

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Subjective cognitive decline (SCD) is a clinical diagnosis when subjects complain of consistent cognitive decline without any objective cognitive impairment in detailed neuropsychological tests.123 It is known to be a risk factor for the progression of Alzheimer's disease (AD) and is purported to be the first symptomatic stage of the AD continuum disorders.245 SCD is also depicted to be a heterogeneous condition including the later stages of preclinical AD, other neurological disorders, systemic medical conditions, personality disorders, and psychiatric diseases. Thus, it is clinically important to use sensitive clinical markers in the categorization of subjective complaints and prediction of AD-related pathologies. Previous studies have explored relevant clinical factors associated with Alzheimer's pathologic changes.6789 However, clinical features of the subjective complaints that are sensitive in the detection of AD pathology have not yet been identified. In 2014, an international work group, SCD Initiative, proposed specific features that may predict AD.2 Nonetheless, investigations on whether the proposed features can discriminate AD and non-AD in SCD have not been fully explored in real practice. We hypothesized some features among the expert suggestions would be useful to detect preclinical AD. We examined neuroimaging biomarker distributions of SCD and explored the relevance between the self-report questionnaire and Alzheimer's pathologic changes.
METHODS
Participants
This study was performed at a university-affiliated dementia clinic from December 2016 to August 2017. The elderly subjects who had visited the hospital for evaluations of dementia and were diagnosed with SCD after routine work-ups, including detailed neuropsychological tests and brain magnetic resonance imaging (MRI), were consecutively recruited during the study period. To be eligible for the current prospective study, subjects had to meet the following criteria: 1) existence of consistent self-reported cognitive complaints; 2) older than 50 years old; 3) normal performance (above −1.0 standard deviation of norms) on all subtests of detailed neuropsychological tests; 4) clinical dementia rating (CDR)10 score of 0; 5) literate; and 6) who agreed to participate in the study and could visit the hospital for evaluations. Subjects were excluded from the study if they had following conditions: 1) uncontrolled medical conditions which can cause cognitive impairment; 2) neurologic disorders such as Parkinson's disease, Huntington's disease, or normal pressure hydrocephalus; 3) major psychiatric disorders such as uncontrolled depression, schizophrenia, alcoholism, or drug dependency; 4) mild cognitive impairment (MCI) or dementia; 5) abnormal lab findings such as abnormal thyroid function, low vitamin B12 or low folate, or positive syphilis serology; and 6) brain lesions known to cause cognitive impairment (tumor, stroke, or subdural hematoma). Additionally, all participants underwent physical examinations, neurologic examinations, apolipoprotein ε genotyping, the self-report questionnaire for SCD, and florbetaben positron emission tomography (PET) scans. Previous brain MRI results (within 6 months), florbetaben PET findings (within 6 months), apolipoprotein ε genotype, neuropsychological tests (within 3 months), and blood lab findings (within 3 months) were permitted. This study was approved by the Institutional Review Board (#DAUHIRB-16-232) and written informed consent was obtained from all participants.
Self-report questionnaire for SCD
The newly developed questionnaire consisted of 2 parts; 10 questions to characterize complaints recommended by experts2 and a Korean version of cognitive failure questionnaire (CFQ) by Broadbent et al.11 The first section was composed of 10 questions associated with an increased likelihood of preclinical AD in individuals with SCD. Some of the questions incorporated in the ‘SCD-plus features' include: 1) Do you have memory decline? (yes/no); 2) Do you have any non-memory domain decline? (yes/no); 3) If a non-memory domain has declined, please specify; 4) Which domain declined first? 5) Age at onset of the decline; 6) Relative scoring compared with the past (range, 1–5; 5 is the best); 7) Feeling of worse performance than others of the same age group (yes/no); 8) Relative scoring compared with others of the same age group (range, 1–5; 5 is the best); 9) Concerns (worries) about SCD (yes/no); and 10) Confirmation of cognitive decline by an informant (yes/no). We have translated the 10 key questions that should be coded in SCD studies to identify features relevant to Alzheimer's pathologic changes. The second component, the CFQ, is the 25-item questionnaire developed for the evaluation of self-reported failures in perception and memory functions. Its score ranges from 0 to 100, and higher score indicating higher levels of self-cognitive complaints.11 The questionnaire was self-administered at the outpatient clinic.
Neuroimaging
Brain MRI was performed using a 3.0-tesla scanner (GE Medical Systems, Milwaukee, WI, USA), including fluid attenuated inversion recovery (FLAIR), gradient-echo, and 3-demensional (3D)-T1 weighted images. The 3D-T1 weighted MRIs were performed in the sagittal plane with a slice thickness of 1.0 mm. The white matter hyperintensities (WMH) were rated using a visual rating scale of axial FLAIR images, in brief, periventricular WMH and deep WMH were separately evaluated and rated as minimal (grade 1), moderate (grade 2), or severe (grade 3).12 Lacunes of presumed vascular origin were defined as small lesions (3–15 mm in diameter), hyperintense on T2- and hypointense on T1-weighted images, with a perilesional halo on FLAIR. Cerebral cortical microbleeds were defined to be round-shaped and homogeneously-low signal lesions with less than 10 mm-diameters in lobar areas on gradient echo images. Hippocampal atrophy was rated on coronal T1-weighted images using Scheltens visual rating scale.13 The mean of the left and right hippocampal atrophy scores was used. The number of lacunes of presumed vascular origin, number of cortical microbleeds, and hippocampal atrophy were assessed by a blinded neurologist.
18F-florbetaben PET scans were acquired in accordance with the standardized protocol.14 A whole brain visual assessment was performed by a trained specialist in nuclear medicine who was blinded to the clinical diagnosis using regional uptake ratings (1, no tracer uptake; 2, moderate tracer uptake; and 3, pronounced tracer uptake) in 4 brain areas and a global scoring system named brain amyloid plaque load (BAPL) adapted from previously described techniques.15 The PET scans were rated as positive amyloidosis with a BAPL score of 2 or 3. Additionally, quantitative neuroimaging analysis using the PET scans was performed to assess the amyloid burden and distributions. Regional amyloid depositions were measured using MATLAB version 2013a and SPM8 (http://www.fil.ion.ucl.ac.uk/spm/software/spm8). Individual T1-weighted MRI scans were estimated and co-registered into corresponding PET images. Each individual MR image was normalized to a standardized stereotaxic space and was divided into 3 probabilistic tissue maps such as gray matter, white matter, and cerebral spinal fluid. A volume-based template, incorporating 90 regions-of-interest, was aligned to individual T1-weighted MRI. The voxels of florbetaben PET images were scaled using the mean uptake value in the cerebellar cortex to calculate the standardized uptake value ratio (SUVR).
Neuropsychological tests
All participants were diagnosed as SCD using a formal neuropsychological test battery, named the Seoul Neuropsychological Screening Battery (SNSB).16 It includes the Korean version of the Mini-Mental State Examination,17 CDR, activities of daily living, attention (Digit Span Test), language (Boston Naming Test, tests for comprehension/repetition/fluency), visuospatial function (Rey Complex Figure Test [RCFT]), verbal and visual memory function (Verbal Learning Test and RCFT recall test), and frontal executive function (contrasting program, go/no-go, Controlled Oral Word Association Test, and Stroop Test).16 These tests were administered by trained neuropsychologists. Age-, sex-, and education-specific norms based on normal controls were used to interpret the SNSB results. Scores of <16th percentile, which were compared to −1 standard deviation of the norm, were defined as abnormal.
Preclinical AD staging
All the participants were divided into 4 groups based on National Institute on Aging and Alzheimer's Association preclinical AD grades.418 We had 2 sources of data, the florbetaben PET for amyloid depositions and brain MRIs for neurodegenerative changes, to categorize the participants. Since the cut-off points used in the definition of normal or abnormal amyloidosis and neurodegenerations in this population were not confirmed, we used the visual rating scales, BAPL scale and Scheltens scale, for the staging. First, positive findings for amyloidosis (Aβ+) indicate BAPL scores of 2 or 3. Second, positive findings for neurodegenerative changes (N+) indicate mean hippocampal atrophy scores of 1.5 or higher.19 SCD participants with Aβ−N− were grouped as ‘stage 0,’ Aβ+N− as ‘stage 1,’ Aβ+N+ as ‘stage 2,’ and Aβ−N+ as ‘suspected non-AD pathophysiology (SNAP).’
Statistical analysis
Independent t-test or nonparametric Mann-Whitney U-test were used in the comparison of continuous variables such as baseline demographics and clinical characteristics and amyloid-positive and amyloid-negative SCD groups according to normal distribution patterns. The χ2 tests were used to compare categorical variables between the 2 groups. All statistical analyses were performed using SPSS (version 18.0; SPSS Inc., Chicago, IL, USA). The p-values below 0.05 were considered to denote significant differences.
RESULTS
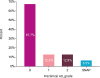
We consecutively recruited 52 subjects who were clinically diagnosed with SCD and finally 31 participants completed the study evaluations (Fig. 1). Among the 31 participants, 8 (25.8%) showed increased amyloid depositions using visual ratings for florbetaben PET scans. The distribution of preclinical AD stages in the participants are shown in Fig. 2. Twenty-one participants (67.7%) were in stage 0 (Aβ−N−), 4 (12.9%) were in stage 1 (Aβ+N−), 4 (12.9%) were in stage 2 (Aβ+N+), and 2 (6.5%) were in SNAP (Aβ−N+).
 | Fig. 1Flowchart of the participants.SCD: subjective cognitive decline, MRI: magnetic resonance imaging, PET: positron emission tomography, N: neurodegeneration; 3D: 3-demensional.
|
The basic demographics and clinical characteristics were not significantly different between the amyloid-positive and negative group except for global SUVR, severities of periventricular WMH, and hippocampal atrophy (Table 1). The mean global SUVR values were 1.169±0.052 in amyloid-negative SCDs and 1.461±0.207 in amyloid-positive SCDs (Table 1). Periventricular WMH and hippocampal atrophy were more severe in the amyloid-positive group compared to those in the amyloid-negative group. Moreover, the amyloid positive group tended to be older compared to the amyloid-negative group, although they did not reach statistical significance (Table 1). The results of the neuropsychological test battery did not differ between the 2 groups (p>0.05).
Table 1
Demographic data and clinical characteristics
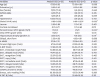
Data are shown as mean±standard deviation or number (%).
SCD: subjective cognitive decline, APOE4: apolipoprotein ε4, DM: diabetes mellitus, SUVR: standardized uptake value ratio, WMH: white matter hyperintensities, GDepS: geriatric depression scale, K-MMSE: Korean version of the Mini-Mental State Examination, K-BNT: Korean version of Boston Naming Test, RCFT: Rey Complex Figure Test, SVLT: Seoul Verbal Learning Test, COWAT: Controlled Oral Word Association Test, K-TMT-B: Korean version of Trail Making Test-B.
*Significant difference between the groups (p<0.05).
![]()
Table 2 shows results of the self-report questionnaire of SCD between amyloid-positive and negative groups. Some of the questions on “symptom onset after 65 years-of age” and “informant's awareness of the decline” showed numerical differences in the incidences but they did not reach a statistical significance (Table 2). By categorization of SCD into 4 preclinical AD grades according to the neuroimaging biomarker findings, participants who reported ‘informant reporting a decline,’ ‘feeling of worse performance than others,’ and ‘age of symptom onset after 65 years old’ showed numerically different distributions of preclinical AD grades, although they did not reach a statistical significance (p>0.05, Fig. 3). In terms of amyloidosis (stage 1 or stage 2), participants with ‘informant reporting a decline’ or ‘age of symptom onset after 65 years old’ showed numerically higher incidences of stage 1 and 2, which indicates more Alzheimer's pathologic changes (Fig. 3).
Table 2
Results of the self-report questionnaire
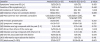
Data are shown as mean±standard deviation or number (%).
SCD: subjective cognitive decline, CFQ: cognitive failure questionnaire, NA: not applicable.
![]()
 | Fig. 3Preclinical AD grades based on self-report questionnaire (A) Informant's report about the decline (B) Worse than others of the same age group (C) Symptom's onset age over 65 years old. ‘1’ indicates ‘yes’ and ‘0’ indicates ‘no’ for the question.AD: Alzheimer's disease, SNAP: suspected non-AD pathophysiology.
|
DISCUSSIONS
In this study, we examined the biomarker distribution in SCD participants and investigated whether specific clinical features using a self-administered questionnaire differed according to Alzheimer's pathologic changes. The categorization of complaints using a self-administered questionnaire is critical in the following aspects. First, subjects with SCD still maintain normal cognition by repetitive compensations for the rapid cognitive decline. Hence, the subjective complaints are the only clinical symptom that can be assessed. Moreover, the subjects in this population can explain and report their symptoms in detail because they retain normal cognitive functions. Second, numerous studies are investigating the reliability of screening tools in SCD used in the detection of AD-related pathologies. This is because, it is an upcoming risk factor for AD and a target population for secondary preventive therapy. Third, in vivo detection of amyloidosis with amyloid PET in all subjects with SCD are not currently available due to high costs, reluctance of the subjects, and ethical considerations. Hence, the categorization of SCD into high-risk group that requires further biomarker evaluation; additionally, the identification of low-risk groups who do not require further work-up would also be clinically important.
Our results showed 3 major findings. First, 25.8% of SCD participants had increased amyloid deposition, which was slightly higher than the one existing in previous studies for the elderly with normal cognition irrespective of subjective cognitive complaints.2021 This could be expected because subjective cognitive complaint is known to be associated with elevated amyloid depositions. Thus, the subjects with SCD showed more AD pathologies in comparison to the general populations.921 Second, amyloid-positive SCDs showed more severe periventricular white matter and neurodegenerative changes represented by hippocampal atrophy. Hippocampal atrophy is a well-known neuroimaging risk factor of AD. Although the association between cerebrovascular markers and amyloidosis in non-demented elderly is controversial, recent studies reported significant relationship of WMH to AD pathologies, which can be explained by 1) common risk factors such as hypertension, diabetes, obesity, and smoking; 2) cerebral amyloid angiopathy causing vascular amyloidosis; and 3) potential other mechanisms by which cerebrovascular changes directly accelerate amyloid depositions.22 Third, participants who reported the ‘informant reporting a decline’ or ‘symptom onset after 65 years old’ showed different distributions of preclinical AD grades and numerically higher incidences of Alzheimer's pathologic changes, although none of the self-administered questionnaires showed statistically significant differences between amyloid-positive and amyloid-negative groups. Our results are in accordance with the previous studies that investigated the relevance of ‘informant reports’ for detecting the subtle AD-related cognitive decline.232425262728 They found that informant's reports were significantly associated with AD biomarkers, risk factors of progression to AD, and enabled discrimination of preclinical AD.2324252627 Informants' reports are thought to contribute to the discrimination of AD by providing a longitudinal, objective overview of cognitive decline in this ‘subjective’ complainers. The ‘symptom onset after 65 years old’ indicates that, the cognitive decline was developed recently; considering that amyloid depositions increase with aging and there is evidence that the onset of cognitive decline within a few years is more predictive of AD than the lifelong cognitive complaints, and onset age of symptom is one of the important questions.2
Several explanations may have been put forth to explain the failure to reach significant differences. For example, it may be due to under-power related with the small sample size, insufficient discriminatory power of a single question to detect Alzheimer's pathologic changes, or innate clinic-pathologic dissociations between clinical symptoms and amyloidosis in this population. Despite the low statistical power, the numerical difference in the distributions of biomarker findings between the ‘yes’ and ‘no’ group in specific questions should be re-assessed in future longitudinal studies.
Another interesting issue is whether the degree of subjective complaints or objective cognitive scores is associated with AD pathologies. In our study, the total CFQ scores did not differ between amyloid-positive and negative groups. This is consistent with the previous studies reporting that amounts of subjective complaints were not associated with cognitive performance or Alzheimer's pathologies but were strongly related to psychological and personality measures.23 The neuropsychological tests scores were not different from the amyloid-positive and negative groups in our study. It is possible that standard neuropsychological tests are not sensitive enough to detect the subtle cognitive changes in preclinical AD because they were originally developed to detect cognitive impairment in later stages.
Our study has several limitations. First, the sample size is relatively small to indicate any statistical power. Thus, it may limit the generalizability of our findings. However, this study would be meaningful since it is a prospective study that aims to adapt the new questionnaire and assess the feasibility of the questionnaire. Moreover, considering that SCD subjects maintain normal function and do not require regular medical assistance, participant recruitment in a single center was difficult. Second, the cross-sectional data required longitudinal evaluation of the progression to MCI/dementia. Third, extensive biomarker evaluations including work-ups for the tau depositions or quantitative measuring of neurodegenerations are lacking. In future studies, reliable cut-off points should be applied for appropriate categorization of biomarker evaluation into normal or abnormal findings. Nevertheless, our study has strengths, in that, we adapted a self-administered questionnaire as the first step for predicting AD, based on extensive neuropsychological tests, neuroimaging biomarker findings for amyloidosis and neurodegeneration, and detailed assessment of cognitive complaints.
In conclusion, amyloid-positive SCDs were different from amyloid-negative SCDs in relation to neuroimaging biomarkers such as WMH and hippocampal neurodegenerative changes. In the self-reported questionnaire, participants with the ‘informant reporting a decline’ or ‘older age of onset’ presented more incidences of preclinical AD, compared to those without these features. A few self-reported clinical features about the cognitive decline might give important clues in the prediction of Alzheimer's pathologic changes in subjects with SCD, which is worth reassessment in future studies.
 XML Download
XML Download