

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ectopic pregnancy (EP) is an important clinical emergency occurring in the initial stages of pregnancy. The incidence of EP with in vitro fertilization and embryo transfer (IVF/ET) has been reported to be between 2.0% and 3.5%.123 This is higher than the rate with natural conception, which has been reported as 1.5% to 2.0%.45 EP with IVF/ET can lead not only to complications such as severe bleeding, hypovolemic shock, or rupture of the uterus and salpinx, but also to psychological problems in infertile couples.
The pathophysiology of EP with IVF/ET is considered to be multifactorial. Although ET procedures can avoid tubal subcompetence related to EP in natural conception, embryo migration in the uterine cavity after ET before implantation could be the main risk factor for EP with IVF/ET. The possible factors related to EP with IVF/ET can be iatrogenic, embryonic, or maternal origin. The physician's ET technique could be one iatrogenic factor. Several studies have suggested that ultrasound-guided ET can lower the rate of EP.67 The competence of transferred embryos is one possible embryonic factor. Previous studies have demonstrated a difference in EP rate between Day 3 and Day 5 of embryo transfer8 and between fresh and thawed embryos.9 Uterine abnormality is one example of a maternal factor. Thin endometrium has been reported as a risk factor for EP with IVF/ET.1011 However, the relationship between ovarian factors and EP rate is largely unknown, even though ovarian reserve is an important factor in conception and its maintenance, owing to its role in supporting the hormonal environment during the embryonic implantation period.
This study aimed to compare the incidence of EP in IVF/ET cycles according to ovarian reserve. The authors analyzed the data from pregnancy cycles after IVF/ET procedures.
Go to : 
MATERIALS AND METHODS
Study subjects
A total of 430 IVF/ET cycles were analyzed from patients at two university hospital infertility clinics. Among these, 324 cycles were from Seoul National University Hospital and 106 cycles from Korea University Guro Hospital. The study included data from 2013 to 2017. All patients were β-human chorionic gonadotropin (hCG) positive at two weeks after the day of oocyte retrieval via controlled ovarian stimulation. For each cycle, we recorded the age of the patient, the duration of infertility, basal follicle stimulating hormone (FSH), anti-Müllerian hormone (AMH), days of controlled ovarian stimulation, numbers of retrieved oocytes and transferred embryos, and pregnancy outcomes. The measurements of FSH and AMH were performed according to the manufacturers' protocols. Automated chemiluminescence immunoassay system was used for the determination of FSH (ADVIA Centaur, Siemens Healthcare Diagnostics, Eschborn, Germany). The limit of sensitivity for FSH was 0.01 mIU/mL. AMH was measured using commercially available enzyme-linked immunosorbent assay kits (Ansh Labs, Webster, TX, USA). The limit of sensitivity for AMH was 0.01 ng/mL. Intra- and inter-assay variations were less than 5% and less than 8%, respectively, for all parameters. Patients with AMH lower than 1.0 ng/dL or basal FSH higher than 10 mIU/mL were classified into the decreased ovarian reserve (DOR) group, while the remaining patients were classified into the normal ovarian reserve (NOR) group. This study was approved by the Institutional Review Boards of Seoul National University Hospital (IRB No. H-1708-077-878) and Korea University Guro Hospital (IRB No. 2013GR0199).
Controlled ovarian stimulation, in vitro fertilization, and embryo transfer
Controlled ovarian stimulation was conducted as previously reported.12131415161718 For the GnRH agonist long protocol, the GnRH agonist triptorelin (Decapeptyl®, 0.1 mg/day; Ferring, Malmo, Sweden) was started during the mid-luteal phase of the previous cycle. After pituitary down-regulation, the triptorelin dose was reduced to 0.05 mg/day, and gonadotropin (Gonal-F®; Serono, Geneva, Switzerland) was added until either the leading follicle reached a mean diameter of 18 mm or two or more follicles reached a diameter of 17 mm. Treatment with 75–300 IU of gonadotropin, depending on the patients' previous or anticipated responses, was initiated on the third day of the menstrual cycle. The treatment was then individualized and adjusted in accordance with the response. For the GnRH antagonist multiple dose flexible protocol, 75–300 IU of gonadotropin was started on the third menstrual cycle day. A daily dose of the GnRH antagonist cetrorelix (Cetrotide®, 0.25 mg; Serono) was added once the leading follicle reached a diameter of 14 mm, and was continued until either the leading follicle reached a mean diameter of 18 mm or two or more follicles reached a diameter of 17 mm. For both protocols, recombinant hCG (Ovidrel ®, Serono) was administered subcutaneously 36 hours before ultrasonography-guided oocyte retrieval. Patients participating in fresh cycles underwent controlled ovarian hyperstimulation with a GnRH agonist or GnRH antagonist protocol, depending on the menstrual cycle day of the patient's visit.
The retrieved oocytes were cultured for 4 to 6 hours until insemination. Semen samples obtained via ejaculation on the morning of the oocyte retrieval day were liquefied at room temperature for 30 minutes and then centrifuged using SpermGrad (Vitrolife, Kungsbacka, Sweden) with two gradients (45%/90%) at 1500 rpm for 20 minutes. After removal of the supernatant, we layered 2 mL of the Universal IVF medium over the sperm pellet for centrifugation at 1000 rpm for 10 minutes. After washing and conducting the swim-up procedure, only the sperm pellet in the supernatant was aspirated and used for the insemination. Fertilization was determined by the presence of two pronuclei (2PN) using an inverted microscope on the first day after insemination. The zygotes with 2PN were cultured individually in microdrops containing 25 µL of growth medium, G-1™ v5 (Vitrolife) overlaid with 8 mL of mineral oil (Sigma, St. Louis, MO, USA) in Falcon 1007 culture dishes (Becton Dickinson Labware, Franklin Lakes, New Zealand). ET was performed 3 days after oocyte retrieval. The embryos were graded according to their morphologies and cleavage rates: they were graded from I to V based on the number and uniformity of the blastomeres and percentage of fragmentation. We defined good-quality embryos as those of morphological grades I–II; embryos with blastomeres of equal size with no cytoplasmic fragments or with minor cytoplasmic fragments or blebs and up to three embryos were selected and transferred into the uterus based upon the embryos' grade. The luteal phase was supported with daily 8% progesterone gel (Crinone®, Serono) initially for 14 days, starting on the day of oocyte retrieval.
Pregnancy outcome assessment
Serum β-hCG levels were checked on the 14th day after oocyte retrieval, and the cases with β-hCG levels over 10 mIU/mL were defined as positive β-hCG. The G-sac was assessed via vaginal ultrasonography on the 21st day after oocyte retrieval. Intrauterine pregnancy (IUP) was defined as the presence of a gestational sac in the uterine endometrial cavity with visible fetal heartbeat by transvaginal ultrasonography after 6–8 gestational weeks. EP was defined as a gestational sac in the extra-uterine cavity by transvaginal ultrasonography. The cases of combined pregnancy with coexistence of IUP and EP were excluded. Chemical pregnancy (CP) was defined as positive β-hCG without a visible gestational sac or as spontaneous abortion prior to visible fetal heartbeat.
Statistical analysis
Categorical variables are presented as frequencies and percentages. Continuous variables are presented as a mean±standard deviation and (median). Data were analyzed using Student's t-test, Mann-Whitney U test, chi-square test, and Fisher's exact test, where appropriate. To determine the association between background and treatment parameters and the rate of EP, we used univariate logistic regression utilizing the generalized estimating equations methodology. Multivariate logistic regression was then implemented to ascertain independent risk factors for pregnancy outcomes. The data were analyzed with SPSS software (SPSS Inc., Chicago, IL, USA). A p value <0.05 was considered to be statistically significant.
Go to :
RESULTS
Characteristics
Of the 430 IVF/ET cycles examined, 355 displayed NOR, and 75 cycles showed DOR. The DOR group had significantly older age, a longer duration of infertility, higher basal FSH, lower AMH, fewer ovarian stimulation days, a lower number of oocyte retrieved, and a higher rate of intracytoplasmic sperm injection (Table 1).
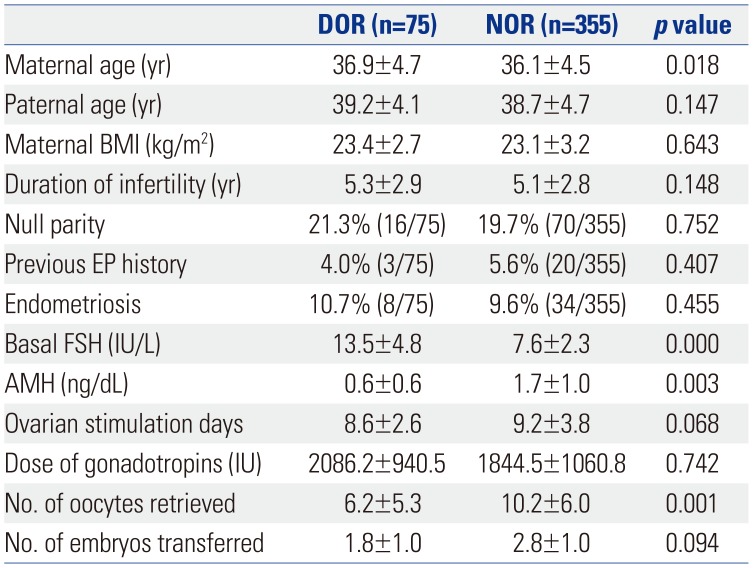
Table 1
Baseline Characteristics of Women Who Became Pregnant after IVF/ET according to Ovarian Reserve
![]()
Pregnancy outcome
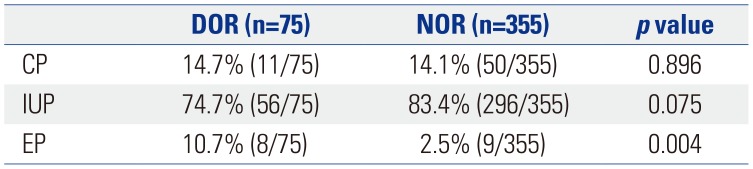
The overall IUP rate was 81.9% (352/430) (Table 2). On comparing IUP, the DOR group had a rate of 74.7% (56/75), whereas the NOR group had a rate of 83.4% (296/355), and the difference in percentages was not significant. The overall CP rate was 14.2% (61/430). For the group comparison of CP, the DOR group rate was 14.7% (11/75), the NOR group rate was 14.1% (50/355), and the difference in percentages was not significant. The overall EP rate was 4.0% (17/430). The DOR group had a significantly higher EP rate than that observed in the NOR group [10.7% (8/75) vs. 2.5% (9/355), p=0.004] (Fig. 1).
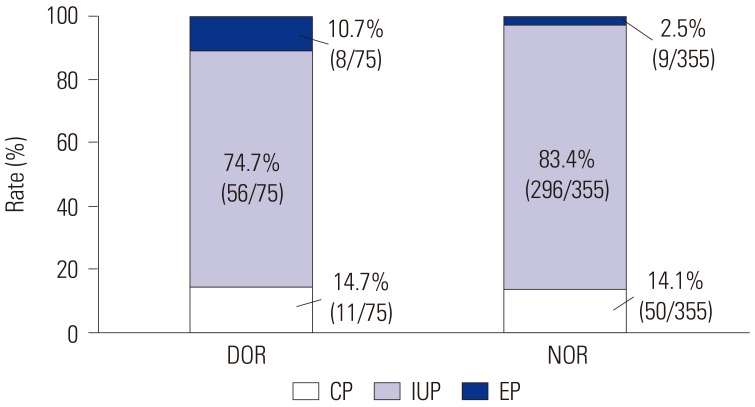 | Fig. 1Comparison of pregnancy outcomes between DOR and NOR. DOR, decreased ovarian reserve; NOR, normal ovarian reserve; CP, chemical pregnancy; IUP, intrauterine pregnancy; EP, ectopic pregnancy.
|
Univariate and multivariate analysis of variables for predicting EP
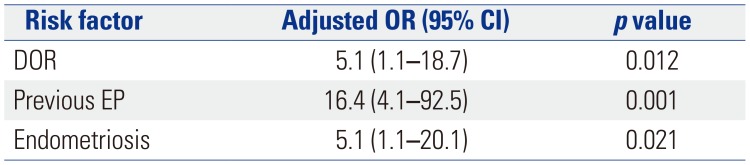
In the univariate analysis, there were no significant correlations between EP rate and maternal age, duration of infertility, maternal body mass index, parity, protocol of pituitary suppression, insemination methods, total gonadotropin dose, ovarian stimulation days, luteal support, endometrial thickness, number of oocytes retrieved, number of embryos transferred, or number of good quality embryos transferred. DOR [odds ratio (OR) 5.6, 95% confidence interval (CI) 1.4–9.6, p=0.011], previous EP history (OR 14.7, 95% CI 4.0–58.2, p<0.001) and endometriosis (OR 3.6, 95% CI 1.1–10.0, p=0.003) were associated with a higher EP incidence (Table 3). In the multivariate analysis with age, DOR showed a higher EP rate (adjusted OR 5.1, 95% CI 1.1–18.7, p=0.012), with previous EP history (adjusted OR 16.4, 95% CI 4.1–92.5, p=0.001) and endometriosis (adjusted OR 5.1, 95 % CI 1.1–20.1, p=0.021) (Table 4).
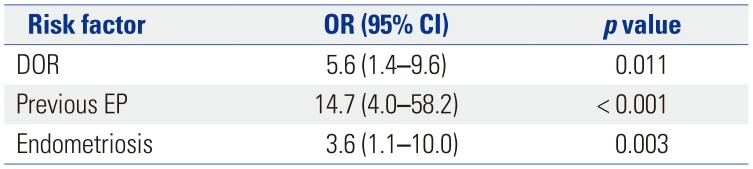
Table 3
The ORs of Variables for Predicting the Probability of EP after IVF/ET Using Univariate Logistic Regression
| Risk factor | OR (95% CI) | p value |
|---|---|---|
| DOR | 5.6 (1.4–9.6) | 0.011 |
| Previous EP | 14.7 (4.0–58.2) | < 0.001 |
| Endometriosis | 3.6 (1.1–10.0) | 0.003 |
![]()
Go to :
DISCUSSION
This study aimed to elucidate the correlation between ovarian reserve and the incidence of EP in IVF/ET cycles. We found that DOR may be a significant risk factor for EP in IVF/ET cycles. EP can be caused by many factors related to IVF/ET cycles, particularly a physician's technique during the ET procedures.19 As our study was undertaken with ultrasound-guided ET, our analysis could show the relative effect of ovarian reserve on EP incidence without ET technical bias.
Ovarian reserve is an important factor in assisted reproductive technology-induced conception. NOR can influence the success rate of pregnancy by IVF/ET even if it is not by itself a sufficient cause. Although a few surrogate markers have been suggested for ovarian reserve, basal FSH and AMH are recognized as clinically available and useful markers at present.2021 Even though AMH has been considered as the best surrogate marker of ovarian reserve, some reports have shown a discordance between AMH and antral follicle counts or ovarian response to stimulation.22 Thus, the present study utilized both AMH and basal FSH as markers of ovarian reserve. Consistent with our data, previous studies used basal FSH as the supporting factor for evaluating ovarian reserve.2324
Our results showed that DOR may be related with an increased risk of EP in IVF/ET cycles, in spite of a smaller number of transferred embryos. A previous study described an increased incidence of EP after IVF/ET in women with DOR, using only FSH level as the ovarian reserve marker, consistent with our results.25 In the present study, we combined AMH and basal FSH markers for more exact evaluation of ovarian reserve. The etiology of a higher EP rate in an IVF/ET cycle, compared to natural conception, remains unclear. Multiple factors in IVF/ET procedures could increase the risk of EP.26 Apart from IVF/ET procedures, the risk factors for EP in DOR group could have several origins. One possibility could be the effect of oocyte quality. Overall oocyte quality with DOR may be decreased, even with ovarian stimulation. Embryos fertilized from oocytes with decreased competence could have lower implantation capacity, resulting in implantation outside of the intrauterine endometrial cavity and causing EP. A second factor could be the sub-optimal hormonal environment in ovaries with decreased capacity. Endocrine support of the ovary for the endometrium to maintain optimal receptivity during embryo transfer could be a crucial variable in viable IUP.
We also found that a previous history of EP and endometriosis were independent risk factors for EP in IVF/ET, which was consistent with the findings from previous studies.27282930 These results suggest that careful monitoring is necessary during the IVF/ET cycles in women with these risk factors. Even though pregnancy was confirmed by positive serum β-hCG, these women could have an increased risk of EP, including heterotopic pregnancies in which there are combined intrauterine and ectopic gestational sacs.
Our study has a few limitations. First, this present retrospective study did not include the evaluation of suspected risk factors, such as previous tubal surgeries, previous pelvic inflammatory disease or sexual transmitted infection, smoking, and high volume of transfer media, due to the limited availability of a complete dataset. Further studies should be necessary for assessing the impact of these factors on incidence of EPs. Secondly, this observational study did not include subgroup analysis due to the small number of subjects with a low EP rate. Further studies with comparisons of the impacts of FSH and AMH should be necessary to distinguish the value of a single predictive marker for assessing the risk of EPs.
In conclusions, DOR was found to be related with increased rates of EP in IVF/ET cycles with controlled ovarian stimulation. Careful monitoring is necessary for pregnant women with DOR. In the future, possible underlying molecular mechanisms313233343536 in animal models37383940 should also be explored.
Go to :
 XML Download
XML Download