

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sperm DNA integrity is essential for precise genetic transmission to a developing embryo and has been proposed as a biomarker for healthy sperm. Sperm DNA fragmentation (SDF) can be induced during chromatin remodeling in spermiogenesis, especially replacement of histone proteins by protamine.1 Other causes of SDF included defective apoptosis, excessive reactive oxygen species, and environmental toxins.2 Although debatable, it has been reported that high SDF levels reduce clinical pregnancy rates34567 and increase miscarriage rates in in vitro fertilization (IVF) cycles.89
Obtaining good-quality embryos is fundamental and leads to success in assisted reproduction. DNA-defective sperm in fertilization could potentially decrease embryo quality. However, evidence for this is insufficient. There are large discrepancies between published studies regarding the impact of SDF on embryo quality.10111213141516 Some researchers have suggested that there is a negative correlation between SDF and embryo quality,10111213 while others have found no association between them.141516
In the aforementioned studies, SDF was measured by different methods: terminal deoxynucleotidyl transferase dUTP nick-end labeling (TUNEL) assay,1114 sperm chromatin structure assay,1215 single cell gel electrophoresis (Comet) assay,1013 or sperm chromatin dispersion (SCD) test.16 Among various methodologies, SCD test has been reported to be simple, less expensive, and highly reproducible.17
In previous studies, the majority of researchers selected women with various ovarian responses to gonadotropin, including poor responders. However, it appears to be reasonable to include normal responders only because poor responders are less likely to yield top-quality or good-quality embryos regardless of SDF. Two previous reports included normal responders only,1114 and only Avendaño, et al.11 found a negative association between SDF level as measured by TUNEL assay and embryo quality.
To our knowledge, this is the first study to analyze correlations between SDF as measured by SCD test and embryo quality only in normal responders. The present study investigated the association of SDF level with three embryo formation rates at day 3 [per fertilized oocyte with two pronuclei (2PN)] in normal responder women.
Go to : 
MATERIALS AND METHODS
Study population
Fifty-three consecutive fresh IVF/intracytoplasmic sperm injection (ICSI) cycles were selected. All cycles were performed between 2014 and 2017 at Seoul National University Bundang Hospital. IVF/ICSI cycles were included if they were normal responders (i.e., 4 to 14 mature oocytes were retrieved) and at least one 2PN zygote was obtained. The median ages of women and their male partners were 35.0 (interquartile range: 32.0–39.5) and 38.0 (interquartile range: 35.0–44.0) years, respectively. Indications for IVF were unexplained (n=22), tubal (n=12), male (n=8), endometriosis (n=5), uterine (n=4), polycystic ovary syndrome (n=1), and old age (n=1). This retrospective study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (IRB No. B-1806-474-106).
Ovarian stimulation and oocyte retrieval
Ovarian stimulation was performed with recombinant folliclestimulating hormone (FSH) (Gonal-F, Merck-Serono, Darmstadt, Germany; or Follitrope, LG Chem, Seoul, Korea), highly purified human menopausal gonadotrophin (Menopur, Ferring, Saint-Prex, Switzerland), or recombinant FSH/luteinizing hormone (Pergoveris, Merck-Serono). The dose of gonadotropin was adjusted individually based on follicular response monitored by transvaginal ultrasonography. Pituitary downregulation was achieved with a flexible GnRH antagonist protocol (Cetrotide 0.25 mg/d, Merck-Serono) (n=49) or a midluteal long protocol using GnRH agonist (Decapeptyl 0.1 mg/d, Ferring) (n=3). Pituitary down-regulation was not employed in a single cycle. When the leading follicle reached a mean diameter of ≥18 mm or two follicles reached a mean diameter of ≥17 mm, 250 µg of recombinant hCG (Ovidrel, Merck-Serono) was injected subcutaneously. Oocyte retrieval was performed at 35–36 hours after hCG injection. If immature oocytes were retrieved, they were cultured in in vitro maturation media. Once matured, they were counted as mature oocytes.
Measurement of SDF, sperm preparation, and insemination
Semen samples were collected on the day of oocyte retrieval. Standard sperm quality was assessed according to the World Health Organization guidelines (5th edition, 2010).18 Normal sperm was defined as semen volume ≥1.5 mL, concentration ≥15×106/mL, motility ≥40%, and a percentage of normal form using strict criteria ≥4%.
After one washing, SDF was measured by SCD test using Halosperm assay (Halotech DNA, Madrid, Spain), as previously described in our institutional protocol.19 Briefly, an aliquot of the semen sample was diluted with Ham's F-10 medium (Sage, Trumbull, CT, USA) to 5×106/mL to 10×106/mL. Agarose gel from the kit was placed in a water bath at 90–100℃ for 5 minutes and then at 37℃ for 5 minutes. This was followed by adding and mixing 25 µL of semen in a marked Eppendorf test tube. The mixture of 15 µL was placed on a super-coated slide and covered with a coverslip. Slides were then placed in a refrigerator at 4℃ for 5 minutes to create a microgel with embedded sperm cells. After obtaining slides from the refrigerator, coverslips were gently removed, followed by immersing slides in acid denaturation solution (80 µL in 10 mL of distilled water) for 7 minutes. These slides were then immersed in a lysis solution from the kit and incubated for 25 minutes. After washing with distilled water, slides were dehydrated in increasing concentrations of ethanol (70, 90, and 100%) for 2 minutes and then air-dried. The slides were stained with Diff-quick solution I and II (7 minutes for each), rinsed with distilled water, and air-dried at room temperature.
Each slide was examined under a light microscopy at ×100 magnification. At least 300 sperms were scored. Each sperm was classified as large halo, medium halo, small halo, no halo, or degraded. A large halo meant that the halo width was similar to or higher than the minor diameter of the core. A medium halo meant that the halo size was between large halo and small halo. A small halo meant that the halo width was similar to or smaller than one-third of the minor diameter of the core. Degraded sperm was similar to sperm with no halo but weakly or irregularly stained. SDF level (%) was calculated as (the number of small halo+no halo+degraded form)/total sperm cell counted.
The remaining semen samples were processed by a discontinuous gradient (Sydney IVF Sperm Gradient, COOK Medial, Brisbane, Australia) as described in the kit instructions and our institutional protocol.819 Mature oocytes were inseminated by conventional methods (18 cycles), ICSI (29 cycles), or split insemination (6 cycles). Fertilization was confirmed by observing 2PN zygotes on day 1 after insemination.
Embryo quality assessment
Embryo quality was evaluated by morphological criteria based on the degree of fragmentation and the regularity of blastomeres on day 3 after insemination. Embryos were graded as follows: grade A, 0% anucleate fragments, regularity of blastomeres, no apparent morphological abnormality; grade B, <20% anucleate fragments, regularity of blastomeres, no apparent morphological abnormality; grade C, 20–50% anucleate fragments, irregularity of blastomeres, no apparent morphological abnormality; and grade D, >50% anucleate fragments, irregularity of blastomeres, and apparent morphological abnormalities.20 The top-quality embryo was defined if they showed seven cells or more with grade A. Day 3 embryo formation rate was always calculated per 2PN zygote. In the present study, three embryo formation rates were employed: top-quality embryo formation rate, grade A embryo formation rate, and grade A or B embryo formation rate.
Embryo transfer and IVF outcome measures
The embryos were transferred at 3 days (n=37) or 5 days (n=10) after oocyte retrieval. Serum hCG levels were determined at 14 days after oocyte retrieval. Those with a positive hCG result underwent transvaginal ultrasound to confirm an intrauterine pregnancy. Clinical pregnancy was defined as the presence of one or more gestational sacs with a fetal heart beat.
Statistical analysis
All statistical analyses were performed using SPSS 22 (IBM Corp., Armonk, NY, USA). Spearman correlation rank test was used to analyze the associations of SDF levels with standard sperm quality and three embryo formation rates. A receiver operating characteristics (ROC) curve analysis was used to determine the specific cut-off value of SDF to predict specific embryo formation rate. Mann-Whitney U test was used to compare parameters between groups. Proportions between groups were compared using Pearson's chi-square test or Fisher's exact test if the observed cell number was less than five. All p values <0.05 were considered significant.
Go to :
RESULTS
The interquartile range of SDF levels was 16.0% to 44.5% (median: 28.0%). SDF levels showed a positive linear correlation with the male's age (r=0.307, p=0.025) and a negative linear correlation with sperm motility (r=−0.491, p<0.0001). The estimated equation was as follows: SDF level (%) = 16.786 + [0.945×husband's age (yr)] − [0.465×motility (%)] (p<0.0001). SDF levels had no relationship with sperm concentration (r=−0.07, p=0.614) or the percentage of normal form (r=−0.08, p=0.590).
The median value of top-quality embryo formation was 33.3% (interquartile range: 14.3–58.6%): grade A embryo formation rate was 33.3% (interquartile range: 17.4–61.3%), and grade A or B embryo formation rate was 75.0% (interquartile range: 50–100%).
SDF levels exhibited a negative relationship with top-quality embryo formation (r=−0.249, p=0.073) and grade A embryo formation (r=−0.240, p=0.083), but did not reach statistical significance. SDF levels had no association with grade A or B embryo formation rate (r=−0.143, p=0.309).
ROC curve analysis revealed that the cut-off value of SDF was <30.7% for prediction of a top-quality or grade A embryo formation rate >70% with statistical significance (Table 1). This cut-off value had good sensitivity and an excellent negative predicted value. Among individuals with SDF <30.7%, the median top-quality embryo formation rate was significantly higher than that among individuals with SDF ≥30.7% (38.1% vs. 20.0%, p=0.038) (Table 2). Among individuals with SDF <30.7%, the median grade A embryo formation rate was also significantly higher than that among individuals with SDF ≥30.7% (50.0% vs. 25.0%, p=0.017). Among those with SDF <30.7%, the clinical pregnancy rate was higher than that in subjects with SDF ≥30.7%, although the difference did not show statistical significance.
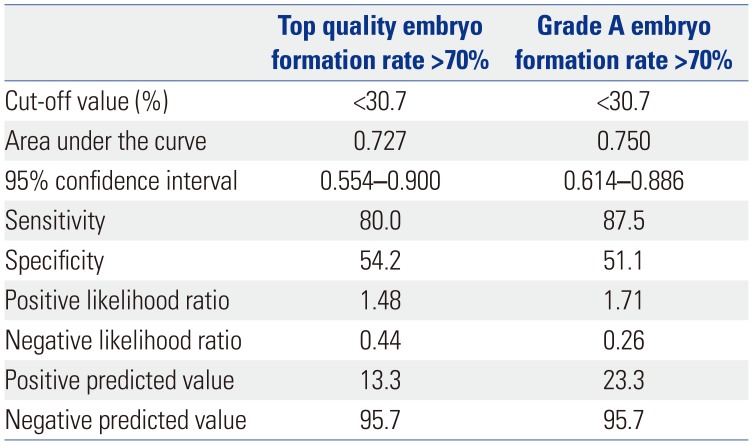
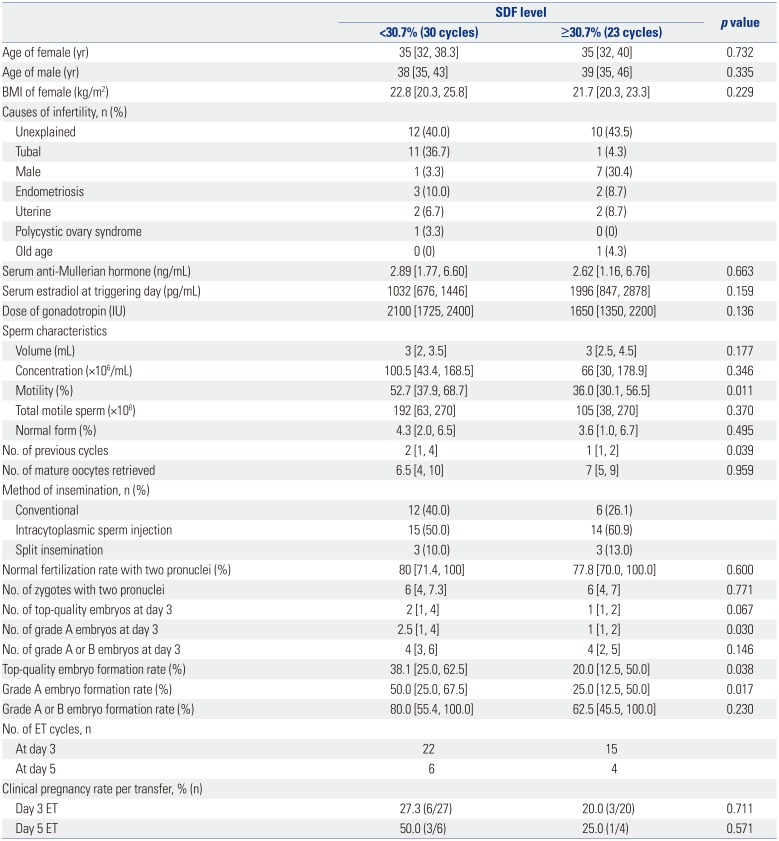
Table 1
Cut-Off Value of Sperm DNA Fragmentation to Predict Top-Quality or Grade A Embryo Formation Rate >70% in Normal Responders
![]()
Table 2
Comparison of Cycle Characteristics according to the Cut-Off Value of SDF in Normal Responders
![]()
Go to :
DISCUSSION
In the present study, SDF levels exhibited a negative impact with top-quality or grade A embryo formation rate in normal responder women. The cut-off value of SDF <30.7% could predict top-quality or grade A embryo formation rate >70% with a statistical significance. Between groups with SDF <30.7% and SDF ≥30.7%, top-quality or grade A embryo formation rate was significantly different.
Analysis of sperm quality is based on standardized protocols recommended by the World Health Organization in 2010,18 although the conventional semen parameters do not reliably predict the outcomes of assisted reproductive technology.21 Male factor infertility is diagnosed by abnormal semen parameters, but could be present even if the semen analysis is normal. Agarwal and Allamaneni22 reported that 15% of men with infertility problems were classified with normozoospermia. Therefore, researchers have investigated other markers to predict male infertility in a more clinically useful manner. An increasing number of studies suggest that SDF could be a potential biomarker of semen quality.23 Moreover, it is well established that the completion of fertilization process and subsequent embryo development depends, in part, on the integrity of the sperm DNA.16
In order to investigate exactly how SDF affects embryo quality, it is appropriate to control the number of retrieved oocytes. In a recent meta-analysis, there was a strong positive association between the number of oocytes collected and the number of top- or good-quality embryos at day 2/3 (r=0.791, p<0.001).24 Considering the quantitative aspects, poor responders with few oocytes have a lower chance to form top-quality or good-quality embryos regardless of SDF. In our study, we selected only normal responders for more convincing evidence that SDF deteriorates embryo quality.
It has been reported that oocytes have the capability to repair damaged DNA of sperm in a murine model.2526 Although oocytes can repair damaged DNA of sperm, it seems to have a threshold. Beyond such threshold, damaged sperm DNA appears unrepairable1227 and may negatively impact embryos. It was traditionally accepted that the male genome becomes activated at the later developmental stage of embryogenesis. Interestingly, high SDF levels could influence early embryo development up to the 4-cell stage, in which the paternal genome is thought to be inactive.13 SDF may activate additional DNA repair pathways, and the embryo development could be delayed, resulting in poor embryo quality.28
In the aforementioned studies that reported a negative correlation between SDF and embryo quality,10111213 there were no definite inclusion criteria regarding ovarian responses, except the study conducted by Avendaño, et al.,11 which included women with more than four oocytes collected. Avendaño, et al.11 evaluated embryo quality using mean embryo score, which may not accurately reflect the embryo quality because it uses mean values and because it is difficult to score the morula or embryo with compaction at day 3. Even if embryo formation rate was employed,101213 using the total number of embryos for the denominator could be affected by the number of oocytes. It seems more suitable to use normally fertilized oocytes with 2PN for the denominator.
In this study, we found that the cut-off value of SDF was <30.7% to predict a top-quality or grade A embryo formation rate >70%. Our cut-off value of SDF was similar to that of a previous report, in which a cut-off value of SDF <27% was significantly associated with higher top-quality embryo formation rates at day 3.12 Interestingly, cut-off values of SDF measured with SCD test to obtain a high pregnancy rate have been reported to be 30–35%.29
The main strengths of this study were including only normal responders, using 2PN for the denominator of embryo formation rate, and determining SDF in the actual sperm sample used for IVF. The limitations of this study were the retrospective nature of the work. We could not analyze the study population by dividing it into conventional IVF or ICSI because of the small sample size. Further studies with large sample sizes are required to exclude other possible confounding factors, such as a women's age.
In conclusion, our results indicated that SDF levels <30.7% could be a good predictor to achieve a top-quality or grade A embryo formation rate >70%. Our results suggest a paternal effect on embryo quality in IVF cycles even in normal responder women.
Go to :
 XML Download
XML Download