

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The incidence and mortality of prostate cancer (PCa) disease around the globe has assumed an epidemic proportion especially among men of the black race [1]. The disease was relatively rare among Nigerian men during the 1960s but has risen exponentially to the number one position of all the male cancers in Nigeria according to a recent report [2]. The World Health Organization had reported a 4.0% prevalence rate of the disease among males within the developing countries [3]. However, a prevalence rate as high as 15.7% of the disease was documented recently in a population-based study reported from the Eastern part of Nigeria [4]. There are also various reports suggestive that the PCa disease is occurring among the younger Nigerian males in contrast to previous reports [5].
The majority of the PCa disease within the black race are of the severe grade with high International Society of Urological Pathology (ISUP) grades which are usually aggressive and characterized by high metastatic and advanced stage disease potential [6]. The ISUP grading system is an objective system employed to grade PCa disease during histologic examination of prostate tissues [67]. The scores define the degree of how the cancerous tissues resemble the normal tissues which determines the disease severity. The ISUP grades are based on the Gleason grading system [67]. A higher ISUP grade suggests poorly differentiated cancer tissues which exhibit severe and advanced stage biologic behaviors [67]. Hence, the severity of PCa is characterized by its grades which determines the disease stage, whereas the stage defines the progressive potential of the disease.
Evidence suggests that environmental factors acting in concert with genetic influences could be responsible for PCa severity which usually determines the disease progression [89101112]. Low zinc status is one environmental factor that has been implicated to play a role in prostate carcinogenesis and its severe variants which define the disease progression [1112]. Zinc accumulates in the prostate ten times more than in any other human tissue where it maintains normal prostate health and inhibition of prostate carcinogenesis and progression via the reduction of energy needed for malignant transformation and the inhibition of metastatic potentials and advanced disease [1314]. Zinc accumulation in the prostate is dependent on its extracellular concentrations [14]. Therefore, plasma zinc status is suggested to be a surrogate measure of its intra-prostatic concentration [15].
Report indicates that low plasma zinc status culminates in the reduction of intra-prostatic zinc levels which promotes prostate carcinogenesis and its various adverse clinicopathologic outcomes (grade and stage) [1112]. However, most of these studies had emanated from western populations with a dearth of data in our region. Besides, very few of these studies had investigated the relationship between zinc status and PCa severity (grade) and progression (stage).
Hence, this study had been designed to examine the impact of low zinc status on the severity and progression of PCa disease using the ISUP grades and clinical staging as indices for severity and progression respectively.
Go to : 
MATERIALS AND METHODS
1. Study location
The study was conducted in the Departments of Chemical Pathology, Histopathology, and Urology of the University of Port Harcourt Teaching Hospital (UPTH). The hospital is one of the tertiary hospitals in Nigeria sited in the south-south region of Nigeria.
2. Study design
This was designed as a descriptive cross-sectional study structured to meet its primary aim and objectives which was conducted from October 2015 to June 2018.
3. Ethical consideration
Ethical approval was obtained from the University of Port Harcourt Research Ethics Committee prior to the commencement of the study (approval number: UPTH/ADM/90/S.II/VOL.X/728). Informed consent was also obtained from each participant before recruitment. The entire study procedures were in accordance with the Declaration of Helsinki of 1964 and its recent revision in 2013.
5. Study population
The study population groups consisted of 220 PCa patients recruited from the Urology clinic of the hospital and 220 age-matched apparently healthy male control participants. The apparently healthy controls are males who were certified disease-free on presentation for routine medical check-ups and screening for different disease conditions (prostatic diseases, diabetes mellitus, glaucoma, dyslipidemia) in various clinics of the hospital during the study period.
6. Eligibility criteria
The PCa patients recruited were all incident, treatmentnaïve and histologically-confirmed cases who are 50 years and above and with Gleason grade ≥6 based on the recommendations of the ISUP [6]. The apparently healthy controls included were age-matched males who are devoid of any previous or current history and clinical features of any prostatic diseases with a total prostate-specific antigen (PSA) level of less than 4 ng/mL and normal digital rectal examination findings. PCa patients and controls excluded were non-consenting potential participants, those with history of previous prostatectomy for benign prostatic hyperplasia, those with medical history of other cancers, those diagnosed with diabetes mellitus (since diabetes mellitus condition increases renal zinc excretion) and those with chronic renal diseases (since renal excretion of zinc increases in the polyuric phase of chronic renal diseases).
7. Sampling method
A simple random sampling technique was employed as a sampling method for the recruitment of the study participants.
8. Data acquisition
Middle-aged and elderly males who had presented in the Urology clinic following PCa diagnosis (via medical history interview, digital rectal examination, PSA test, and transperineal prostate biopsy confirmation) and the healthy controls were first assessed for inclusion and exclusion criteria after obtaining informed consent. Those who met the inclusion criteria were recruited following prostate biopsy by the urologist and subsequent histological confirmation by the histopathologists.
For each case selected, an age-matched (matched by ±3 years) male control was selected following medical history review, digital rectal examination and serum PSA test. Thereafter, questionnaires were administered to extract demographic variables and each participant was examined and their blood specimen was taken. Data obtained from each participant in both study groups were age (years), plasma zinc (µmol/L), fasting plasma glucose (mmol/L), plasma creatinine (µmol/L), serum total PSA (µg/L), calculated estimated glomerular filtration rate (mL/min) using the Modification of Diet in Renal Disease formula [17]. The ISUP grades were obtained from the prostate biopsy histological reports while cancer staging was done clinically at diagnosis prior to treatment using the guidelines recommended by the American Joint Committee on Cancer (AJCC) [18].
9. Specimen collection and laboratory analysis
Fasting venous blood specimen, collected from each participant every morning during the course of the study, was processed accordingly to obtain either the serum or plasma for laboratory analysis. Fasting plasma glucose was analyzed within 24 hours using the glucose oxidase method. Samples for creatinine and zinc were stored at −20℃ and analyzed within 72 hours. Plasma creatinine was determined using the Jaffe kinetic method. The total serum PSA was determined using Enzyme-linked Immunosorbent assay method. The plasma zinc was determined via the flame atomic absorption spectrophotometry using the direct method described by Smith and associates [19]. Analytical procedures were monitored for accuracy and precision with the use of three levels of commercial quality control sera. The necessary precautions were taken to prevent environmental zinc contamination of blood samples, reagents, and equipment as recommended by the International Zinc Nutrition Consultative Group (IZiNCG) [20].
10. Data stratifications and definitions
The PCa disease grades were stratified based on the ISUP grading system [6]. Using the ISUP grades, PCa disease was arbitrarily categorized as mild-moderate grade (ISUP grade 1–3) or severe grade (ISUP grade 4–5) disease [6]. The AJCC clinical staging was also arbitrarily stratified at diagnosis prior to treatment as localized (clinical stage ≤cT2) or advanced (clinical stage ≥cT3) disease [18]. Zinc status was dichotomized as low (≤11.3 µmol/L) or normal (>11.3 µmol/L) based on the IZiNCG recommendations [20].
11. Statistical analysis of data
All the data acquired were keyed into the IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA) and were subsequently reviewed, validated and properly coded. The continuous variables were initially tested for normality of distribution using the Shapiro-Wilk test. All the observed non-parametric distributed data were subsequently logarithmically transformed prior to statistical analysis. The continuous variables were presented as mean±standard deviations and compared with the independent student t-test. The categorical variables were presented in numbers/percentages and compared with the chi-square test. Pearson's correlation test was employed to examine the relationship between plasma zinc status and the ISUP grades. Binary logistic regression model was generated to determine the impact of low zinc status (plasma zinc ≤11.3 µmol/L) to predict severe grade and advanced PCa disease. Since plasma zinc status decreases with advancing age [20], age was also adjusted in the logistic regression models. An alpha value of <0.05 was chosen as being statistically significant.
Go to :
RESULTS
This study was conducted between October 2015 and June 2018 at the UPTH. The study population consisted of 220 histologic confirmed PCa patients and 220 age-matched males with no evidence of prostate diseases.
Most of the study cohorts (n=152) had low zinc status compared to those with normal zinc status (n=68) based on the definition by the IZiNCG [20].
No statistical difference was observed in the age distribution of both study groups (p=0.291) since there were age-matched. However, there were statistical difference of the fasting plasma glucose (p<0.001), plasma creatinine (p<0.001), estimated glomerular filtration rate (p<0.001), total serum PSA (p<0.001) and plasma zinc levels (cases: 9.42±3.02 µmol/L versus controls: 15.23±4.47 µmol/L; p<0.001) among both study groups (Table 1).

Table 1
Basic characteristics of prostate cancer and controls
![]()
The majority of the PCa patients presented with mild-moderate grade disease (n=137, 62.3%) while others (n=83, 37.7%) presented with severe grade disease (Table 2). Most of the patients had localized disease compared to those with advanced disease (localized: n=166, 75.5% versus advanced: n=54, 24.5%). The PCa patients with severe grade and advanced disease had significantly lower plasma zinc compared to those with the mild-moderate grade (p<0.001) and localized disease (p<0.001) respectively (Table 2).

Table 2
Distribution of plasma zinc in each ISUP grades and clinical stage stratifications
![]()
Table 3 shows strong negative correlations between plasma zinc status and the ISUP grades among the overall PCa patients (r=−0.612, p<0.001) and among those with mild-moderate grade (r=−0.586, p<0.001), localized (r=−0.622, p<0.001) and advanced disease (r=−0.558, p<0.001). However, a moderate negative correlation was documented among those with severe grade disease (r=−0.408, p<0.001) as depicted (Table 3).
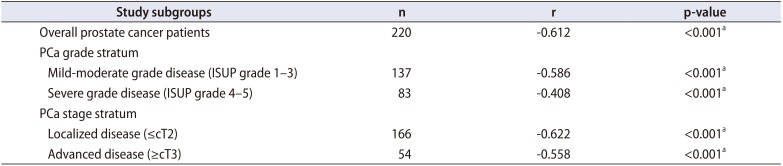
Table 3
Correlation table of plasma zinc levels and ISUP grades among various subgroups
![]()
The impact of low zinc status to predict severe grade PCa disease was about 9-fold in crude (odds ratio [OR], 8.714; 95% confidence interval [CI], 3.746–20.273; p<0.001) regression model which was amplified to more than 11-fold in the ageadjusted (OR, 11.152; 95% CI, 4.467–27.843; p<0.001) model (Table 4). While the impact of low zinc status of predicting the advanced PCa disease was more than 17-fold in crude (OR, 17.160; 95% CI, 4.041–72.871; p<0.001) and amplified also to about 19-fold in the age-adjusted (OR, 18.927; 95% CI, 4.297–83.409; p<0.001) models respectively (Table 4).
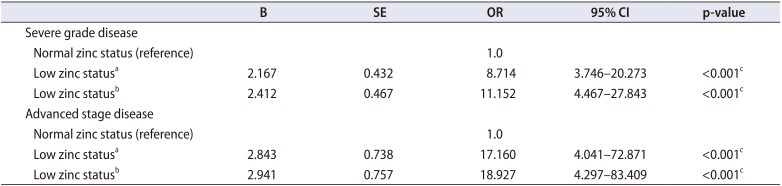
Table 4
Result of binary logistics regression analysis of the impact of low plasma zinc status of predicting severe grade (ISUP grade 4–5) and advanced (≥cT3) PCa disease
![]()
Go to :
DISCUSSION
In this study, we had evaluated the impact of plasma zinc status on the severity (grade) and progression (stage) of PCa disease. One of the most significant findings of the study was the observed significant reduction of zinc status of the overall study population with PCa disease compared with the apparently healthy age-matched controls without evidence of prostatic diseases (cases: 9.42±3.02 µmol/L versus controls: 15.23±4.47 µmol/L; p<0.001). The low zinc status was more pronounced among those with severe grade and advanced stage of the disease with inverse relationship existing between the zinc status and the disease grade among the entire PCa patients and the other study subgroups. The mean plasma levels of zinc observed among the entire PCa patients and the patients with severe grade and advanced stage disease were below the normal cut-off value defined by the IZiNCG for adult males [20]. Low zinc status also had a significant odd of predicting severe grade and advanced stage PCa disease in crude and adjusted logistic regression models. These findings are in agreement with a number of recent reports which underscore the influence of zinc on the severity and progression of PCa disease.
A recent study reported from North India by Abhishek et al. [8] had noted decreased zinc status in PCa patients relative to controls (cases: 85±10.4 µg/L versus controls: 116±19.1 µg/L; p=0.001). A previous study reported in 2014 from South-eastern Nigeria had also observed similarly reduced plasma zinc in men with PCa disease compared to apparently healthy controls (cases: 22.5±6.4 µmol/L versus controls: 25.9±9.1 µmol/L; p<0.05) [9]. The reduction of the zinc status had consistently been documented from other regions of the world among PCa patients compared to controls [212223]. However, Białkowska et al. [10] had recently reported a higher zinc status among Polish PCa patients compared to controls. While Eken et al. [11] found no difference in zinc status of Turkish PCa patients compared to controls. These reports [89] are at variance to our finding and could be related to environmental, dietary, genetic or study methodological differences. A recent meta-analysis by Gumulec et al. [22] had observed that the reduction of zinc status in PCa patients is an established fact in PCa disease. Though reports on the relationship between dietary zinc intake and PCa has produced inconsistent results due to the reliance on self-reported zinc intake, Mahmoud et al. [24] had recently reported lower zinc intake with increased PCa risk among African-Americans men.
A number of reports suggest a decreasing trend of prostatic tissue zinc status with increasing severity and progression of PCa disease [812]. Some other investigators had also evaluated the relationship between zinc status and prostate biopsy outcomes with encouraging results [25]. These reports are in accord with the findings of this present study. Cortesi et al. [12] had comprehensively evaluated this relationship and concluded that the reduction of zinc status in PCa tissues correlates with the grade of the PCa which determines the invasiveness and extension of the disease. This was recently corroborated by Abhishek and colleagues who documented a strong negative correlation between zinc status and tumor grade (r=−0.680, p=0.001) among Indian men with PCa disease [8]. Recently, the Vitamin and Lifestyle Cohort study found that long-term use of zinc supplements, although was not associated with reduced PCa risk, but was associated with reduced risk of advanced PCa disease [26].
However, a recent evaluation of the relationship between dietary zinc intake and the disease grade and stage by Gutiérrez-González et al. [27] did not support this association. Additionally, Park et al. [28] found no association between serum zinc status and PCa grade and stage.
The prostate gland has a high capacity of amassing high zinc concentrations from plasma with the aid of special transport proteins. The most important of these proteins is zinc transport protein 1 [22]. These proteins have the specialized ability to trap high amount of zinc from the extracellular plasma for the maintenance of the normal prostate gland physiology and biochemistry [14]. The intraprostatic concentrations of zinc in the prostate gland also depends on the available quantities of plasma zinc concentrations [1415]. The prostate zinc concentration has been reported with overwhelming evidence of inhibiting the promotion of carcinogenesis while enhancing various anti-cancer activities in the prostate gland. The reduction of zinc mineral in the prostate plasma and prostate tissue has been adjudged the most cardinal initiating event in prostate carcinogenesis [13]. Hence, the reduction of zinc status that occurs in these patients eliminates all the anticancer effects of zinc in the gland, enabling the malignant transformation of prostate cells, facilitating the malignant cells to meet the metabolic and bioenergetics of malignancy, enhancing their growth and progression to invade tissues and metastasize in the process [12131415].
The strength of this study lies in its prospective design and the recruitment of only the histologically-diagnosed PCa disease. However, there are some limitations that are worth mentioning. First, it was a hospital-based study conducted in a single center. Therefore, its findings might not be representative of the entire population in the region. Secondly, the Gleason grades were reported by different histopathologist, which is subject to inter- and intraindividual variations. Thirdly, prostate biopsy was not carried out on the controls due to ethical issues, so we cannot rule out with certainty that some of the controls did not harbor subclinical PCa. However, the controls were all healthy and ambulatory men with no medical history, clinical, and laboratory features of prostatic diseases. Finally, although plasma zinc is an accepted biomarker for zinc status owing to its response to zinc intakes and prediction of functional response to zinc supplementation, its plasma levels may not correlate well with zinc levels in prostate tissues [2223].
Go to :
CONCLUSIONS
The findings from this study support the epidemiologic evidence that zinc status is significantly reduced in patients with PCa compared to controls. The reduction was more pronounced among those with the severe grade and advanced stage PCa disease. Zinc status was found to be inversely associated with disease grades which tend to define the disease stage. This suggests that low zinc status influences the severity and progression of PCa disease. However, further elaborate and well-designed studies with large sample size are warranted to confirm these associations.
Go to :
 XML Download
XML Download