

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Transrectal ultrasound (TRUS)-guided systematic biopsies of the prostate do not pick up all prostate cancer and many lesions may be missed [1234]. Multiparametric magnetic resonance imaging (mpMRI) is among the most common imaging modalities used to aid detection of prostate cancer [34]. mpMRI involves one anatomical sequence (T2-weighted) with at least one functional sequence such as diffusion-weighted imaging (DWI), dynamic contrast enhancement (DCE), or spectroscopy (MRS) and is also used in the current standard Prostate Imaging-Reporting and Data System (PI-RADS) classification for prostate lesions [5]. Lesions seen on mpMRI correlate with actual tumor location on radical prostatectomy specimens, and the level of suspicion on imaging correlates with the D'Amico stratification [67].
Lesions identified on mpMRI can be targeted for biopsy either within the MRI machine (in-bore) or during a TRUS biopsy using either cognitive localization or devices that ‘fuse’ MRI images with real-time ultrasound. Cognitive biopsy relies on operator expertise, whereas inbore biopsy is expensive, time-consuming, and uncomfortable for the patient, and has limited availability. While MRI-TRUS fusion biopsies offer an opportunity to harness the advantage of mpMRI data, their value in routine clinical practice is not standard [8]. Asian populations have a lower incidence of prostate cancer than reported in Western nations [9]. Since the sensitivity of a test can vary according to the prevalence of disease, it is possible that the performance of fusion biopsies would differ in these populations [10].
We previously reported our experience with cognitive fusion biopsies using MRS data and found that targeting improves detection in our population where the biopsy positivity rate is otherwise low [1112]. Since cognitive fusion and MRS are difficult techniques to perform, we assessed the role of an MRI-TRUS fusion device in increasing the yield of biopsies in patients with serum prostate-specific antigen (PSA) values between 4 and 20 ng/mL and those with prior negative results on standard 12-core TRUS biopsies.
Go to : 
MATERIALS AND METHODS
1. Setting
This prospective study was performed at a single tertiary referral center in a country (India) with a low incidence of prostate cancer over an 18-month period beginning in August 2015. The study was approved by the Institutional Ethics Committee, All India Institute of Medical Sciences, Ansari Nagar, New Delhi (approval number: IECPG-526) and conformed to the provisions of the Declaration of Helsinki, and all subjects provided written informed consent.
2. Patients
All patients with clinical indications for prostate biopsy (total PSA between 4 and 20 ng/mL or an abnormal result on a digital rectal examination [DRE] suspicious for prostate cancer) were screened for inclusion. Patients in whom MRI was contraindicated or not feasible, those who refused to participate in the study, and those with diffuse hard nodular prostates were excluded. Patients in whom no abnormalities were found by MRI were also excluded from the study.
3. Procedural details
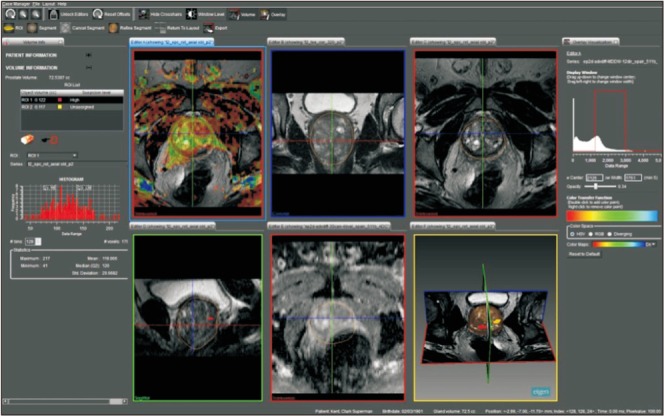
All patients underwent mpMRI of the prostate (Philips Ingenia 3T Machine; Philips, Amsterdam, The Netherlands) before the biopsy. All MRI results were reported by a single radiologist using the PI-RADS classification (version II) [5]. Identifiable abnormal lesions were marked on mpMRI using the PROFUSE software (Eigen, Grass Valley, CA, USA) (Fig. 1) and targeted for biopsy on the Artemis MRI-TRUS fusion device (Eigen). A standard systematic 12-core biopsy (base, mid-gland, and apex; lateral and paramedian; both lobes) preceded targeted biopsies from mpMRI-identified lesions. At least one and preferably two cores were taken from each of the targeted lesions. All biopsies were individually labeled and processed.
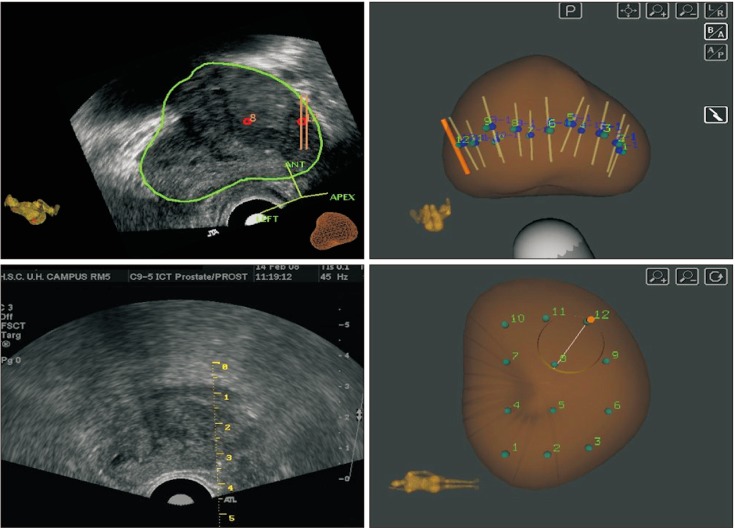
All patients received a preprocedural prophylactic antibiotic and enema. All biopsies were performed on an outpatient basis with infiltrative local anaesthesia on either side at the base of prostate. The whole gland was scanned over 360 degrees, after which the image was registered and then segmented and refined in both transverse and sagittal dimensions by the software. The refined image was then fused to the premarked mpMRI images that had already been uploaded on the device. For each core sampled, the needle track was automatically saved by the software. At the end of the procedure, a PDF file was generated for each patient showing the three-dimensional track of the sampled cores (Fig. 2). Complications were noted before discharge, during follow-up if the patient self-reported, and with direct enquiry at the next visit.
4. Interpretation
The rate of cancer detection was compared between systematic and targeted biopsies. Additionally, change in Gleason scoring and change from nonsignificant to significant cancer was compared on the basis of each of the two biopsy modalities. Cancers with a Gleason's score (GS) of 3+3 or 3+4 were considered clinically insignificant cancers, whereas those with GS 4+3 or higher were considered clinically significant [1314]. Additional analyses were performed for patients who had a prior negative biopsy result.
5. Statistical analysis
The data were analyzed by using STATA statistical software (version 14.0). Quantitative data were expressed as mean, standard deviation, and median (minimum-maximum) as appropriate. Qualitative data were expressed as frequency and percentage. Fisher's exact test was used to check the association between the variables. Student's t-test and Mann Whitney U test were used to compare normal and skewed variables, respectively. The p-values ≤0.05 were considered as statistically significant.
Go to :
RESULTS
During the study period, 210 patients were screened, of whom 131 were included in the study. Their mean age was 63.5 years and their mean serum PSA value was 9.75±5.35 ng/mL. Mean prostate volume was 54.2±30.9 cm3. A total of 30 patients (22.9%) had a suspicious nodule on a DRE.
The PI-RADS score on mpMRI ranged from 2 to 5 with a median of 3. A median of 14 cores (range, 13–20 cores) were biopsied in each patient, of which the median number of targeted cores was 2 (range, 1–8 cores) (Table 1). Malignancy on biopsy was detected in 36 patients (27.5%). In three patients, cancer was detected exclusively on systematic biopsy, whereas in another three cancer was detected exclusively in targeted cores. The detection rate with each modality was thus 91.7% (33/36). Thirty of the cancers were significant (83.3%). Of these, 21 (70.0%) were picked up by systematic biopsies and the targeted biopsies picked up 28 (93.3%) (Table 1).

Table 1
Outcomes of biopsy
![]()
Among the 30 patients who had cancer detected on both systematic and targeted biopsies, 8 (26.7%) had discordant a GS between systematic and targeted biopsies and were upgraded on targeted cores (Table 2). Of these, 6 were upgraded from clinically insignificant to significant cancer.

Among patients with a prior negative biopsy result (n=17), five (29.4%) were detected to have cancer on fusion biopsy. Of these, three had cancer detected only on systematic cores, and none had cancer detected exclusively on targeted cores, whereas the other two had one core each of systematic and targeted biopsies positive. Two of these five had clinically significant cancers.
Eight patients (6.1%) developed a complication, of whom five had post-biopsy fever requiring admission and parenteral antibiotics, one had hematuria, and two had urine retention.
Go to :
DISCUSSION
In our cohort of males with historically low rates of detection of prostate cancer, mpMRI-TRUS fusion biopsies detected malignancy in 27.5% of males. A total of 83.3% of these cancers were clinically significant, and targeted biopsies identified 93.3% of these significant cancers. However, targeted biopsies alone would have missed 3 of 36 cancers, including 2 of 30 significant cancers.
The use of mpMRI targeting for prostate biopsies may serve two purposes. Apart from identifying potential targets for biopsy based on MR data, use of mpMRI may help to improve yield even from systematic cores by ensuring a more even sampling of the gland than TRUS guidance alone. Standard systematic biopsies have a low sensitivity and tend to detect more indolent cancers [15]. While there is increasing data on the use of fusion techniques, nearly all of this comes from populations with relatively high prevalences of prostate cancer [131617181920]. Some of these studies have reported cancer detection rates, with fusion techniques, as high as 89% [16]. The prevalence of cancer in India and other Asian countries is much lower, at times less than 5.6% of the rates in other populations (7/100,000 versus 126/100,000) [92122]. Disease prevalence affects the performance of a diagnostic test and may cause a change in its sensitivity or specificity of up to 40% [10]. Cancer detection rates among our population of men tend be low, with reported detection rates of 13% for men with PSA below 20 ng/mL [21]. Our own data from a similar population of patients found a low 10.1% cancer detection rate on standard TRUS-guided biopsies, although one of the confounders in that cohort may have been the lower average PSA [11]. The current study found a higher yield not only on targeted cores but also on the systematic cores. This would suggest a role of fusion techniques in increasing the yield even on systematic biopsies. Similar data have previously been reported using fusion techniques in these populations which otherwise have a low incidence of prostate cancer [23]. Such variations make it important that data on performance of investigations be assessed in different populations, because direct translation of information from one study may not be possible.
The PI-RADS classification has simplified mpMRI reporting and allows uniformity for comparisons [24]. Similar to previously reported data, our findings showed that a greater proportion of positive biopsies corresponded to higher PI-RADS scores [16]. However, cancer was found even on lesions reported as PI-RADS-2, which suggests that when a fusion biopsy is planned, PI-RADS-2 lesions should also be targeted.
mpMRI-based targeted biopsies have been reported to result in higher cancer detection rates along with detection of more clinically significant cancers [171825]. We found that targeted cores detected a high 93.3% of all significant cancers in our cohort. However, targeted biopsies failed to detect three cancers, including two significant ones, suggesting that the systematic cores should not be omitted from the biopsy protocol. On the contrary, performing systematic biopsies alone would not only have missed three cancers altogether (all significant cancers), but would have understaged six additional cases. Overall, 9 of 30 significant cancers (30.0%) would have been missed by systematic biopsies alone. Similar studies have shown upgrading rates of 32% to 35% [13]. Our data are consistent with the findings of the prospective PROFUS trial that evaluated targeted biopsies [19]. That study reported a cancer detection rate of 32% with the primary benefit of fusion being the detection of higher grade cancers.
Our study was limited by the lack of a control arm including patients who did not undergo nonfusion biopsies. However, our previously reported data [1112], and that of other reports from this region [2123], suggest that the cancer detection rate of systematic TRUS biopsies is low in our patients. Our current results can thus be compared to such controls. We were also limited by the lack of radical prostatectomy step-section histology results for comparison. However, since the primary objective was to evaluate the rate of cancer detection on biopsy, the objective was fulfilled.
Go to :
CONCLUSIONS
mpMRI-TRUS fusion targeted biopsies improved the detection of clinically significant cancers in comparison with systematic TRUS-guided biopsies. However, targeted biopsies alone would have missed 8.3% of cancers, including 6.7% of significant cancers. The use of fusion techniques increased the overall cancer detection rate in comparison with historical systematic TRUS biopsies in our population with a low incidence of prostate cancer, which suggests a potential role for this technique.
Go to :
 XML Download
XML Download