

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Malignant melanoma (MM) is one of the most aggressive known skin tumors due to its frequent metastases, high mortality rate, and resistance to available therapies. Worldwide, 160,000 new melanoma cases are diagnosed each year and the incidence of MM has increased recently.1 The incidence of particular subtypes of MM varies according to the type of skin; superficial spreading melanoma (SSM) is the most common type in Caucasians, while acral lentiginous melanoma (ALM) is most commonly reported in Asians.2345
MM is a rare disease in Asians because of the protection conferred by pigmented skin, but the incidence shows an upward trend in Koreans.678 However, information on the clinicopathologic characteristics and prognostic factors of cutaneous melanoma is limited in Korea.
In this study, primary cutaneous melanoma cases diagnosed in seven centers over the course of 21 years were investigated retrospectively. The objective of this study was to describe the epidemiological and clinicopathologic characteristics of primary cutaneous melanoma in Korean patients and to identify the clinicopathologic variables associated with the clinical course of primary cutaneous melanoma, including metastases, and overall survival (OS).
METHODS
Patient selection and study design
The electronic medical records of all primary cutaneous melanoma cases diagnosed between 1997 and 2017 in seven medical centers (Hallym University Kangdong Sacred Heart Hospital, Hallym University Dongtan Sacred Heart Hospital, Hallym University Kangnam Sacred Heart Hospital, Hallym University Chuncheon Sacred Heart Hospital, Soonchunhyang University Seoul Hospital, Soonchunhyang University Bucheon Hospital, and Soonchunhyang University Cheonan Hospital) were retrospectively reviewed. All cases were confirmed as primary cutaneous melanoma after histopathologic testing, by a dermatologist and pathologist. Non-cutaneous MM was excluded.
Data on the following variables were collected and analyzed: age, gender, body mass index (BMI), site of primary lesion, histologic subtype, Breslow tumor thickness, Clark level, presence of ulceration, metastasis (presence or absence, and first metastatic site), and period of survival. Patients were categorized into two different groups according to their age at diagnosis: 0–59 years and 60 years or older. Primary cutaneous melanoma was classified into four groups according to its anatomical location: head and neck, hand and foot, extremities, and trunk. The histologic subtype was categorized based on the World Health Organization classification: SSM, nodular melanoma (NM), ALM, and lentigo maligna melanoma (LMM). According to the American Joint Committee on Cancer (AJCC) staging system, tumor thickness and invasion were assessed by the staging systems of Breslow and Clark, respectively. The survival time was defined as the interval between the date of diagnosis of the primary cutaneous melanoma and the registered date of death or the date of the last consultation. We defined and classified these variables based on previous reports about malignant melanoma.91011121314
Statistical analyses
The Kaplan-Meier method and multivariate Cox's proportional hazards analysis were used. The associations were summarized by using hazard ratios (HRs), odds ratio (OR) and 95% confidence intervals (CIs). OS was calculated by the Kaplan-Meier method with a CI of 95%. Differences were considered significant at P < 0.05. Statistical analyses were performed using SPSS for Windows statistical software package (version 21.0; SPSS Inc., Chicago, IL, USA).
Ethics statement
This study was approved by the Institutional Review Boards (IRBs) of Soonchunhyang University Hospital Cheonan and Hallym University Kangnam Sacred Heart Hospital (IRB No. 2017-09-006-001 and 2017-10-011, respectively). Informed consent was not obtained because this was a retrospective study using clinical data.
RESULTS
Between 1997 and 2017, a total of 261 patients were diagnosed with primary cutaneous melanoma in seven medical centers. All electronic medical records were retrieved and reviewed. The men-to-women ratio was 1:1.3. The mean age of the patients was 62 ± 15.8 years (range, 21–99 years). The median follow-up period for the entire cohort was 18 months (range, 1–210 months). The anatomic distribution and histopathologic features of the melanomas in our study are shown in Table 1. We compared clinicopathologic features of our patients with previous reports (Table 2).15161718
Table 1
Clinical and histopathologic features of 261 primary cutaneous melanomas
Values are presented as number (%).
CM = cutaneous melanomas, SSM = superficial spreading melanoma, NM = nodular melanoma, ALM = acral lentiginous melanoma, LMM = lentigo maligna melanoma, NOS = not otherwise specified.
a0–59 years; b≥ 60 years.
![]()
Table 2
Clinical and histopathological features of melanoma patients in previous reports

| Study (year) | Total patient number | Gender (men:women) | Mean age at diagnosis | Frequency of melanoma subtype | Most common location | Most common/Mean Breslow depth, mm | Presence of ulcer, % |
|---|---|---|---|---|---|---|---|
| Park et al.15 (2007) | 97 | 1:1.2 | 59.7 | ALM > NM > SSM = LM & LMM | Feet | 2.01–4 (22.2%) | 45.6 |
| Jang et al.16 (2014) | 206 | 1:1.03 | 60 | ALM > MM > NM > SSM > LMM > Unclassified | Acral | 4.45 | 27.7 |
| Nam et al.17 (2015) | 100 | 1:1.8 | 55 | ALM > NM > SSM > LMM | Feet | ≥ 4.01 (32%) | - |
| Lee et al.18 (2018) | 122 | 1.26:1 | 61.2 | ALM > SSM > NM | - | > 1 to ≤ 2 (39.3%) | 29.5 |
| Current study | 261 | 1:1.3 | 62 | ALM > NM > SSM > LMM | Hand and foot | 1.01–2.00 (27.6%) | 41.0 |
ALM = acral lentiginous melanoma, NM = nodular melanoma, SSM = superficial spreading melanoma, LM= lentigo maligna, LMM = lentigo maligna melanoma, MM = mucosal melanoma.
![]()
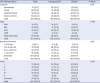
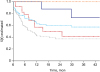
The 1-, 2-, and 5-year OS for the entire group was 63.3%, 55.4%, and 51.9%, respectively. The mean survival time was 83.9 months (95% CI, 64.7–103.1) and the median OS was 65.4 months (95% CI, 13.5–117.4) (Table 3). A total of 109 patients (41.8%) had metastasis of the melanoma in the brain, gastrointestinal tract, liver, lung, or distant lymph node at diagnosis or during the follow-up period. The first location of metastases was the brain in 20 (7.7%), liver and gastrointestinal tract in 33 (12.6%), lung in 31 (11.9%), and extra-regional distant lymph node plus others in 25 (9.6%) patients (Table 4). The median OS from the time of detection of any metastasis was only 7.8 months (95% CI, 6.1–9.4) and the mean survival was 9.9 months (95% CI, 8.1–11.7). The 1-year OS of stage IV patients was 28.6% and the 2-year OS was 14.3%. By Cox regression, the median OS is showed to have increased 17.7-fold without metastasis (P < 0.001). We found that MM patients with brain metastasis had the lowest median OS, of only 2.79 months (95% CI, 0.69–4.89), followed by patients with metastases in the liver and gastrointestinal tract (median OS of 5.96 months; 95% CI, 4.39–7.53) and lung metastases (median OS, 7.50 months, 95% CI, 3.42–11.58) (Table 4 and Fig. 1).
Table 3
OS rate and median OS

| Survival rate | % |
|---|---|
| 1-yr survival rate | 63.3 |
| 2-yr survival rate | 55.4 |
| 5-yr survival rate | 51.9 |
| Median OS, mon | 65.4 |
![]()
Table 4
Distribution of first metastatic site and OS rate for stage IV patients according to first metastatic site

![]()
 | Fig. 1Kaplan-Meier overall survival for American Joint Committee on Cancer stage IV cutaneous melanoma patients depending on the first metastatic site. Brain metastasis (blue line), liver and gastrointestinal tract metastasis (red line), lung metastasis (skyblue line), and distant lymph node metastasis and others (orange line).
|
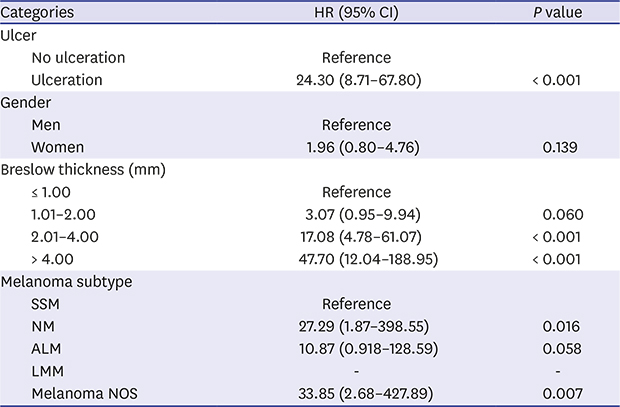
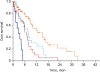
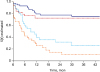
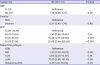
According to the Kaplan-Meier method and Cox's multivariate analysis, the following variables were risk factors for the development of metastasis of primary cutaneous melanoma: NM type (P = 0.016), Breslow thickness > 2.00 mm (P < 0.01), and ulceration (P < 0.001) (Table 5 and Figs. 2-4). Multivariate analysis of the clinicopathological variables associated with increased Breslow thickness was also performed. Patients whose data were not fully investigated were excluded. Gender and histologic subtype were not significantly associated with Breslow thickness (P > 0.05). As age increased, so too did the Breslow thickness, but this association did not reach statistical significance. However, overweight and obesity (BMI > 23) was significantly associated with increased Breslow thickness (P < 0.01). (Table 6). Thus, we additionally evaluated the direct effects of overweight and obesity (BMI > 23) on the development of metastasis and OS. The risk associated with the development of metastasis was significant with an OR of 2.10 (95% CI, 1.2–3.6). Moreover, overweight and obesity (BMI > 23) was also significantly associated with shorter OS (P = 0.033).
Table 5
Cox multivariate analysis for metastasis

HR = hazard ratio, CI = confidence interval, SSM = superficial spreading melanoma, NM = nodular melanoma, ALM = acral lentiginous melanoma, LMM = lentigo maligna melanoma, NOS = not otherwise specified.
![]()
 | Fig. 2Kaplan-Meier curves showing the time of metastasis in patients with primary cutaneous melanoma according to Breslow thickness. Breslow thickness < 1 mm (blue line), Breslow thickness = 1.01–2.00 mm (red line), Breslow thickness = 2.01–4.00 mm (skyblue line), and Breslow thickness > 4 mm (orange line).
|
 | Fig. 3Kaplan-Meier curves showing the time of the metastasis in patients with primary cutaneous melanoma according to the histologic subtype. Lentigo maligna (orange line), superficial spreading (blue line), acral (skyblue line), nodular (red line), and not otherwise specified (gray line).
|
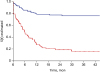 | Fig. 4Kaplan-Meier curves showing the time of metastasis in patients with primary cutaneous melanoma according to the presence of ulceration. No ulceration (blue line), and ulceration (red line).
|
Table 6
Cox multivariate analysis of clinicopathologic variables associated with Breslow thickness
HR = hazard ratio, CI = confidence interval, BMI = body mass index, SSM = superficial spreading melanoma, NM = nodular melanoma, ALM = acral lentiginous melanoma, LMM = lentigo maligna melanoma, NOS = not otherwise specified.
aCategorized in three groups.
![]()
DISCUSSION
MM is a malignant tumor originating from melanocytes of the skin and other organs, and is characterized by a high risk of metastasis and death. This study demonstrated the epidemiologic and clinicopathologic characteristics of primary cutaneous melanoma in a number of centers in Korea. Prognostic clinicopathologic variables potentially related to the disease course of MM, in terms of the development of metastases and OS, were also evaluated.
In our study, the most common site of cutaneous melanoma was the hand and foot (44.4%), and the most common histopathologic subtype was ALM (44.1%). These results agree with those of previous studies of melanoma in Korea and other Asian countries, which also described the most common site as hand and foot.12192021 In terms of histologic subtype, a previous study of melanoma in Korea also found that ALM accounted for more than 70% of all cases.22 In addition, ALM was the most common type of melanoma in a Chinese study, accounting for nearly half of all cases, while the sum of the incidences of NM, SMM, and LMM was less than half the incidence of ALM.23 Regardless of type, 41.4% of the melanoma patients in the present study had AJCC stage IV disease. Among them, 42 patients (16.1%) had stage IV ALM. Jung et al.24 noted the proportion of Korean ALM patients presenting with stage IV disease and showed that 5.4% of ALM patients had metastases. Data from Chinese populations showed that stage IV ALM represented 2.8% of all cases.25 In the present study, the prevalence of AJCC stage IV ALM was higher than in other Asian studies. We consider this result to be due to the fact that ALM is usually detected at a later stage than other types of melanoma in Asians and that all involved medical centers were tertiary referral hospitals, such that patients might have been more likely to have severe disease.2
The development of distant metastases is known to be a serious problem, with melanoma being associated with a high mortality rate. In the present study, Cox's regression analysis showed that the median OS rate increased 17.7-fold without metastasis (P < 0.001). The median OS for patients with metastases was 7.8 months (95% CI, 6.1–9.5 months), which was similar to another large study of melanoma, in which the mean median survival time was 7–8 months for patients with metastases.26 The prognosis of MM depends on the site of metastasis.27 The mean OS rate was reported to be 4 months for liver, brain, and bone metastases, 8 months for lung metastases, and 12.5 months for gastrointestinal metastases.27 When classified according to metastasis site, the lowest OS was seen in the brain metastasis group. The present study found that MM patients with brain metastases had the lowest median OS, of only 2.79 months. The 5-year survival rate of patients with brain metastases was 0%, while in other clinical trials the estimated 5-year survival was 0%–5%.2829 In an autopsy study, 75% of patients who died of MM had brain metastases.30
In the current study, nodular histologic subtype, ulceration, and the Breslow thickness of the primary cutaneous melanoma were significantly associated with the development of metastasis. Homolak et al.11 retrospectively evaluated the association between various predictor variables and sentinel lymph node biopsy (SLNB) outcomes (positive SLNB and metastatic development) in 844 patients with primary cutaneous melanoma. They showed results consistent with those of the present study, where the main predictors of metastatic spread were Breslow thickness, nodular-type melanoma, and ulceration. A previous study in Australia also reported that the rapid growth of primary cutaneous melanomas was associated with tumor thickness and aggressive histologic features. NM grew four times faster than either SSM or LMM.31 Our study also showed that the Breslow thickness, development of metastasis and shorter OS were related to excess body weight. Obesity has been considered a risk factor for many types of cancer, including those of the endometrium, colon, esophagus, breast, kidney, gallbladder, pancreas, prostate, and thyroid.32 Epidemiological studies found a relationship between excess body weight and the risk of developing melanoma.3233 Retrospective European studies found that excess body weight was associated with increased Breslow thickness.3435 Interestingly, the present study found that excess body weight (BMI > 23) was associated with increased Breslow thickness in a Korean population. Potential mechanisms of melanoma growth due to obesity are as follows: 1) chronic hyperinsulinemia; 2) high plasma leptin level; 3) caveolin-1 expression; and 4) low serum vitamin D level.36 Excess body weight is associated with hyperinsulinemia, insulin resistance, and high insulin-like growth factor-1 levels, which lead to tumor growth via stimulation of angiogenesis and inhibition of apoptosis.37 Leptin, a cytokine secreted by adipose tissue, has direct mitogenic activity and may accelerate melanoma tumor growth.38 A previous study analyzed the overexpression of caveolin-1, a scaffolding protein involved in tumor proliferation, and fatty acid synthase, an enzyme implicated in the promotion of melanoma cells.39 BMI is inversely related to serum vitamin D, which is important in both the risk and prognosis of cutaneous melanoma.40
This study had limitations. The data were collected retrospectively and extracted from previous records; in some cases, the desired information, such as Breslow thickness and histopathologic subtype, was missing because diagnostic protocols and medical record formats differed among the hospitals.
 XML Download
XML Download