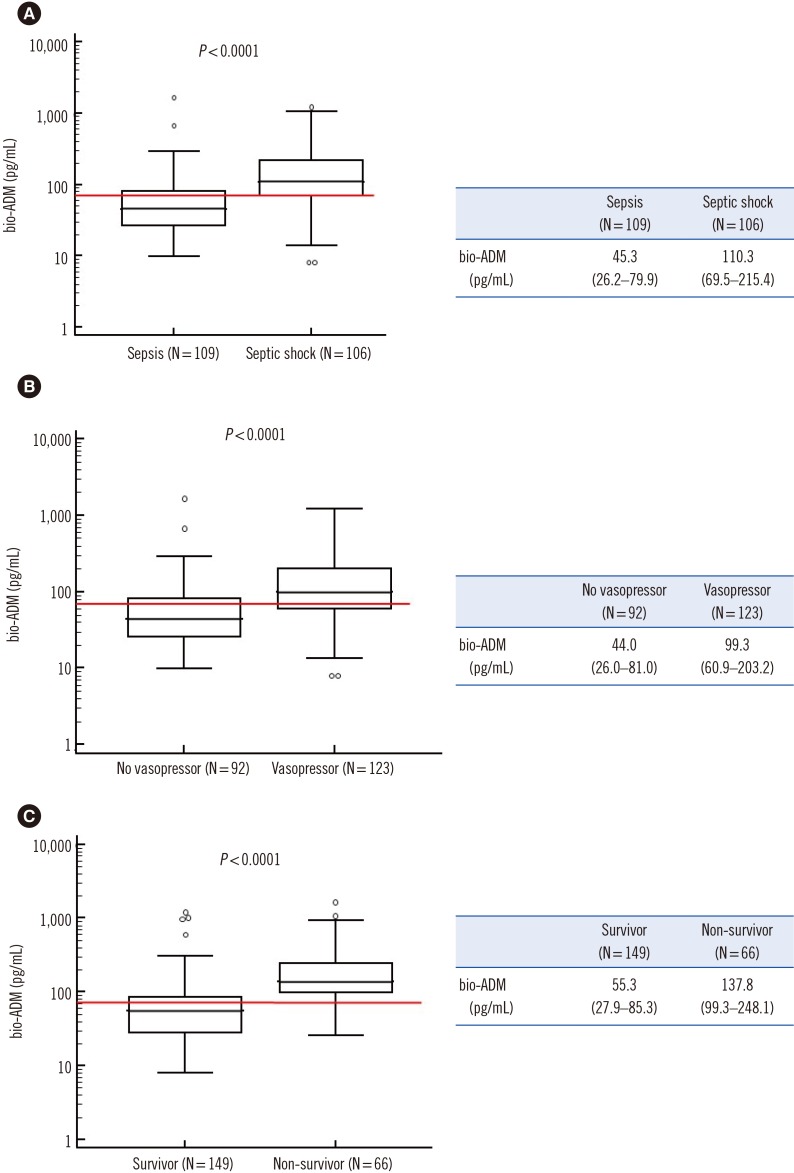
Bio-ADM concentration was significantly higher in septic shock patients than in septic patients (110.3 vs 45.3 pg/mL, P<0.0001), in patients with vasopressor use than in patients without vasopressor use (99.3 vs 44.0 pg/mL, P<0.0001), and in non-survivors than in survivors (137.8 vs 55.3 pg/mL, P<0.0001) (Fig. 1). In all three comparisons, median bio-ADM concentrations were higher than the 70 pg/mL medical decision point in patients with septic shock, vasopressor use, and in non-survivors.
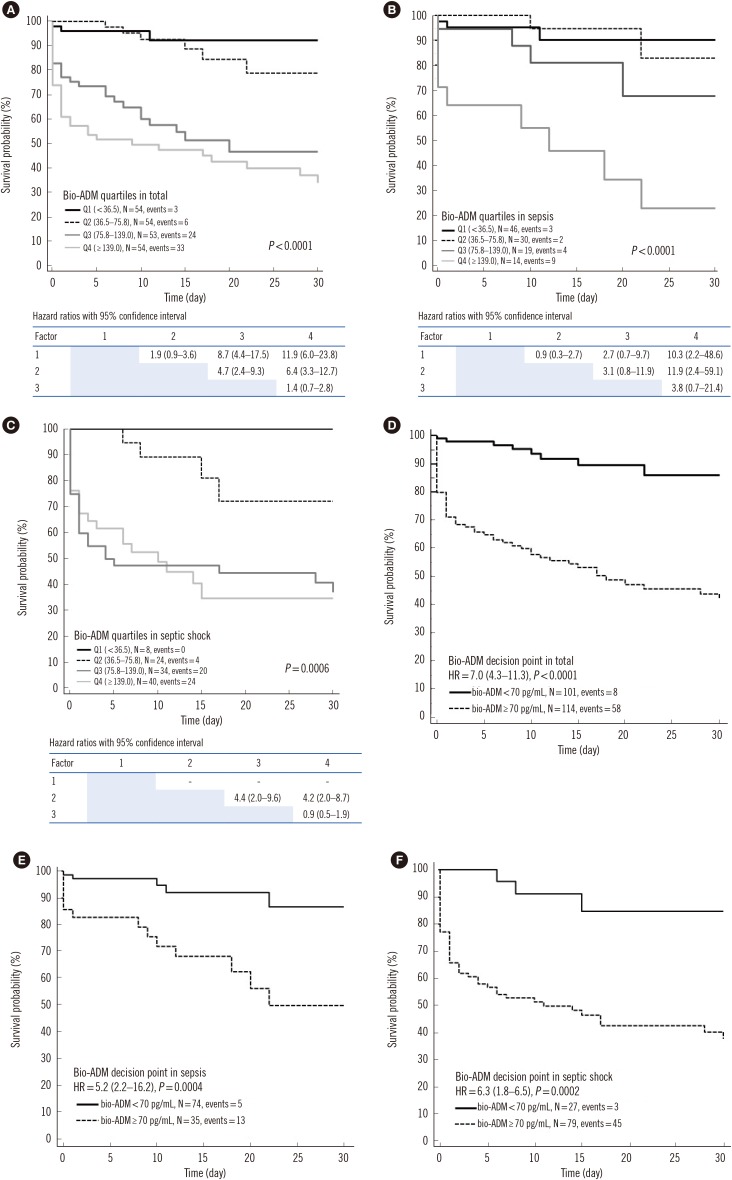
Bio-ADM concentrations were divided into quartiles: Q1<36.5 pg/mL (N=54); 36.5 pg/mL≤Q2<75.8 pg/mL (N=54); 75.8 pg/mL≤Q3<139.0 pg/mL (N=53); and Q4≥139.0 pg/mL (N=54). Bio-ADM quartiles were significantly associated with the number of organ failures (P<0.0001) (Fig. 2A) and with SOFA cardiovascular, renal, coagulation, and liver subscores, but not with SOFA respiratory and central nervous system subscores (Fig. 2B; data not shown). Bio-ADM quartiles were associated with SOFA renal subscore in patients with sepsis and with SOFA renal and coagulation subscores in patients with septic shock (data not shown).
Prediction of 30-day mortality
The 30-day mortality rate in each bio-ADM quartile group showed a stepwise increase: 5.6% in Q1, 11.1% in Q2, 45.3% in Q3, and 61.1% in Q4. In addition to all patients, significant increase was also observed in each sepsis and septic shock patient group (all P<0.0001; data not shown). Bio-ADM quartile groups could stratify the survival probability, and the HRs were significantly higher when bio-ADM Q3 and Q4 groups were compared with Q1 and Q2 groups (HR=8.7 in Q3 vs Q1; HR=4.7 in Q3 vs Q2; HR=11.9 in Q4 vs Q1; and HR=6.4 in Q4 vs Q2 group). In addition to all patients, this significant finding was also observed within the sepsis and septic shock patients (P<0.0001; P<0.0001; P=0.0006) (Fig. 3A, 3B, and 3C). When bio-ADM concentrations were stratified using the medical decision point of 70 pg/mL, the 30-day mortality rate also differed significantly between the two groups in all patients as well as within the sepsis and septic shock patient groups (HR=7.0, 5.2, and 6.3, respectively) (Fig. 3D, 3E, and 3F).
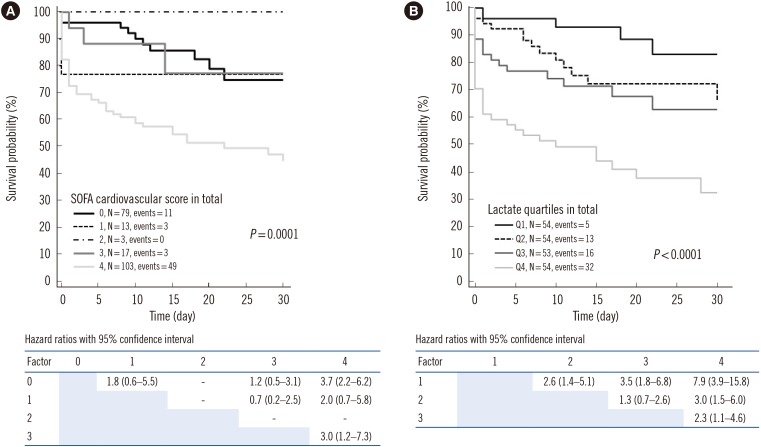
The SOFA cardiovascular subscores and lactate quartiles stratified the survival probability in all patients (P=0.0001 and P<0.0001, respectively) (Fig. 4). When patients were divided into sepsis and septic shock groups, only the lactate quartiles in patients with septic shock showed a significant stratification (data not shown). Bio-ADM concentration and SOFA score were similar in predicting 30-day mortality (AUC, 0.827 vs 0.830, P=0.918); the RR of bio-ADM concentration was higher than that of SOFA score (RR=3.6 and 1.2, respectively; Table 2).
DISCUSSION
We explored the clinical utility of bio-ADM as an objective biomarker equivalent to SOFA score for assessing organ failure and predicting mortality in septic patients. We observed that bio-ADM concentration was significantly associated with septic shock, vasopressor use, and 30-day mortality (Fig. 1). In addition, bio-ADM quartiles showed a stepwise increase in the number of organ failures, and elevated bio-ADM concentration was associated with specific organ failures, especially in terms of SOFA cardiovascular, renal, coagulation, and liver subscores (Fig. 2).
Multiple organ failure is a complex syndrome involving diverse pathways and pathological processes in sepsis [2425]. Cardiac failure is a major risk factor of in-hospital mortality [26]. In addition, cardiac and renal diseases interact in a complex bidirectional and interdependent manner in both acute and chronic settings; sepsis is a representative disease entity of the organ crosstalk between the heart and kidney [24]. Because congestion is the main cause for worsening heart failure, the 2016 European Society of Cardiology heart failure guidelines recommend daily evaluation of signs of congestion [27]. In clinical practice, however, frequent assessment of congestion is difficult, and the assessment is often considered unreliable because of considerable inter-observer variability. Therefore, there is a need for a rapid, reliable, and objective tool to assess and monitor patient's heart failure; bio-ADM is an emerging biomarker for predicting acute circulatory failure [282930]. Our data shows that bio-ADM can simply and objectively reveal sepsis-induced organ failure in circulation and has the potential to serve as a substitute for SOFA subscores.
Bio-ADM quartiles, SOFA cardiovascular subscore, and lactate quartiles all showed significant association with 30-day mortality rate. Of note, bio-ADM and lactate quartiles indicated a stepwise increase in the 30-day mortality rate; however, the SOFA cardiovascular subscore could not separate the 30-day mortality rate in a stepwise pattern (Figs. 3 and 4). This finding is in line with the original study on the SOFA scoring system [2]. More remarkably, when patients were divided into sepsis and septic shock groups, bio-ADM quartiles could consistently predict and stratify 30-day mortality. Interestingly, very high bio-ADM concentrations in sepsis without shock identified patients with a very high mortality risk (despite not having shock), whereas very low bio-ADM concentrations in septic shock identified patients with a low mortality risk. This finding may be clinically important. However, neither SOFA cardiovascular subscore nor lactate quartiles could show such a finding. The lactate quartiles were associated with 30-day mortality in patients with septic shock; given that the current definition of septic shock is based on lactate concentration, this finding was expected in this patient group. Taken together, it seems that the measurement of bio-ADM concentration could provide added value to the treatment-related SOFA cardiovascular subscore and lactate concentration in predicting 30-day mortality.
Regarding the suggested medical decision point of bio-ADM, Marino et al. [23] showed that a high 28-day mortality rate was noted for European patients who were admitted with bio-ADM concentrations >70 pg/mL. In our study on an Asian population, the clinical bio-ADM value was also useful in identifying patients with an increased mortality risk, as well as the need for vasopressor therapy; our findings support the usefulness of this bio-ADM clinical value regardless of ethnicity [161723].
Our study was limited in that it was a small-sized, single-center registry study; therefore, sepsis severity and mortality could differ from those of other population cohorts. Second, the SOFA cardiovascular subscore was based on the requirements for adrenergic support; although the enrolled patients received standardized treatment, treatment may vary across institutions or countries. Third, we could not maintain a standardized sampling time or define the exact time delay from sepsis diagnosis to plasma sampling, although it was done within 24 hours. The half-life of plasma bio-ADM is known to be approximately 20 minutes; as a biomarker of acute cardiovascular failure, bio-ADM could have significantly changed during the first 24 hours after sepsis diagnosis. In recent studies, serial measurements of bio-ADM concentrations indicated a survival benefit in patients with decreased bio-ADM concentrations at subsequent measurements [16173132]. Observation of a delta change would have further clarified the clinical significance of bio-ADM. Fourth, we did not evaluate the correlation of bio-ADM with proadrenomedullin (proADM), which has been extensively researched in sepsis and other critical settings; more bio-ADM studies (similar to the proADM studies) aimed at improving patient triage are necessary [3334].
Despite these limitations, we provide evidence that bio-ADM concentration was associated with sepsis severity, organ failures, vasopressor use, and short-term mortality in patients with sepsis and septic shock. Bio-ADM concentration and SOFA score similarly predicted 30-day mortality, with the assumption of a greater effect of bio-ADM concentration. Bio-ADM quartiles seem to be superior to SOFA cardiovascular subscore and lactate quartiles for predicting and stratifying 30-day mortality in each sepsis and septic shock patient group. Thus, bio-ADM could serve as a useful and objective biomarker that can substitute for or modify the current role of the SOFA scoring system in evaluating septic patients. Further large-scale studies are needed to support our findings.


 XML Download
XML Download