

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Vertebral compression fractures (VCFs) is a main public health issue in the elderly population1112) and osteoporosis is one of the most common causes of VCF.13) Many patients with osteoporotic VCFs (OVCF) are managed by conservative treatment such as pain medication, bed rest, and external orthosis apply,41925) but, pain does not improve even with aggressive conservative pain management and progression of vertebral body collapse are considerable problems in conservative treatment.26) Since surgical interventions such as vertebroplasty and kyphoplasty can lead to rapid pain relief, enable early ambulation, and improve the quality of life for most patients, some clinicians favor surgical intervention rather than conservative treatment.127913192829) However, surgical treatment also has risks of infection, cement leakage, and nonhealing between interface of bone/cement and new adjacent VCF.32) Therefore, treatment of OVCF is still controversial.26)
Teriparatide, a recombinant human parathyroid hormone (PTH), is the first anabolic agent of osteoporosis.26) Its effects on cultivating bone mineral density (BMD) and diminishing fracture risk have been reviewed extensively in the literature to directly stimulate bone formation for increasing bone strength and quality.510171821232635) Nowadays, it is assumed that teriparatide can potentially enhance fracture healing and treat OVCF. However, there is little evidence that teriparatide may enhance OVCF healing.32) US Food and Drug Administration (FDA) and European Medicines Agency only approved teriparatide for the treatment of osteoporosis and recommended that it should not be used for more than 2 years because of osteosarcoma risk. Therefore, usage of teriparatide for fracture healing is still off-label. Although Park et al.26) and Wu et al.34) have reported that using teriparatide for 3 months is effective for fracture healing, the period of teriparatide administration for fracture healing varies depending on studies without a consensus. Teriparatide should be used for up to 24 months for maximum efficacy, but compared to conventional drugs such as bisphosphonate, teriparatide is expensive and had a problem with patient compliance during long-term use. Since teriparatide increase lumbar spine BMD significant at 3 months (FDA), we started the study assuming a minimum period of 3 months to see the therapeutic effect of teriparatide. Thus, the aim of this study was to elucidate the effectiveness of using teriparatide for 3 months on patients with OVCF at thoracolumbar spine via pain and radiological preference.
MATERIALS AND METHODS
Study design and patients
Twenty-five patients with thoracolumbar osteoporotic compression fractures between July 2012 and October 2016 who could be followed up for more than 1 year were reviewed. The inclusion criteria were as follows: 1) only 1 level osteoporotic fracture with 5% to 20% canal encroachment; and 2) BMD of less than −2.5. Exclusion criteria were: neurological deficits exist, pathological fractures, unstable vertebral fractures involving the middle or posterior column of the spine, and those who underwent spinal surgery such as vertebroplasty. Patients were divided into 2 groups depending on whether teriparatide was used. Fourteen patients received teriparatide by subcutaneous injection (group I) and 11 patients did not receive teriparatide (group II). Patients in group II received other osteoporosis drugs such as selective estrogen receptor modulator (SERM), bisphosphonate, calcium, or vitamin D supplement, according to personal circumstances. Patients in group I were given SERM or bisphosphonate after 3 months teriparatide injection. It would have been better if we divide group 1 and group 2 to subgroup depending on usage of SERM, bisphosphonate, vitamin D and calcium supplement. However, the total number was small and could not be divided into subgroup. All patients in both groups had bed rest for at least 2 weeks. Some patients with consistent pain had bed rest up to 3 weeks. All patients underwent postural reduction using a soft pillow under the compressed level for a few days. After that, patients began to ambulation with thoracolumbosacral orthosis. Pain medication was optimized according to individual needs of patients. All patients started with nonsteroidal anti-inflammatory drug. Depending on their symptoms, medications such as acetaminophen, opiate derivatives, and other specific pain killers were added or changed. To optimize analgesic use, daily dose of prescribed analgesics was regulated first and then the class of pain medication was adjusted. For clinical characteristics analysis, we reviewed demographic data, BMD, hospitalization period, changes in the visual analogue scale (VAS) score, body mass index (BMI), and medical history such as smoking, alcohol, diabetes, and steroid usage. We also reviewed radiographs to evaluate vertebral body compression percentages and kyphotic angles. In order to evaluation the bone turnover, biochemical markers such as osteocalcin and C-telopeptide of collagen type1 are required, and computed tomography (CT) is required for bone microarchitecture evaluation. BMD was also performed in the initial phase, but additional follow-up was not performed. We assumed the compression percentage and kyphotic angles indirectly reflect bone quality.
Imaging assessment
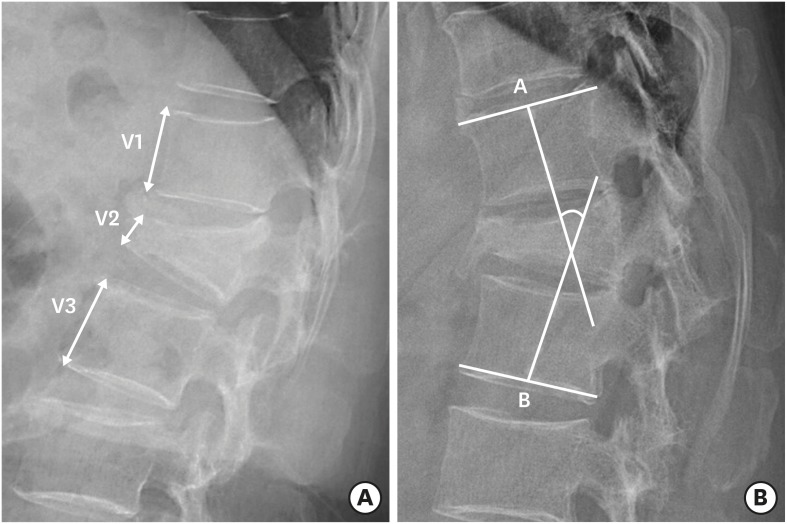
We measured vertebral body compression percentage and kyphotic angle. Vertebral body compression percentage was defined as the percentage of anterior vertebral body compression with respect to the average height of anterior vertebral bodies immediately cephalad and caudad to the injury level (formula: [1−V2/(V1+V3)/2]×100%) (FIGURE 1A). Kyphotic angle was determined by measuring the angle between the superior endplate of the vertebral body above and the inferior endplate of the vertebral body below the fractured vertebra on lateral radiograph (FIGURE 1B). Follow-up radiography was performed at baseline, 2 weeks, 3 months, 6 months, and 12 months after fracture diagnosis in both groups.
FIGURE 1
Measured factors. (A) Vertebral body compression percentage was calculated as the percentage of anterior vertebral body compression with respect to the average height of anterior vertebral bodies immediately cephalad and caudad to the injury level (formula: V2/[V1+V3]/2×100%) (B) Vertebral wedge angle (kyphotic angle). The angle between the superior endplate of the vertebral body above and the inferior endplate of the vertebral body below the fractured vertebra on the lateral radiograph.
Statistical analysis
SPSS statistical package (version 25.0; IBM Corp., Armonk, NY, USA) was utilized for all statistical analyses. Data are presented as mean±standard deviation. All p-values of less than 0.05 were considered to indicate statistical significance. VAS, vertebral body compression percentage, and kyphotic angle were compared to determine difference between the 2 groups using Wilcoxon rank sum test for follow-up time and Wilcoxon signed rank test with Bonferroni adjustment for changes between injury and follow-up time.
RESULTS
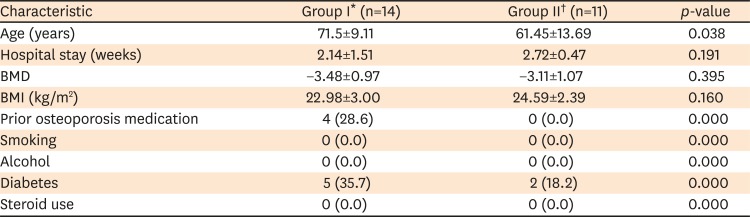
Male-to-female patient ratio was 3:22. Mean age of patients was 67.08 years. Location and number of the treated vertebrae were as follows: T6 (n=1), T10 (n=1), T11 (n=1), T12 (n=5), L1 (n=5), L2 (n=2), L3 (n=5), and L4 (n=5). Mean T-score was −3.34. The number of patients was 14 (56%) in group I and was 11 (44%) in group II. TABLE 1 shows demographic data comparison between the 2 groups. Unfortunately, baseline characteristics showed statistically significant difference in age (p<0.05), while other factors (hospital stay, BMD, and BMI) were similar between the 2 groups. Group I had higher rates of prior osteoporosis medication (28.6%) and diabetes (35.7%). Smoking, alcohol, and steroid usage were 0% in both groups.
TABLE 1
Demographic data
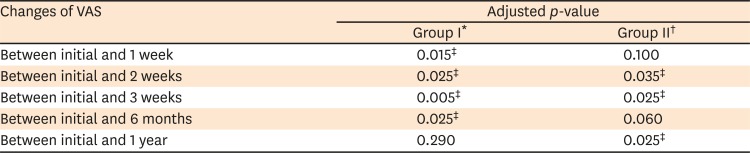
Mean VAS scores of groups I and II were 4.8±2.0 and 5.2±1.6 at injury, 2.5±1.7 and 3.2±1.3 at 1 week post-injury, 1.6±0.9 and 2.5±1.0 at 2 weeks post-injury, 1.5±1.2 and 2.4±1.5 at 3 weeks post-injury, 1.6±1.2 and 1.7±1.9 at 6 months post-injury, 2.6±1.7 and 2.4±1.2 at 1 year post-injury, respectively. Overall VAS scores were significantly improved in both groups at 2 and 3 weeks post-injury compared to those at injury. VAS scores at 1 week and 6 months post-injury were only significantly improved in group I. However, difference in VAS improvement at a specific time between 2 groups only showed statistically significant difference at 2 weeks post-injury (FIGURE 2, TABLE 2).
FIGURE 2
Changes of VAS. Group I: patients received teriparatide by injection, group II: patients did not receive teriparatide.
VAS: visual analogue scale.
*p<0.05.
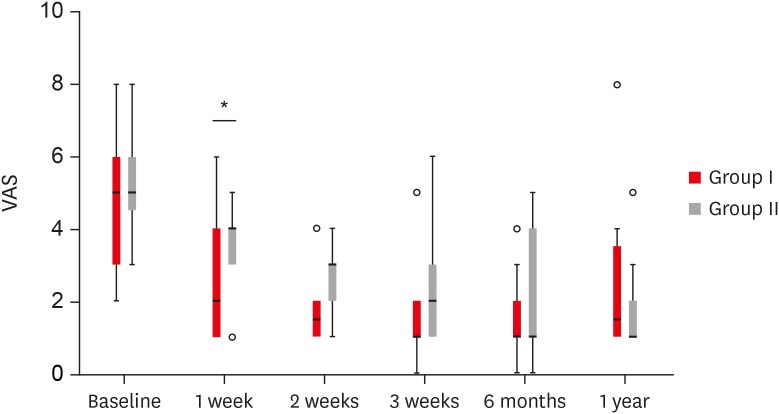
TABLE 2
Changes of VAS
Mean compression percentages of groups I and II were 17.9±11.9 and 23.6±9.7 at injury, 25.5±16.8 and 30.4±13.4 at 2 weeks post-injury, 26.1±14.5 and 42.3±17.1 at 3 weeks post-injury, 31.1±19.3 and 46.3±18.9 at 6 months post-injury, and 35.1±19.4 and 46.1±20.7 at 1 year post-injury, respectively. Overall change in compression percentage between injury and follow-up time was bigger in group II than that in group I, although difference between the 2 groups was statistically not significant. Compression percentage at 1-year post-injury was significantly increased compared to that at injury in both groups (FIGURE 3, TABLE 3).
FIGURE 3
Changes of compression percentage. Group I: patients received teriparatide by injection, group II: patients did not receive teriparatide.
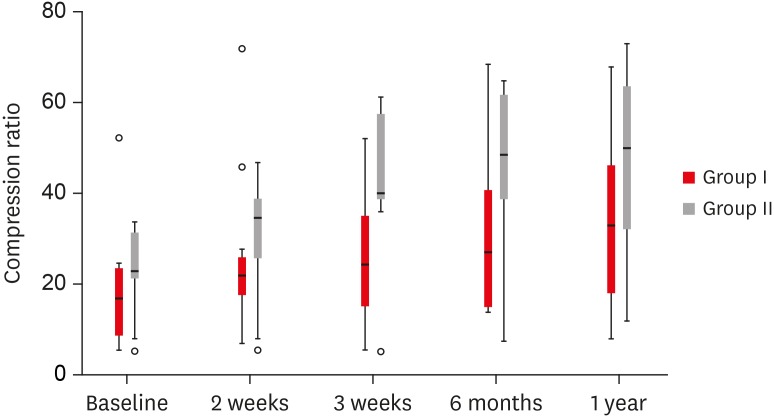
TABLE 3
Changes of compression percentage

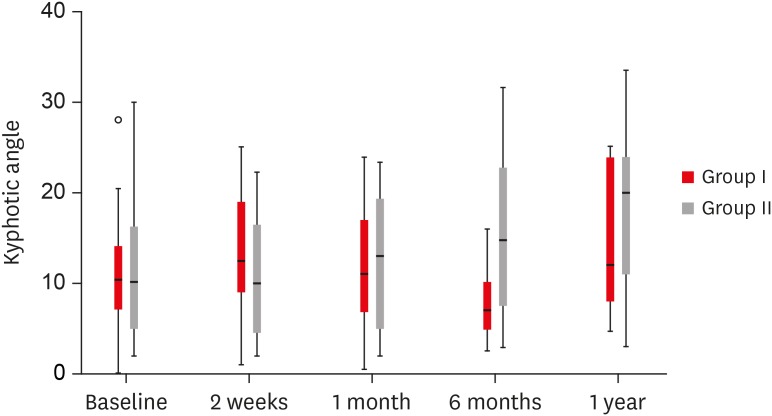
Mean kyphotic angles of groups I and II were 11.2±7.4 and 11.7±9.0 at injury, 13.4±6.8 and 11.3±10.8 at 2 weeks post-injury, 11.9±7.4 and 12.6±8.2 at 1 month post-injury, 7.8±4.4 and 15.6±9.8 at 6 months post-injury, and 14.7±10.8 and 18.3±9.5 at 1 year post-injury, respectively. Overall increase of kyphotic angle between injury and follow-up time was more in group II than that in group I, although the difference was statistically not significant. Changes in kyphotic angle between injury and any follow-up time were statistically not significant in both groups (FIGURE 4, TABLE 4).
FIGURE 4
Changes of kyphotic angle. Group I: patients received teriparatide by injection, group II: patients did not receive teriparatide.

DISCUSSION
Teriparatide, a recombinant human PTH, is an osteogenic osteoporosis agent. It has bone formation effect through direct and early stimulation of osteoblasts,6) prevention of osteoblast apoptosis,15) and increased osteoblast activity.68) Improvement of new bone formation will result in positive bone balance at the level of individual bone multicellular units, thus improving bone microarchitecture and quality.2135) Therefore, teriparatide is a preferential drug for osteoporosis to prevent fracture.26)
Previous randomized controlled trials have demonstrated that teriparatide can accelerate fracture healing.14) Aspenberg et al.3) have revealed that teriparatide can enhance fracture repair in 102 postmenopausal women with distal radius fracture in a prospective, randomized, double-blind study. Peichl et al.27) have performed a randomized controlled trial of 65 patients with osteoporotic pubic bone fractures and verified that a once-daily injection of PTH 1–84 can enhance healing compared to treatment with vitamin D and calcium.27) So, this pharmaceutical agent might potentially enhance fracture healing, and based on this knowledge, we assumed that teriparatide treatment after OVCF could improve bone strength and quality to prevent vertebral body collapse and kyphosis with increase of pain control.
Several studies have described that bisphosphonate has an analgesic effect.2224) Teriparatide can also decrease back pain, leading to rapid resolution for back pain compared to placebo and antiresorptive agents.26) These findings might be result of preventing micromovement of fractured vertebral body due to early bone-healing effects, rather than a direct analgesic effect. In the present study, overall VAS scores at 2 and 3 weeks post-injury were significantly improved in both groups compared to those at injury. However, VAS scores at 1 week and 6 months post-injury were significantly improved only in group I. Difference in VAS improvement at a specific time between the 2 groups was only significant at 2 weeks after injury (FIGURE 2, TABLE 2). Therefore, teriparatide injection group I showed more rapid pain control at early stage and more long-standing effect for the pain control. Our results are consistent with results of previous studies.3033)
Cancellous bone repair can be made by endochondral ossification. Some recent reports have shown that the intermittent teriparatide administration is related to accelerated formation of cartilage tissue due to accelerated bone union.162031) It might prevent vertebral collapse in the early stage. In this study, overall changes of compression percentage and kyphotic angle between injury and follow-up time were bigger in group II than those in group I, although the difference between the 2 groups was not statistically significant. However, compression percentages at 1 year after injury were statistically increased compared to those at injury in both groups (FIGURE 3, TABLE 3). Furthermore, change of kyphotic angle was not significantly different in either group (FIGURE 4, TABLE 4). These findings showed difficulty of preventing progression of vertebral collapse and kyphotic angles.
This study has some limitations. This was a retrospective analytic study. We were not able to conduct a randomized control study. Prospective studies are needed to determine the progression of vertebral collapse with longer follow-up period. Longer period of teriparatide usage is also needed to determine the optimal period for fracture healing. Long-term follow-up with many patients could powerfully analyze positive effects of teriparatide in conservative treatment after OVCF. In addition, only pain and radiologic factors were considered in this study. Moreover, economic outcomes were not analyzed.
CONCLUSION
This study did not show protective effects of 3-month of teriparatide on the progression of fractured vertebral body collapse or kyphotic changes in patients with osteoporosis. Therefore, further prospective studies are needed to evaluate the relative indication and effective treatment period for osteoporotic compression fracture in patients with thoracolumbar VCF.
 XML Download
XML Download