

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cataract surgery is one of the most commonly performed surgeries worldwide. Due to advancement in surgical techniques and materials, cataract surgery has become faster and safer.1 However, complications of posterior capsular tear, loss of endothelial cells, corneal stromal burn, postoperative endophthalmitis, and even retinal detachment still occur.23
Acute postoperative endophthalmitis (APE) is a rare, but devastating complication of cataract surgery. Its incidence is reported to be approximately 0.023% to 0.26%, depending on the report.45678 Commonly known risk factors for APE include older age, diabetes, posterior capsular tear and, although controversial, silicone intraocular lenses (IOLs), among others.789 To prevent APE, aseptic procedure, intracameral injection of cefuroxime, and intracameral moxifloxacin injection have been shown to be effective in several studies.8101112
There are many studies on APE, most of which have been conducted at several institutions, in the past, or from Western nationwide data.471213 The purpose of the present study was to evaluate the nationwide incidence of APE after cataract surgery in Koreans and to investigate risk factors related to the development of APE.
Go to : 
MATERIALS AND METHODS
National Health Insurance (NIH) is a universal health insurance system in South Korea.14 All Korean citizens are required to be registered with the NIH regardless of income, employment status, or marriage status.15 Health Insurance Review and Assessment Service (HIRA) is a government organization under the NIH that is responsible for reviewing medical bills, as well as conducting quality assessment of health care services.14 When a healthcare provider offers a medical service, they file a claim to the HIRA to obtain repayment for the service that they provided to patients.14 After July 2013, cataract surgery in Korea was assigned to the Diagnosis Related Group payment system; therefore, all cataract surgery claims must be filed to the HIRA for reimbursement and quality assessment. The HIRA's database is not open source. The data used in this study are available solely to the authors; researchers can apply to the HIRA after obtaining approval from the institutional review board of the institution. The Institutional Review Board of the Wonju Severance Christian Hospital approved this study (IRB number: CR317339), which adhered to the tenets of the Declaration of Helsinki.
We selected patients who had a cataract surgery recorded in the HIRA database between July 1, 2014, and June 31, 2017. For each patient, cataract surgery was identified by the code S5119 (phacoemulsification) or S5111 [intracapsular cataract extraction (ICCE)/extracapsular cataract extraction (ECCE)]. We also reviewed procedures based on IOL placement. The code for IOL included S5117 (IOL primary) and S5116 (IOL secondary). Patients who had a history of intraocular foreign body (H446, H447) were excluded. Patients with combined glaucoma surgery (S5043, S5047, S5049) or total vitrectomy (S5122, S5121) were also excluded. APE was defined when endophthalmitis criteria were found within 42 days following the date of cataract surgery. Endophthalmitis was defined as 1) diagnoses of endophthalmitis (H440, H441, H451, H59802) and treatment of vitrectomy (S5122, S5121); 2) diagnoses of endophthalmitis and antibiotic injection; or 3) antibiotic injection without diagnoses of endophthalmitis. The criteria for the use of antibiotics were based on injections of either vancomycin, amikacin, ceftriaxone, ceftazidime, or amphotericin B.
Posterior capsular tear was defined when anterior vitrectomy was performed. Usage of sutures was defined when a 10/0 nylon suture was used during surgery. Hypertension and diabetes were defined when diagnosis codes for hypertension (I10) and diabetes (E08-13) with antihypertensive medication or diabetes medications were found. Other medical conditions, such as heart failure, hepatic failure, dementia, stroke, etc., were included when a patient diagnosis code was present regardless of the medications.
Clinical setting was divided as primary, secondary, and tertiary hospitals. Because the information is protected, patient addresses could not be determined; thus, the address was evaluated based on the address of the hospital where the operation was performed. The address was divided into Seoul, metropolitan, and other areas. Income levels were classified according to whether the patients were covered under medical insurance or medical care, government expenditures, or patriots and veterans' affairs.
Statistical analysis was performed using independent two-sample t-test and chi-square (or Fisher's exact) test. For continuous variables, the data are expressed as the mean±standard deviation. For categorical variables, the data are expressed as counts and percentage. To assess potential risk factors for APE after cataract surgery, separate univariable logistic regression models were created with each covariate as an independent predictor and APE as the outcome. Covariates with p<0.1 in the univariable models were included in one multivariable model to assess for multivariable predictors of APE after cataract surgery. Results were reported as odds ratio (OR) and 95% confidence intervals (CI). All statistical analyses were performed with SAS Enterprise Guide 6.1 (SAS Institute Inc., Cary, NC, USA). All the tests were 2-sided, and p values <0.05 were considered significant.
Go to :
RESULTS
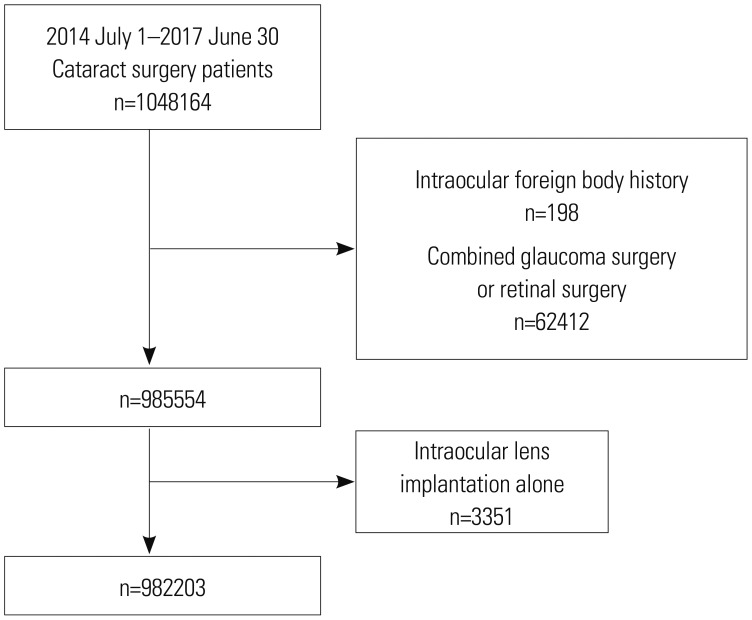
A flow diagram of the inclusion and exclusion of participants is provided in Fig. 1. A total of 1048164 patients were enrolled from July 2014 to June 2017. We excluded 198 patients due to intraocular foreign body history and 62412 patients with combined glaucoma and total vitrectomy surgery. Additionally, 3351 patients had IOL implantation alone. Finally, 1505103 cases of cataract surgery (982203 patients) were included in this study of APE development after cataract surgery.
In 953 eyes of 938 patients, APE developed with an overall incidence rate of 0.063%. The annual incidences of APE were 0.067% in 2014 (July 2014–June 2015), 0.064% in 2015 (July 2015–June 2016), and 0.058% in 2016 (July 2016–June 2017). Demographic factors of cataract patients are shown in Table 1. The mean age at which patients underwent cataract surgery was 69.10±10.41 years. Patients with APE were more likely to be male (p<0.001), have undergone surgery at a lower clinical setting (p=0.001), live in a rural region (p=0.002), have low income status (p<0.001), and have a medical history of hypertension (p<0.001), diabetes (p<0.001), heart disease (p=0.038), hepatic disease (including chronic hepatitis) (p=0.040), renal failure (p<0.001), or dementia (p=0.006).
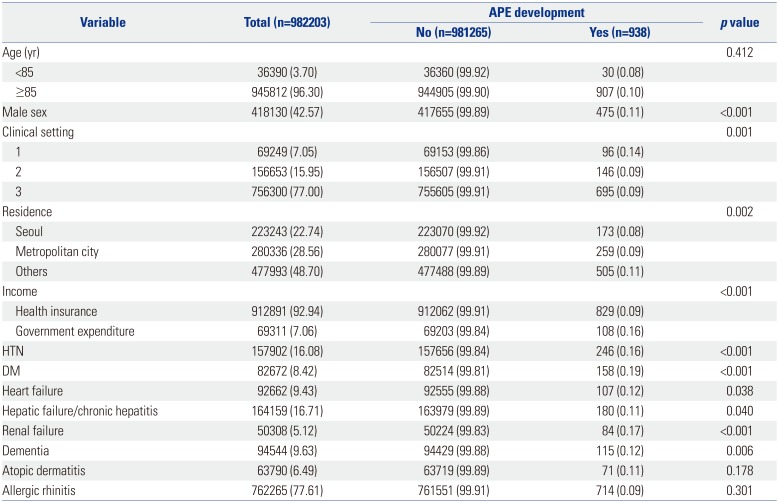
Table 1
Demographic and Clinical Characteristics of the Study Patients
![]()
Results of case-wise data examination and univariable regression analysis are shown in Table 2. With respect to surgical aspects, patients with APE received more sutures (p<0.001) and anterior vitrectomy (p<0.001).
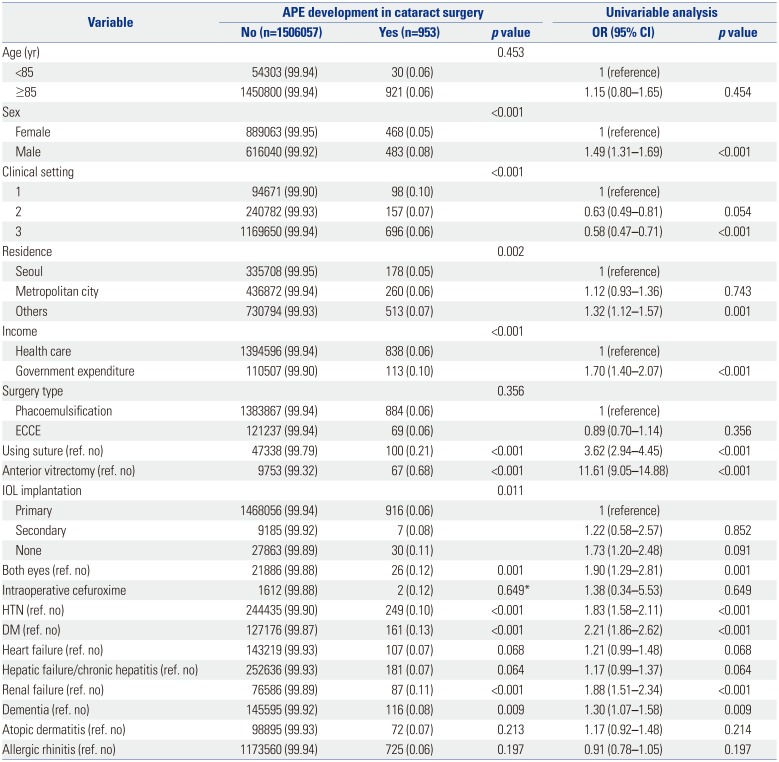
Table 2
Cataract Cases and Univariable Regression Analysis with APE Development
![]()
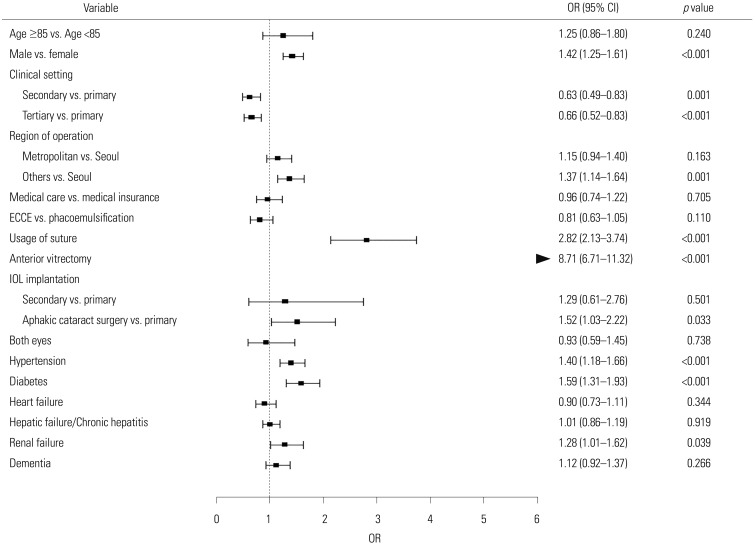
Results of case-wise multivariable regression analysis are shown in Fig. 2. After adjusting for possible confounding factors, male sex (OR 1.42; 95% CI 1.25–1.61; p<0.001), primary clinical setting, operations performed in non-major cities, usage of sutures (OR 2.82; 95%CI 2.13–3.74; p<0.001), anterior vitrectomy (OR 8.71; 95% CI 6.71–11.32; p<0.001), aphakic cataract surgery (OR 1.52; 95% CI 1.03–2.22; p=0.033), hypertension (OR 1.40; 95% CI 1.18–1.66; p<0.001), diabetes (OR 1.59; 95% CI 1.31–1.93; p<0.001), and chronic renal failure (OR 1.28; 95% CI 1.01–1.62; p=0.039) were found to be associated with APE development.
There were 3351 eyes from 3351 patients with IOL implantation without phacoemulsification or ECCE/ICCE. Primary IOL implant was performed in 690 eyes (690 patients), and secondary IOL implant was performed in 2661 eyes (2661 patients). None of the patients with IOL implantation only developed APE.
Go to :
DISCUSSION
Demand for cataract surgery is increasing due to aging populations, and complications after cataract surgery are a growing concern. Therefore, safer, faster, and cheaper cataract surgery that avoids possible risk factors is crucial. Also, in terms of quality management, continuous monitoring of complications of cataract surgery is needed. The overall APE rate in Korea from July 2012 to Jun 2014 was 0.063%, which is consistent with previous reports.
Preoperative immune status is important in APE development. 1617 In the present study, hypertension, diabetes, and chronic renal failure were associated with APE development. Diabetes is a well-known risk factor for APE.789 However, studies reporting the relationship between hypertension and APE development were difficult to find. Hypertension could be a confounding factor for APE development; however, there is a possibility that hypertension itself could be a risk factor for APE, as an association between hypertension and immune system dysfunction has been shown in several studies.1819 Further studies are needed to determine whether hypertension is a direct cause of endophthalmitis. Chronic renal failure also affects immune function and renders the patient prone to various infections, such as APE.20 However, the authors were unable to find other large studies reporting associations between APE and chronic renal failure.
In the present study, clinical settings and region of surgery were also associated with APE development. Secondary and tertiary referral hospitals had lower incidences of APE development. Interestingly only 94671 (6.3%) of all cataract surgeries was performed at primary clinics. According to the HIRA, there are 1561 ophthalmology clinics, 78 secondary hospitals, and 173 tertiary referral centers registered.21 The authors cautiously suspect that, since only 6.3% of cataract surgeries are performed in private clinics, which account for more than 85% of the total number of ophthalmologic hospitals, this shows that cataract surgery is not performed frequently, so it may be difficult to maintain sterilization of facilities and instruments. Further study and education should be performed regarding this matter. Patients who received cataract surgery in non-major cities had higher APE development rates. This suggests that environmental factors also affect APE development.
Whether ECCE or phacoemulsification poses a higher risk of APE is controversial. Theoretically, ECCE would pose a higher risk due to the larger surgical incision and inflow of fluid from the ocular surface during surgery. While some reports suggest increased risk in ECCE,22 Wong and Chee4 reported that phacoemulsification had a three-fold higher risk of developing APE, although the reason was unclear. In the present study, ECCE exhibited a reduced risk, although the difference was not statistically significant (OR 0.81; p=0.110).
Herein, we found anterior vitrectomy to be strongly associated with APE development (OR 8.71; p<0.001). Posterior capsular tear is a common intraoperative complication during cataract surgery.23 Many reports show an increased risk of developing APE in patients with posterior capsular tear.7 When the posterior capsule is ruptured, a longer duration of surgery is needed, and delayed bacterial elimination from the vitreous is assumed to be a reason for increased APE development.4 Anterior vitrectomy was the most important risk factor for the occurrence of endophthalmitis, and close observation is needed both during and after surgery for possible APE development.
In this study, leaving the patient aphakic was associated with higher APE risk (OR 1.52; p=0.033). Aphakia after cataract surgery is usually unplanned and primarily caused by a surgical complication:24 the authors suspect it is mainly from intraoperative complications. In the prevention thereof, intracameral cefuroxime was found to be effective in several studies.81011 However, the prophylactic effect of cefuroxime was not statistically significant in this study.
The most interesting finding in the present study was that usage of sutures increased the risk of developing APE. The incidence of APE had been on a continuous decrease until 1992, the year in which the self-sealing clear corneal incision was introduced. After 1992, an increased incidence of APE was described.2526 Widespread use of clear corneal incisions was thought to be one of the reasons for increased APE development.26 While clear corneal incision offers a shorter procedure time, less astigmatism, and faster visual recovery, compared with a scleral tunnel procedure,25 wound integrity and fluid influx from self-sealing clear corneal incisions have been issues for a long time.2728 Also, whether suturing of the corneal wound in cataract surgery improves wound integrity has been debated.2930 The role of sutures in postoperative endophthalmitis is controversial. Lee, et al.31 reported suture-related delayed postoperative endophthalmitis. However, Thomas, et al.32 suggested that suturing decreased the rate of APE. In the present study, use of sutures was associated with increased APE even after correction for ECCE and ICCE in multivariable logistic regression. Using sutures during surgery could mean several things. Sutures could be used to improve wound stability in non-complicated surgery or it could also be related to wider incisions, complications, such as corneal stromal burn, prolonged and excessive manipulations, and sutured scleral incisions, etc., which could also have an effect on APE development. Although the suture itself could be a focus for infections, concluding that suturing is related to APE will require further evaluation.
There are several limitations to this study. First, error or loss in coding is possible.33 If complications, such as dropped nucleus, occurred and a patient received a total vitrectomy, the patient is no longer included in the diagnosis-related groups. These patients were impossible to distinguish from planned phaco-vitrectomy. Therefore, some patients may have been overly excluded in the present study. Also, since hospitals claim a reimbursement from the HIRA after the procedure, loss to claim used materials could be possible. In addition, the database does not clarify the route of antibiotics administration nor laterality of surgery, leading to overestimation of APE development. Second, inflammatory disease, such as toxic anterior segment syndrome, could be coded as endophthalmitis, which could be confused as APE. Fifteen patients were suspected to have bilateral APE. Although it is not impossible to develop bilateral APE, authors suspect that if APE occurred in the first operation, it is likely that the surgeon may have over treated inflammatory reactions after fellow eye surgery. Therefore, there is a possibility that the incidence of APE is overestimated. Third, the period of observation time was short. The authors reviewed only 3 years of cataract surgeries due to size limitations of the HIRA database, and trends in APE development could not be evaluated. Fourth, information regarding the type and placement of incision was not available, and clear corneal incision and temporal placement are considered risk factors for developing APE.26 Fifth, the IOL material is unknown, since previous studies have suggested that certain types of IOL may be implicated in APE development.34 However, the material of the IOL could not be identified in this study. Another limitation is that this study did not clearly identify the residence of the patients. If the patient is operated outside their area of residence, there may be an error in the evaluation. Despite these limitations, this study is the first nationwide evaluation of APE development in Korea and has the advantage of evaluating variables that were not identified in other studies.
The overall rate of APE was 0.063% in South Korea form July 2014 to June 2017. Preoperative risk factors for APE were male sex, hypertension, diabetes, and chronic renal failure. Intraoperative risk factors were usage of sutures, anterior vitrectomy, and aphakic cataract surgeries. Operations performed in non-major cities in a primary clinical setting were also associated with increased development of APE. Additional research is needed to determine the relationship of newly found risk factors, such as hypertension, primary clinical setting, chronic renal failure, and usage of sutures, with APE development. No APE developed after IOL implantation only without cataract extractions.
Go to :
 XML Download
XML Download