

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
With their high clinical success, dental implants are preferred for the rehabilitation of aesthetic and functional problems due to tooth loss. During functional movements, dental implants translate stresses to the surrounding tissues. Thus, the characteristics of bone quality and quantity around implants are biomechanically critical in implant dentistry.1 Insufficient bone height and an extensive trabecular structure, which can be seen in the posterior maxilla, could make the implant treatment complicated and cause failures.2 Obtaining the adequate bone height by sinus lifting and grafting may be needed. However, these procedures have complication risks and require technical skills, extra time, and higher costs.3 Although some studies24 claimed that short implants and tilted implants can cause more stress in the surrounding bone, short implants and tilted implants can be good alternatives to these advanced surgical procedures.5
Supplying optimal biomechanical status is important for establishing the prognosis of implant treatment. The materials used as implant-retained restorations can influence the dissipation of stress.6 Choosing material is related to aesthetics and strength features; therefore, zirconia restorations have recently become a popular treatment option.7 However, it is stated that fracture of the veneering porcelain in implantretained zirconia-fused porcelain restorations is a common problem.8 Therefore, monolithic zirconia has been developed to handle the chipping problem of zirconia-fused porcelain restorations.9 Although successful outcomes of monolithic zirconia restorations have been obtained, the longterm studies have not been sufficient to provide definitive conclusions related to monolithic zirconia.10 In addition to the material, stress levels and dispersion can be affected by the restoration designs.11 Thus, splinted and non-splinted restoration designs can change the stress levels. Although it has been claimed that better stress distribution can be achieved with splinting restorations, there is no consensus on splinting versus non-splinting restorations.12 How does design of monolithic zirconia restorations influence the stress dispersion on the bone surrounding implants?
Testing the stress on the bone surrounding implants is difficult in both in vitro and in vivo studies.13 As an alternative, finite element analysis (FEA) can be useful to evaluate the results about the stresses by imitating clinical conditions.14 FEA is an engineering method, and it has been used to assess biomechanics in implant dentistry since 1976.15 Generally, von Mises stress value is used to figure out stress dispersion in FEA studies.2412 Different from previous studies, the safety factor was added to the study for predicting the risks of whole structures found in the model.
The aim of this study is to analyze the stress distribution around the short and tilted implants on the atrophic posterior maxilla with different zirconia restoration materials using the 3D finite element method. The tested hypothesis is that splinted restorations decrease the risks for structures and stress on the bone surrounding implants.
Go to : 
MATERIALS AND METHODS
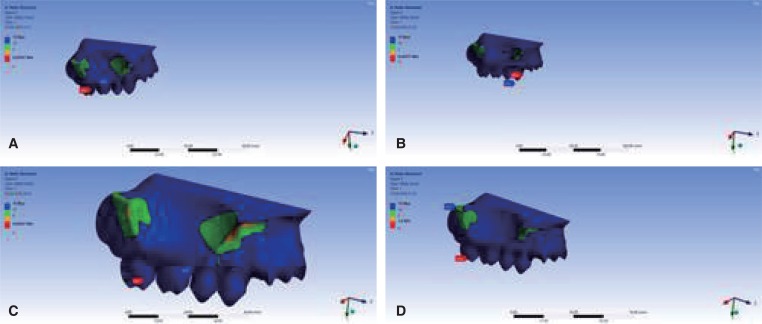
For the research, the solid 3D model was constructed by using a patient's tomography image from the radiology archive in Kocaeli University Dentistry Faculty. Data from the tomography were translated to stl (stereolithography) format via 3D-Doctor program (Able Software Corp., Lexington, MA, USA), which can design geometric models. Non-uniform rational basis spline (NURBS) surfaces were used from 3D Max (Autodesk, Inc., San Rafael, CA, USA), and 3D surfaces were obtained in this format. Subsequently, the model was converted to the format of DXF by C-FBX translator. The model was recorded in the IGES format; the surfaces of the model were arranged using the UG NX 6.2 program, and the structures of bone and maxillary sinus were designed. The bone was designed as trabecular bone as the cortical bone showed severe atrophy in the tomography image. The residual bone height was arranged as under 10 mm to imitate the condition requiring sinus augmentation. The research model was acquired for the analyses (Fig. 1A); the mucosa was not included, as in similar studies.216 The model was fixed by two planes to mimic the clinical position of maxilla following the previous research; these planes are the sagittal plane, which goes through the middle of the central incisors, and the horizontal plane, which passes the superior border of zygomatic bones.2
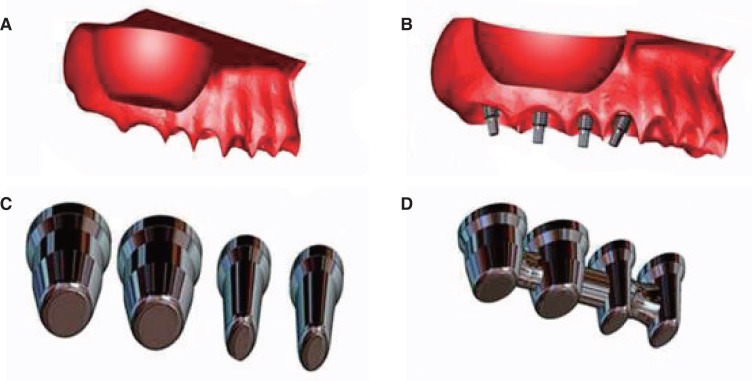 | Fig. 1(A) Three dimensional solid model, (B) Long implants and short implants with snappy abutments placed on posterior maxilla, (C) Non-splinted framework designs for monolithic zirconia and zirconia fused to porcelain restoration, (D) Splinted framework designs for monolithic zirconia and zirconia fused to porcelain restoration.
|
The model clinically imitates deficiency of the right maxillary premolars and molars. Parallel, conical connection implants (Nobel Biocare long: 15 × 3.75 mm and short: 7 × 3.75 mm) were selected. 3D images of the implants and the abutments were obtained from the catalogue by means of e-drawing program (Waltham, MA, USA). Then, 3D images were translated to Parasolid XT (Berkeley, CA, USA). One long implant placed in the position of first premolar was mesially tilted at a 17-degree angle along with the anterior wall of the maxillary sinus. The other long implant for second molar was placed as distally tilted at a 17-degree angle along with the posterior wall of the maxillary sinus and two short implants, one eached placed vertically in the second premolar and first molar. Snappy abutment, which is mainly used for cemented prosthesis, was chosen (Fig. 1B). The distance between implants was set at 1.5 mm, and the distance between implants and the crestal bone was set at 3 mm.17 The implants were accepted as being 100% osseointegrated.12
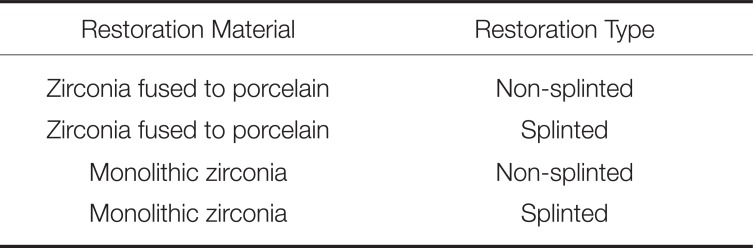
Teeth 14, 15, 16, and 17 were restored in the research. So, the form of the restoration was simulated according to the dimensions of described by Wheeler18 using the I-DEAS program (version ms 6, Electronic Daa Systems, Plano, TX, USA). The restorations were designed as splinted or non-splinted for each zirconia material. Two different restoration materials were prepared as zirconia-fused porcelain and monolithic zirconia (Fig. 1C, Fig. 1D). The thicknesses of the zirconia-fused porcelain used in the study were 1 mm and 1.5 mm. Similarly, the thickness for monolithic zirconia was 2.5 mm. Cement material was not included for the analysis because of its minimal effect.2
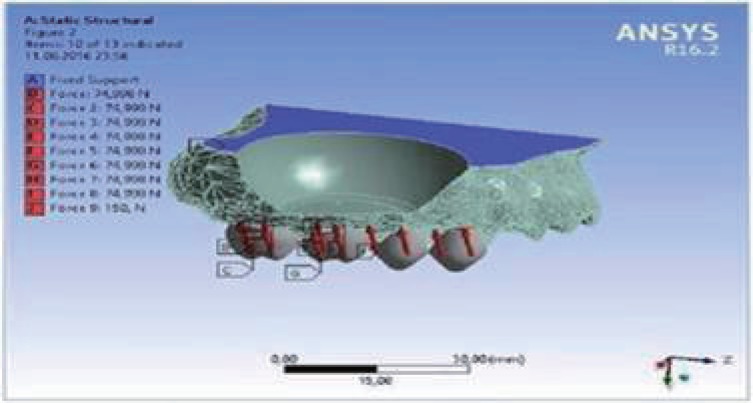
For all clinical attitudes, static load of 300 N were applied to 15° oblique to the long axis of the implants in the palato-buccal direction for imitating masticatory force.219 The force on the crowns were divided into equal parts. Force loads were distributed equally over the crowns (i.e. 300/2 N per cusp for premolars and 300/4 N per cusp for molars) assuming a balanced occlusal relationship with posterior contacts (Fig. 2).20 The model was evaluated for different clinical situations (Table 1).
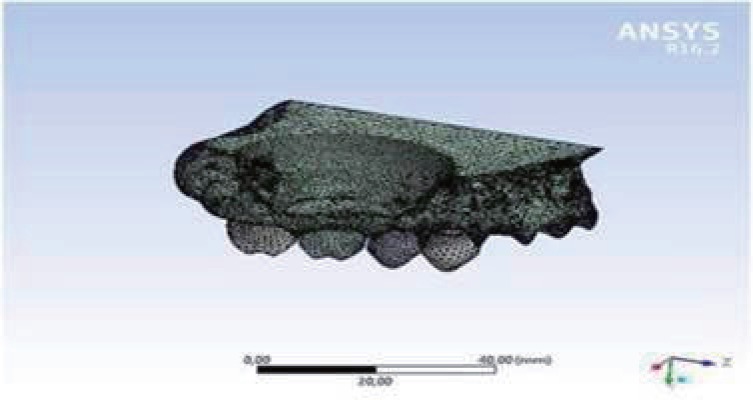
All materials in the study were supposed to be isotropic, homogenous, and linearly elastic.19 The suitable elastic properties, such as Young's modulus and Poisson ratios, were stated, considering similar studies in the literature (Table 2).2721 The meshing model was obtained from the geometric model by the free meshing method (Fig. 3). The homogenously distributed elements in all the structures were preferred in the meshing model for more realistic results. For the meshing model, which included all structures from bone to restoration, the number of elements was 541754, and the number of nodes was 91678. To analyze the stress, the model was imported to ANSYS R 16.2 (Ansys, Inc., Southpointe, Canonsburg, PA, USA), which is a 3D FEA program. The von Mises stress was used to figure out the dispersion of stresses that occurred at the bone structure and surface of the implants. In addition, the safety factor was evaluated for the understanding of the risks for all the clinical scenarios. This study did not need to be assessed using a statistical analysis, as FEA results did not have variance.2
Go to :
RESULTS
The defined values on the bones, implants, and safety factors in all models under 300 N oblique force are shown in Table 3.
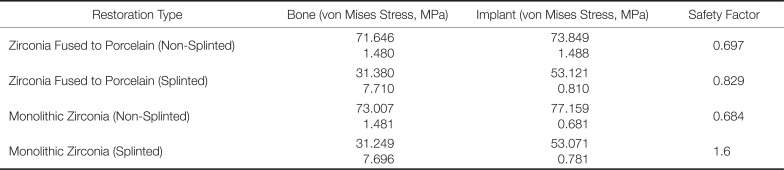
Table 3
The evaluating values for finite element analysis under oblique 300 N forces
![]()
The von Mises stress values for bone structures in all clinical scenarios are defined (Fig. 4). Considering restoration planning, stress dispersion at the peri-implant bone showed different patterns. Comparing the von mises stress values, the highest von Mises stress value at bone (73.007 MPa) was observed in the non-splinted monolithic zirconia model (Fig. 4C) and the lowest (31.249 MPa) in the splinted monolithic zirconia model (Fig. 4D).
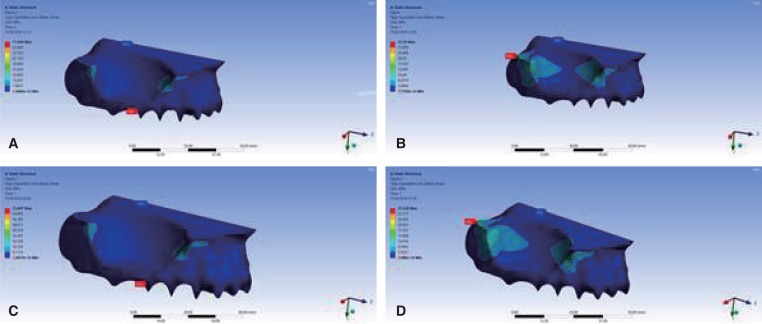 | Fig. 4(A) von Mises stress values of bone for non-splinted zirconia fused to porcelain restorations, (B) von Mises stress values of bone for splinted zirconia fused to porcelain restorations, (C) von Mises stress values of bone for non-splinted monolithic zirconia restorations, (D) von Mises stress values of bone for splinted monolithic zirconia restorations.
|
When evaluating stress distribution on the implant surfaces for all attitudes, it was observed that restoration type altered stress patterns on the implant surfaces. The von Mises stress values for implant surfaces are analyzed (Fig. 5). The highest von Mises stress value at an implant surface (77.159 MPa) was observed on the neck of the first premolar implant in the non-splinted monolithic zirconia model (Fig. 5C) and the lowest (53.071 MPa) in the apical area of the second molar implant in the splinted monolithic zirconia model (Fig. 5D).
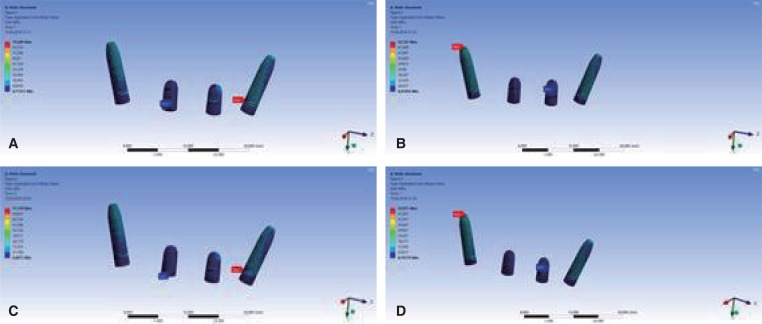 | Fig. 5(A) von Mises stress values of implants for non-splinted zirconia fused to porcelain restorations, (B) von Mises stress values of implants for splinted zirconia fused to porcelain restorations, (C) von Mises stress values of implants for non-splinted monolithic zirconia restorations, (D) von Mises stress values of implants for splinted monolithic zirconia restorations.
|
Also, minimum safety factors were evaluated to estimate possible clinical results (Fig. 6). The highest minimum safety factor (1.6) was detected at the bone surrounding the second molar in the splinted monolithic zirconia model (Fig. 6C) and the lowest (0.684) at the bone between the first molar and second premolar implants in the non-splinted monolithic zirconia model (Fig. 6D).
 | Fig. 6(A) Safety factor values of all structures for non-splinted zirconia fused to porcelain restorations, (B) Safety factor values of all structures for splinted zirconia fused to porcelain restorations, (C) Safety factor values of all structures for non-splinted monolithic zirconia restorations, (D) Safety factor values for splinted monolithic zirconia restorations.
|
In general, higher stress values and lower safety factor values were observed in the non-splinted models when compared to the splinted models. Moreover, the safety factor value for the non-splinted design of the monolithic zirconia restoration indicated a risk of failure for bone structure. So, splinting zirconia fused to porcelain restorations did not have significiant effect on safety factor, but there was an increase in safety factor when monolithic zirconia restorations were splinted.
Go to :
DISCUSSION
The clinical success of implant treatment is related not only to biological factors, but also to biomechanical factors. As a biomechanical factor, occlusal forces affect the bone surrounding implants, and it has been shown in animal experiments that high stress causes bone resorption.22
Implant-supported restorations are important for stress distribution, and rigid materials are advised to prevent complications.23 Recently, zirconia materials with the chemical stability, good mechanical properties, and aesthetic colour successfully fulfill patients' and clinicians' demands.24 Also, zirconia can be a good option for implant retained restoration considering its high biocompatibility to peri-implant soft tissues and minimal bacterial adhesion.25
The total thickness of the zirconia-fused porcelain restoration must be at least 2 mm to prepare the veneer.26 In this study, the thickness of the prepared restorations was 2.5 mm. Thus, the comparison of the two types of materials was not affected by the thickness. It could be claimed that the implant and bone stress values were higher in the monolithic zirconia models than in the zirconia-fused to porcelain models. In the monolithic zirconia models, the minimum safety factors were identified at the bone. Porcelain's elastic modulus is lower than that of zirconia.27 Thus, porcelain can absorb stress better than monolithic zirconia can and transmit less stress to the bone and implant.28 Also, occlusal thickness of zirconia can change fracture resistance of restoration under chewing forces.29 In the study, the thickness of monolithic zirconia was arranged as same as zirconia fused to porcelain for standardizing the restorations. However, increasing thickness of monolithic zirconia may cause higher stress values on the surrounding bone of implants. In a previous study, implant-supported restorations of monolithic zirconia in full mouth rehabilitation were assessed. Chipping complications could be seen in the experimented period, but the long-term results for peri implant tissues were unknown.10
Design of restoration is another factor that can affect stress distribution. Studies have reported different results about the biomechanics of splinted and non-splinted restorations.12 While some studies have found no significant differences between the success rates of splinted and non-splinted restorations,3031 it was stated that splinted restorations with angulated implant may induce more severe force because they alter the direction of occlusal forces.32 Guichet et al.33 showed better stress distribution for splinted restorations than non-splinted ones. Similarly, in this study, the stress values of bone in the splinted restoration models were lower than those in non-splinted models. However, the maximum stress areas of the implants were different in the splinted and non-splinted restoration models. In the splinted restoration models, the maximum stress converged apically on the implant on the molar. In contrast, the maximum stresses were detected on the cervical part of the implant for the premolar in the non-splinted models. This may be due to lack of cortical bone similar to the study results by Okumura et al.34 This can be explained by a higher modulus of elasticity in cortical bone than trabecular bone. So, it can change stress direction and distribution.
The bone feature is essential factors in implant stability. Goiato et al.35 reported that the diversity of bone and survival rate of implants are related to each other. The cortical and trabecular structure of bone affects the stress distribution and implant success. However, bone anatomy is complex, and it can change from person to person. The cortical structure may not always be seen clinically.4 In a previous study, when implants were placed more apically, the researchers found that the stress and strain increased because of greater contact with trabecular bone.19 Similarly, in this study, higher von Mises stresses were detected than the values reported in the literature because of the deficiency of cortical bone.246
FEA is a feasible method for simulating real structures easily, and it is widely used in studies of implant dentistry and the understanding of stress distribution.12 The finite element method can be applied in two or three dimensions. A two-dimensional (2D) method is commonly preferred for simple evaluation. In this study, the 3D finite element method was used owing to the complexity of the model and multiplicity of materials.36 Thus, the right posterior maxilla region was modelled for this study. Generally, in FEA studies, von Mises stress and principle stress values are assessed.412 However, the safety factor can be used to provide important data about the risks of the evaluated clinical condition. When the safety factor value is under 1, it indicates possible risks.37 According to the safety factors in the study, chipping is seen in splinted and non-splinted zirconia fused to porcelain. In assessing monolithic zirconia, the safety factor indicated probable bone resorption for non-splinted restorations, and splinting should be beneficial for protecting the bone structure.
Like in other finite element studies, this study had some limitations relating to the clinical conditions, material properties and loading properties.38 Clinically, an implant cannot be 100% osseointegrated, and structures cannot be homogenous. In addition, chewing movements cause dynamic forces. In future studies, non-homogenous models should be evaluated under dynamic loadings.
Go to :
CONCLUSION
In finite element studies, generally, von Mises and principle stress values are considered. For this study, not only the stress values but also the safety factor was evaluated, in contrast to previous studies. Within the limitations of the research, the following conclusions can be drawn: splinting monolithic zirconia restorations can effectively decrease the stress values. The minimum safety factors showed better recovery when splinting monolithic zirconia. Thus, monolithic zirconia was selected as the restoration material on the atrophic bone, and splinted restoration should be preferred to reduce bone stresses.
Go to :
 XML Download
XML Download