

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Osseointegrated implants have long been considered a dependable treatment for effectively restoring oral function and improving quality of life of edentulous patients.123 Particularly in the case of removable prostheses for mandibular edentulous patients, use of removable prostheses with dental implants are well documented to improve function, usually in the form of an implant overdenture with two or four implants.45
Mandible with severe alveolar bone atrophy poses a challenge to prosthodontists aiming to achieve successful oral rehabilitation.6 The shape of the posterior ridge often changes from a positive structure to a flat or negative one as the ridge atrophy progresses, making it hard to achieve a proper impression to reproduce clinically acceptable anatomy on the working cast.
In mandibular distal extension cases, an altered cast impression procedure has been recommended to improve the stability and support of the removable partial dentures with accurate reproduction of the anatomy of residual ridges.789 To avoid incorrect or incomplete seating of the framework in the mouth, a major potential complication of this procedure, stable stops for the framework are necessary.10
Inaccurate impression following unfit tissue surface of the denture causes sore spots, making it difficult for the patient to accommodate the new prosthesis. A precise impression with stable stops and accurate reproduction of a clinically acceptable tissue surface of the denture can resolve this issues. The combination of implant, fixed prosthesis and altered cast impression technique may help improve the accuracy of impression on atrophied mandible.
Case Report
An 80-year old woman visited the Department of Prosthodontics at Yonsei University, College of Dentistry. The chief complaint was pain on chewing on her mandible. The patient had a pair of old prostheses made in a private dental clinic, an upper removable partial denture and lower complete denture. She had a medical history of cerebral infarction and had trouble controlling her right hand due to hemiplegia.
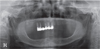
Clinical and radiographic examination revealed severe ridge resorption on the mandibular ridge, especially on the posterior region. On maxilla, there were 6 remaining teeth, from right second premolar to left central incisor, treated with a porcelain-fused-to-gold fixed partial denture (Fig. 1). She had no problem with the prosthesis on her maxilla, but could not use the lower complete denture due to pain from several sore spots. A dental implant could not be placed on the posterior region due to severe atrophy. Thus implant-retained overdenture with implants on both canine positions was planned.
The implant was placed at the Department of Periodontics. After 4 months of healing, a final impression with customized open tray was taken for implant abutment crowns. Milled bar and magnet were selected for the attachments of the first prosthesis to enhance implant support and stability. The magnets (Magfit Ex, Aichi Steel Co., Tokai, Aichi, Japan) were placed on the bar distal to each implant. The denture with milled bar and magnets was designed for easy and proper placement on the mandible by the hand-disabled patient (Fig. 2).
After the first implant overdenture was delivered, however, the patient consistently complained of sore spots on the posterior mandible for several months. Minor denture movements from the gap between the milled bar and denture seemed to keep causing soreness. The attachments were therefore changed to locator attachments (Kerator, Daekwang I.D.M, Seoul, Korea) to reduce the minor movement of the first prosthesis and the overdenture was remade (Fig. 3).
However, the patient was not able to chew with the second overdenture either, complaining of severe sore spots and lack of stability. Like the first overdenture with the milled bar attachment, the second prosthesis was unsatisfactory to the patient in restoring the chewing function.
Inaccuracy in terms of both the impression and reproduction of the anatomical details of the atrophied mandible seems to mainly account for the failure of both prostheses. Because proper placement of the customized tray was difficult without stable tissue stops, accurate impressions of the posterior ridge for the two former trials were compromised. Finally, an implant-assisted removable partial denture with two single implant abutment crowns was fabricated and installed on both canine regions. After the try-in of the metal framework, a customized tray for a secondary impression of the posterior region was connected to the framework (Fig. 4).
With the stable tray stops of the rest seat on the implant crowns, border molding of the posterior tray was done, and then a final impression was taken for the implant assisted removable partial denture (IARPD). An altered cast model was made and the denture was fabricated and delivered to the patient (Fig. 5). The patient complained of minor sore spots at the first two check-up appointments, but afterwards was able to chew without pain and eventually expressed satisfaction with the third prosthesis, reporting no sore spots.
Discussion
This 80-year-old woman had problems adapting to new restorations. First, her mandible was severely resorbed to a nearly flat alveolar ridge. Severe mandibular ridge atrophy poses a severe challenge to prosthodontists. Also, due to hemiplegia, she could not move her right hand, which made it hard to take the denture in and out. Moreover, most elderly patients don't recognize that they have lost proper muscle tone and movements. The patients always compare their new denture with a previous one that had satisfied them when they were younger. These considerations make it more difficult for the clinician to satisfy the patients.
It was difficult to obtain a precise impression in this patient due to her physical condition and atrophied mandible, which both aggravated the situation. However, by sticking to fundamental denture concepts, a clinician eventually finds solutions.
There is still no consensus on using implant crowns as abutments of removable partial dentures. However, several recent clinical reports have reported short- or long-term successes.111213 If clinicians do not greatly deviate from orthodox concepts regarding removable prosthodontic dentures when using implants as abutments, they can achieve successful rehabilitation within limited circumstances. In a case such as this, when the patient's condition is neither healthy nor stable, frequent recall check-ups are to be recommended.




 XML Download
XML Download