

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Implant surgery in the dental field has rapidly developed in terms of materials and techniques. It has been widely used in clinical practice as a way to restore missing teeth without tooth preparation of the adjacent teeth. However, as implant surgery is performed more frequently, nerve injury is also increasing as a complication [123]. The inferior alveolar nerve (IAN) is the most commonly damaged nerve in such complications [45].
Nerve injuries vary from short-term neurosensory disturbances to complete paresthesia and permanent dysfunction [6]. In previous studies, postoperative dysesthesia after implant placement was reported in 1.7%–43.5% of cases and permanent sensory disturbance (after more than 1 year) was present in 5%–15% of cases [278].
If a patient complains of sensory abnormality after mandibular implant surgery, the possibility of nerve injury should be considered, and panoramic and intraoral radiography are performed as the first radiological diagnostic tools. It may be difficult to obtain information using these 2-dimensional (2D) imaging methods about whether the implant fixture invades the mandibular canal (MC). Thus, 3D imaging methods, such as computed tomography (CT) and cone-beam CT, should be additionally performed as part of the evaluation.
Nerve disturbance from dental implant surgery often degrades a patient's quality of life and causes negative psychological effects. In particular, iatrogenic IAN damage has been reported to occur in many cases, sometimes leading to medico-legal problems [1]. Nevertheless, there is insufficient information on the relationships among the radiological evaluation, patients' symptoms, and recovery in cases of nerve disturbance.
This study classified CT images based on the distance between the implant fixture and the MC, investigated the distribution of various neurosensory disturbance symptoms after mandibular implant surgery, and explored the relationships of these parameters with the prognosis for recovery.
MATERIALS AND METHODS
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Yonsei University Dental Hospital (IRB No. 2-2018-0013). Patient consent was exempted by IRB due to retrospective study.
Subjects
Of the total of 286 Korean patients who visited Yonsei University Dental Hospital between 2008 and 2017 for nerve disturbance after implant surgery in the mandibular posterior area, 56 patients who met the following inclusion criteria were selected.
CT image classification
CT scans were obtained using a Highspeed Advantage (GE Medical Systems, Milwaukee, WI, USA) CT scanner, and the images were reformatted in panoramic and cross-sectional views of the mandible using DentaScan software (GE Medical Systems). Two oral and maxillofacial radiology specialists with more than 10 years of experience independently evaluated the distance between the implant fixture bed and the MC, and classified the scans into 4 groups. If the implants had been removed, the image evaluation was performed based on the bony defect caused by drilling for implant fixture insertion. The radiologists agreed on the definitions for the classification of the 4 groups, and in cases of disagreement, consensus was achieved through discussion. The radiologists had no information about any of the individuals included in this study.
Both observers used 2 liquid crystal display monitors (21.3 inches; resolution, 1,260×2,048 pixels; Totoku Electric Co., Nagano, Japan), and were permitted to adjust the sharpness, brightness, and contrast on axial, cross-sectional, and reformatted panoramic images. CT images were evaluated and classified as belonging to the following 4 categories to analyze inter-observer reliability (Figure 1).
Figure 1
Each computed tomography image was classified into 1 of 4 groups according to the distance from the implant fixture to the mandibular canal. (A) Intrusion group, (B) Contact group, (C) Close group, and (D) Separate group.

1) Intrusion: a discontinuity of the cortical roof of the MC caused by the implant or drilling bony defect during surgery is seen clearly (a score of 1; Figure 1A).
2) Contact: the implant or drilling bony defect is in contact with the cortical roof of the MC with loss of continuity (a score of 2; Figure 1B).
3) Close: the implant or drilling bony defect is apart from the cortical roof of the MC, within 1 mm (a score of 3; Figure 1C).
4) Separate: the implant or drilling bony defect is clearly apart from the cortical roof of MC, by more than 1 mm (a score of 4; Figure 1D).
Symptom classification
All paresthesia-related symptoms that the patients reported at the first visit were investigated and classified into 8 groups. Multiple responses were allowed.
Group A included cases with a sensation of electric shock; group B, an aching feeling similar to sore muscles; group C, a burning sensation or sensation of being on fire; group D, a formication or worm crawling sensation under or on the skin; group E, a feeling of pins or needles stuck into the skin; group F, a tightening sensation. Symptoms that appeared in only a single patient were included in group G (pressure sensation, stiffness, toothache, etc.). Group H was categorized as having no other symptoms other than numbness.
Symptom improvement classification
All patients with sensory disturbances were divided into 2 groups (recovery and no recovery). No recovery was defined as improvements in 2 or fewer symptoms from the previous visit. Recovery was defined as improvements in 3 or more symptoms or the absence of discomfort in daily life.
Statistical analysis
The intraclass correlation coefficient (ICC) of the 2 radiologists for the CT image classification was calculated with a 95% confidence interval (CI). The distribution of CT evaluations, symptoms, and improvements were investigated in terms of frequency and by using a cross-table based on multiple response analysis. The linear-by-linear association test was used to assess the relationship between the CT evaluation-based classification and improvement, between the CT evaluation-based classification and groups of symptoms, and between groups of symptoms and improvement. Statistical analyses were performed using SPSS (version 23.0; IBM Corp., Armonk, NY, USA) and the significance level was defined as 5%.
RESULTS
The inter-observer ICC value of the CT image evaluations by the 2 radiologists was 0.884 (95% CI, 0.802–0.932). Table 1 presents the age and sex distribution of subjects. The 56 patients who satisfied the inclusion criteria were aged between 29 and 74 years (mean age, 54.4 years), and included 9 males and 47 females.
Table 1
Age and sex distribution of study subjects

| Age groups (yr) | Males | Females | Total |
|---|---|---|---|
| 20–29 | 0 | 1 | 1 |
| 30–39 | 0 | 3 | 3 |
| 40–49 | 5 | 7 | 12 |
| 50–59 | 2 | 20 | 22 |
| 60–69 | 2 | 14 | 16 |
| 70 | 0 | 2 | 2 |
| Total | 9 | 47 | 56 |
Based on the CT image classification, the intrusion group included 18 cases, the contact group 16, the close group 11, and the separate group 11. Additionally, 38 of the 56 patients with nerve disturbance experienced improvements (Table 2). The close and separate groups in the CT classification showed a strong tendency for symptom improvement, at 90.9% and 81.8%, respectively, and these rates showed a statistically significant difference compared to the other groups (P<0.05). The intrusion group showed the lowest rate of recovery, but it was non-negligible, at 50%.
Table 2
Distribution of CT image classification according to symptom improvement

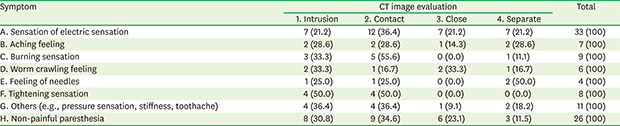
The relationship of the CT evaluation-based classification with the symptom classification is shown in Table 3. Overall, there was no correlation between symptoms and the CT evaluation. However, the frequency of symptom C (burning sensation) was higher in the intrusion group (33.3%) and the contact group (55.6%) than in the close group or the separate group. Symptom F (tightening sensation) occurred in 50% of patients in both the intrusion and contact groups, but did not occur in the close and separate groups. Table 4 shows correlations between the CT image evaluation and presence or absence of symptom F (tightening sensation). Statistical significance was found for the linear-by-linear association test (P<0.05).
Table 3
Distribution of paresthesia types according to CT image classification

Table 4
CT image evaluation with regard to presence of symptom F (tightening sensation)

Table 5 shows the distribution of symptoms according to the type of paresthesia. Among the 8 subtypes from 56 patients, an electric shock sensation was the most common (31.7%), while the feeling of needles was the least common (3.8%). The 6 patients with a worm crawling sensation improved, while the patients with a tightening sensation were the least likely to improve, at 12.5%. Symptom improvement was less common when symptom F (tightening sensation) was present, as only 12.5% of patients with symptom F recovered. There was a statistically significant difference in the recovery rate depending on the presence or absence of symptom F (P<0.05, Table 6).
Table 5
Distribution of paresthesia types according to symptom improvement

Table 6
Recovery rates according to the presence of symptom F (tightening sensation)

| Symptom F (tightening sensation) | Symptom improvement | Total | P value | |
|---|---|---|---|---|
| No recovery | Recovery | |||
| Presence | 7 (87.5) | 1 (12.5) | 8 (100) | 0.001a) |
| Absence | 11 (22.9) | 37 (77.1) | 48 (100) | |
When the implant fixture was removed, the time interval from implant surgery to removal was found to be between 0 and 21 days. In 14 patients, the implant fixtures were removed within 2 days after surgery, and 11 of them showed symptom improvement. Although 6 of those patients belonged to the intrusion group, they also showed symptom improvement (Supplementary Table 1).
The average time from symptom onset to recovery was 17.42 weeks (range, 1.29–42.57 weeks) (Supplementary Table 1).
DISCUSSION
Implant fixture intrusion into the MC is one of the most common complications after implant surgery, and sometimes there is the potential for permanent damage of the IAN [910]. Irreversible damage of the IAN is much more frequently caused by implant surgery than by tooth extraction [7]. Direct (mechanical or chemical) trauma from drilling, indirect trauma (hemorrhage or hematoma), overheating during implant site preparation, excessive stretching during the flap procedure, and the needle stick stimulus during anesthesia can result in nerve injury [2111213]. Previous researchers reported that the blood vessels lay above the IAN within the MC, and the nerve was observed along the linguo-inferior side of the MC [1415]. When damage of the vessels in the MC is caused by direct or indirect injury, hemorrhage can occur, resulting in compression of the underlying nerve [1617].
Females generally tend to be more sensitive to this complication than males and to be overrepresented among patients who experience it [181920]. The results of this study are similar to that of previous research in this regard, as there were only 9 males, compared to 47 females, in the total sample of 56 patients.
In previous research, it was reported that when the nerve is only slightly compressed and the perineurium layer of the nerve can protect the nerve fiber from compression stimuli [13], recovery is expected. In this study, half of the patients in the intrusion group, as classified by CT, recovered. This result suggests that superior cortical involvement of the MC does not mean complete bisection of the nerve tissue.
However, in the close and separate groups in this study, no recovery took place in 9.1% and 18.2% of patients, respectively. Previous studies reported that even if the implant bed does not intrude into the MC, when it is close to the canal cortical roof, nerve injury may occur due to accumulation of debris or nerve compression caused by hematoma [421]. The compression can lead to neurosensory disturbances, although the implant does not damage the nerve directly.
While 6 patients with the symptom of a worm crawling sensation recovered, only 12.5% of the cases with a tightening sensation did so and the symptom of a tightening sensation occurred only in the intrusion and contact groups of the CT image evaluation. It is hypothesized that if the patient has a crawling symptom at the first visit, there is a high likelihood that the patient will recover, but that the patient will be unlikely to recover if he or she has a tightening sensation at the first visit. Worm crawling or a tightening sensation at the first visit may be a predictor of a positive or negative prognosis, respectively.
Previous studies reported that it is important to remove the pressure caused by the implant fixture [6222324]. Khawaja et al. [22] reported that when the implant was removed within 36 hours, patients' symptoms recovered. We observed a similar finding in this study. Symptoms improved in 78.6% of the patients who underwent implant removal within 2 days, and even in the intrusion group, all patients whose implants were removed within 2 days showed symptom improvement.
This study has several limitations. Symptoms of neurosensory disturbance may change while becoming chronic [2125], but this study focused on initial symptoms. Furthermore, the patients' symptoms were analyzed based on medical records, so the most common symptoms were classified into 8 groups. In the future, a prospective study of the correlations between image evaluation and symptoms should be performed, possibly leading to greater clinical significance. However, our findings regarding the distribution and the relationships of improvements in nerve disturbance with the CT evaluation classification and symptoms are thought to be meaningful, and will help clinicians to predict patients' prognoses and to plan treatment when patients experience undesired complications.
This study aimed to include a large number of patients, and it is important to categorize the various symptoms of patients, as well as the positional relationship between implant fixtures and the MC on 3D CT images. This study is almost unique in that it examined the relationships of CT imaging with prognosis and symptoms.
In conclusion, half of the cases where the fixture appeared to intrude into the MC on CT images recovered, so this finding does not mean complete bisection of the nerve tissue. Among the various symptoms of paresthesia, a worm crawling feeling has the potential to be a predictor of symptom recovery, but when a tightening sensation was present, improvement was less likely.
 XML Download
XML Download