

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since Leonard Noon and John Freeman reported the effect of prophylactic inoculation of grass pollen in hay fever patients in 1911, allergen-specific immunotherapy (AIT) has been used to treat allergic diseases in clinical practice for more than 100 years.1 It is well known that AIT can reduce symptoms and medication scores,23 alter the natural course of allergic diseases45 and prevent disease progression from allergic rhinitis to asthma67 as well as new sensitization.89 However, relatively long treatment duration, high cost, and frequent hyperreactivity reactions, including anaphylaxis, can be hurdles to choose AIT.
Although AIT is a well-established, effective therapeutic modality for treating allergic disease, the use of AIT is not widely used in most countries. A minor portion (2–9%) of allergic patients in the United States have been treated with AIT according to previous reports,1011 and only 36.2% of patients recommended AIT by their doctors doctors eventually underwent AIT.12 This seems to suggest a lack of education and understanding of AIT among both patients and doctors. Demoly, et al.13 reported that about 50% of patients recognized AIT as a therapeutic option, of whom 14% had negative opinion thereof. However, once AIT is started, approximately 60% of patients are satisfied with it. Among doctors, less than 50% of general practitioners were aware of the exact placement of AIT, and almost all of them wanted detail information about AIT in Italy.1415 Several aspects of AIT in controlled studies have been extensively investigated, including clinical efficacy,161718 tolerability,19 and effects on health-related quality of life (QoL);202122 however, a few studies addressing patient and physician perspectives on AIT have been published, especially in Korea.
Accordingly, this multicenter cross-sectional study aimed to explore patient and physician satisfaction with the efficacy, safety, and economic parameters of AIT through a questionnaire survey: this survey addressed symptom changes, medication use, economic aspects, side effects, and satisfaction rate among allergic patients, as well as changes in disease severity based on international guidelines.
MATERIALS AND METHODS
Patients
A total of 273 patients with allergic rhinitis, allergic conjunctivitis, allergic asthma, and/or atopic dermatitis were recruited from 10 secondary or tertiary hospitals around Korea between April 2017 and July 2018 in this study. Inclusion criteria were patients who gave written informed consent and received AIT to house dust mites, tree/grass/weed pollen, animal dander, or fungi for at least 1 year, regardless of AIT methods and manufacturing companies. Of the 273 patients, only six received sublingual immunotherapy (SLIT) for their allergic disease and were excluded from the study. The study protocol was approved by the institutional review boards of each hospital (AJIRB-MED-SUR-17-159, Ajou University Hospital).
Survey
The questionnaire was developed by an expert panel from the Korean Academy of Asthma, Allergy and Clinical Immunology (KAAACI) on the basis of experience and literature review. After a literature search for perspectives of AIT, workgroup members made a draft of this study. For each question, responses and comments from the workgroup members were collected and synthesized into a draft manuscript that was recirculated until consensus was reached. The questionnaire consisted of 15 items for patients and 10 items for physicians. The patient questionnaire included demographics, perception, expectation, side effects, and satisfaction on a 5-point Likert scale (much improved/improved/no difference/aggravated/much aggravated; excellent/good/fair/poor/very poor; very favorable/favorable/neutral/unfavorable/very unfavorable). The physician questionnaire included allergic status, AIT products, and changes in disease severity based on international guidelines. The questionnaire items for patients and physicians are presented in the Supplementary Materials (only online).
Statistical analysis
All analyses were carried out using SPSS 22.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to analyze demographic and clinical data obtained from the patients' and physicians' responses to the questionnaire. Continuous variables are expressed as means±SD and categorical variables are expressed as percentage. The clinical data were compared among age groups using the chi-square test or McNemar's test. All p values <0.05 were considered statistically significant.
RESULTS
General characteristics
A total of 267 patients who received subcutaneous immunotherapy were analyzed in this study. Enrolled patients consisted of 161 (60.3%) patients treated at the Department of Internal Medicine and 106 (39.7%) treated at the Department of Pediatrics. The mean age was 25.6±15.4 years, and 133 (49.8%) were male. AIT was most frequently prescribed to patients in their 10s; it was rarely prescribed to patients in their 60s. In addition, 79.0% of patients had a family history of allergic disease, and 10.2% of patients had a previous AIT history. Most patients (69.6%) had heard about AIT by general hospital physicians; however, only 5.9% of allergic patients had heard about AIT by general practitioners.
Allergic rhinitis (91.4%) was the most common disease to be treated by AIT, followed by asthma (42.7%) and atopic dermatitis (20.2%). Their mean duration of AIT was 27.3±15.0 months. Moreover, 91.6% of patients reported that they had good adherence to AIT, and these data were correlated with that of the doctors' views (kappa agreement=0.356, p<0.001). Detailed data on the patient characteristics and immunotherapy-related factors are shown in Table 1.
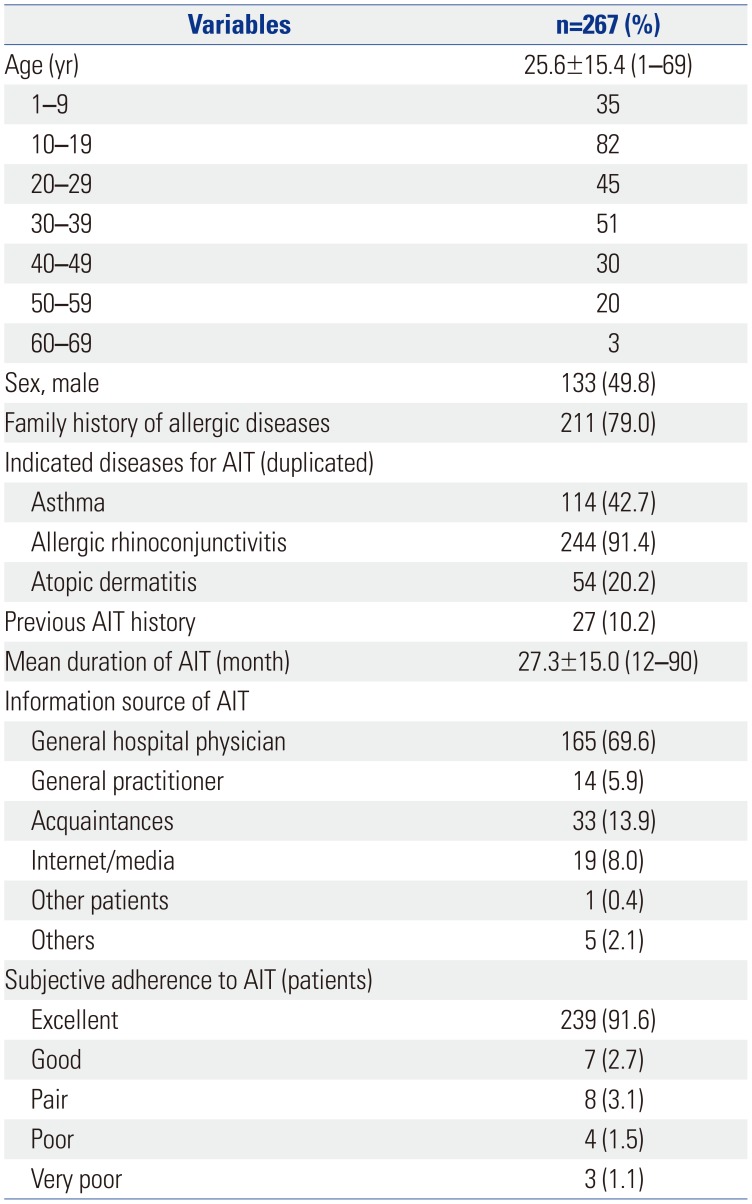
Table 1
Demographic- and Immunotherapy-Related Characteristics of Patients in This Study
![]()
Changes in symptoms and disease severity after AIT
After more than 1 year AIT of treatment for asthma, most patients reported a better than ‘improved’ state in their daytime symptoms (91.0%), nighttime symptoms (92.8%), short-acting beta-agonist use (82.4%), asthma attack (87.2%), and QoL (90.5%) (Fig. 1A). Physician indicated in the questionnaire on allergy symptoms and medication use that disease severity dramatically decreased after AIT for asthma (intermittent from 7.9% to 63.4%, mild persistent from 38.6% to 28.7%, moderate persistent from 46.5% to from 6.9%, and severe persistent 6.9% to 1.0%, p<0.001) (Fig. 1C).
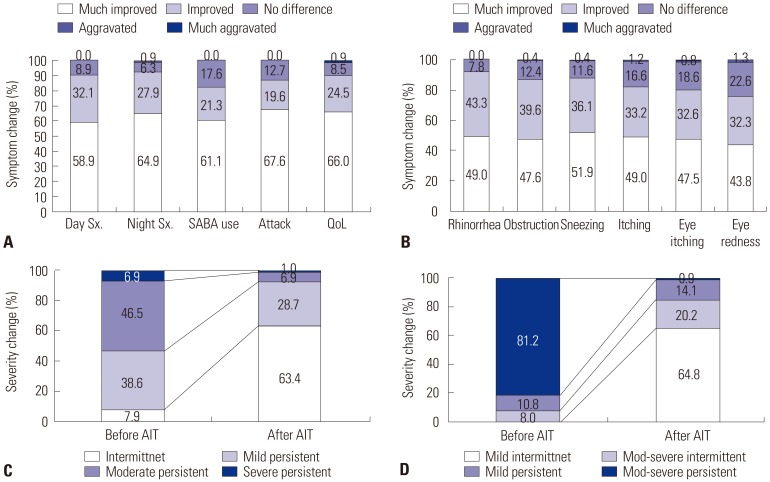
Fig. 1
Changes in allergy symptom and severity after AIT. (A) Symptom changes in patients with asthma. (B) Symptom changes in patients with allergic rhinitis. (C) Asthma severity change based on the GINA guideline. (D) Allergic rhinitis severity change based on the ARIA guideline. AIT, allergen-specific immunotherapy; SABA, short-acting bata-agonist; QoL, quality of life.
![]()
For patients with rhinitis, there were improvements in symptoms, including rhinorrhea (92.3%), nasal obstruction (87.2%), sneezing (88.0%), itching (82.2%), eye itching (80.1%), and eye redness (76.1%) (Fig. 1B), as well as disease severity (mild intermittent from 0% to 64.8%, moderate-severe intermittent from 8% to 20.2%, mild persistent from 10.8% to 14.1%, and moderate-severe persistent from 81.2% to 0.9%; p<0.001), (Fig. 1D).
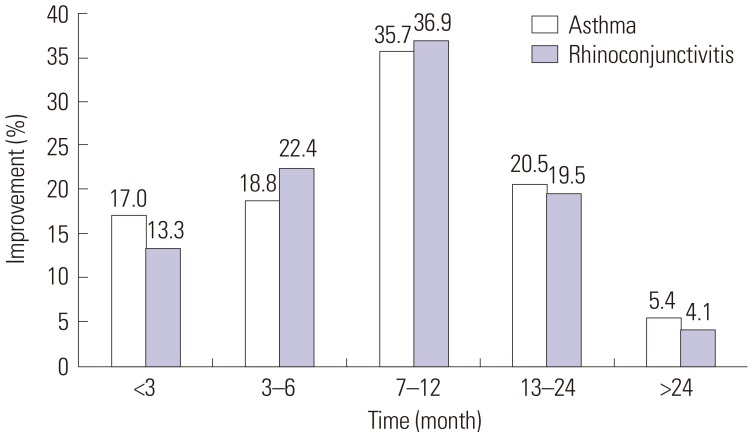
Interestingly, about 15% of patients reported symptom improvements within 3 months after starting AIT, and almost 3 out of 4 patients reported that their symptoms were diminished within 1 year after starting AIT (Fig. 2). However, whether patients had only one of rhinitis or asthma or both diseases did not affect satisfaction with AIT among patients and their physicians.
Changes in medication use after AIT
Prescription rates were evaluated for individual drugs in the questionnaire for physicians. Before starting AIT, ICS, beta-agonists, LTRA, and theophylline were administered to 79.8, 61.1, 57.5, and 2.9% of the asthmatic patients, respectively; however, the prescription rates dramatically dropped to 49.1, 37.5, 29.7, and 1%, respectively, after AIT treatment (Fig. 3A).
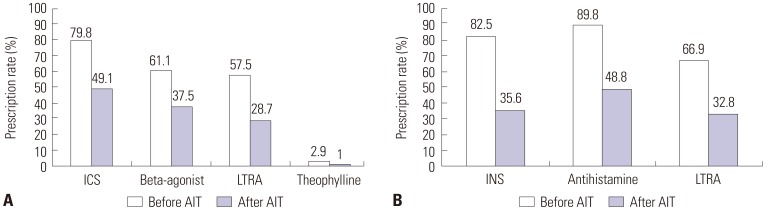
Fig. 3
Changes in drug prescription patterns after AIT. (A) Prescription patterns after AIT in patients with asthma. (B) Prescription patterns after AIT in patients with allergic rhinitis. AIT, allergen-specific immunotherapy; ICS, inhaled corticosteroids; LTRA, leukotriene receptor antagonists; INS, intranasal corticosteroid.
![]()
Drug prescription rates were also investigated in patients with allergic rhinitis. The prescription rates of intranasal corticosteroid, antihistamines, and LTRA were 82.5, 89.8, and 66.9%, respectively, before starting AIT. The prescription rates were significantly decreased to 35.6, 48.8, and 32.8%, respectively, after AIT (Fig. 3B).
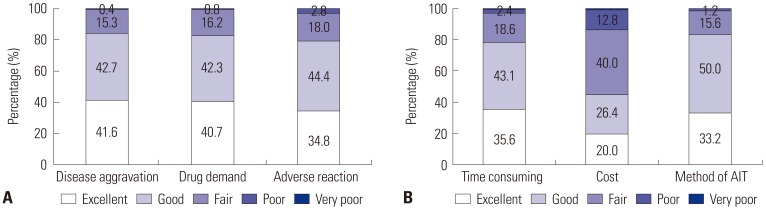
Medical and socioeconomic aspects of AIT
As for advantages of AIT, disease aggravation and drug demand were decreased such that patients reported a better than ‘good’ state in 84.3% and 83.0% of patients, respectively, and 79.2% of patients were in a better than ‘good’ state with respect to adverse reactions to AIT. Regarding economic aspects of AIT, 78.7% and 83.2% of patients reported a better than ‘good’ state for time consumption with AIT treatment and methodologic discomfort of AIT; however, 53.6% of patients described burden with the cost of AIT (Fig. 4). In addition, the rates of overall satisfaction with AIT higher than ‘good’ were 85.3% and 86.4%, respectively, in patients with asthma and allergic rhinitis (Fig. 5), and these were corresponded with those results of their physicians (kappa agreement=0.234, p<0.001 in allergic rhinitis and kappa agreement=0.373, p<0.001 in asthma). Interestingly, the rates of satisfaction with AIT for asthma tended to be higher in patients than in physicians.

Moreover, 91% of patients wanted to continue AIT, and 88.7% were willing to recommend AIT for other allergic patients. The results demonstrated that AIT can be a safe and effective therapeutic option for allergic patients in both medical and economic aspects, except for its cost.
The efficacy of AIT according to age groups
The efficacy of AIT was assessed in the pediatric and adult groups. Although parameters of allergic rhinitis/asthma symptoms or adverse reactions were not different between the groups (data not shown), there was a significant difference in guideline-based disease severity and medication use. The proportions of patients with intermittent severity asthma were 86.2% and 54.2%, respectively, in the pediatric and adult groups after AIT. The use of inhaled corticosteroids (ICS) (28.1% vs. 57.7%), beta-agonists (22.6% vs. 44.6%), and leukotriene receptor antagonists (LTRA) (9.4% vs. 36.8%) were significantly less frequent in the pediatric group than in the adult group. Moreover, the prescription rates of antihistamine were quite decreased in pediatric allergic rhinitis patients compared to those in adult patients (Table 2).
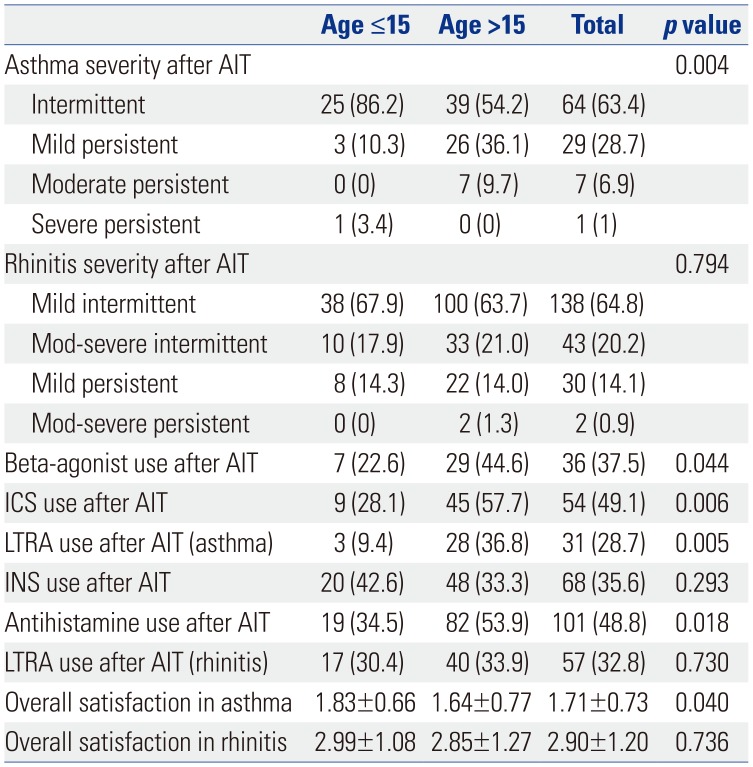
Table 2
Effects of AIT according to Age Groups
![]()
The overall rates of satisfaction with AIT for asthma were significantly higher in the pediatric group than in the adult group (1.83±0.66 vs. 1.64±0.77, p=0.040). However, such results were not observed in allergic rhinitis patients who received AIT (Table 2). Sex, adherence to AIT, initial disease severities, and associated diseases did not affect satisfaction with AIT in both asthma and rhinitis patients.
Taken together, our results showed that AIT might reduce allergy symptoms, medication use and disease severity based on the GINA or ARIA guidelines in Korean patients with asthma or allergic rhinitis.
DISCUSSION
In this cross-sectional study, we aimed to evaluate patient perspectives on AIT together with those of their physicians, and found excellent satisfactions with AIT in regarding to its efficacy and time-consuming and methodologic difficulties in both groups with good correlation. We also clearly showed that about three-quarter of the patients experienced symptom improvement within a year after AIT in this study.
Although many surveys of prescription patterns in AIT have been published,2324 studies regarding perspectives or satisfaction with AIT are extremely rare, especially in Korea. This study had some heterogeneity in disease patterns, hospital settings, ages, and products for AIT and the specialties of physicians due to its retrospective design. Despite this heterogeneity, it is interesting that the overall rate of satisfaction with AIT was more than 80% for asthma or allergic rhinitis patients, moreover, it was more than 70% for physicians. This result is in line with those of previous studies performed in Italy and Spain.1920 The rates of patient and physician satisfaction with AIT were 74/100 and 78/100, respectively, using VAS scores, and showed a significant similarity between them.25 The Satisfaction Scale for Patients Receiving Allergen Immunotherapy (ESPIA) totaled 69.2 points on a 0–100 scale after sublingual grass pollen immunotherapy.26 Although the methods for evaluating the overall rate of satisfaction with AIT were not similar between studies, AIT appeared to be an excellent therapeutic option meeting the expectations of allergic patients and physicians. In contrast, the most unsatisfactory part had answered the cost of AIT. More than 50% of patients answered fair or worse opinions in that question.
Another interesting result of this study was that the rate of satisfaction with AIT was higher in pediatric asthmatics than in adult asthmatics. While patient age does not seem to be a limitation to AIT, the efficacy of AIT according to age groups is still debatable. Asthma is a chronic inflammatory disease that leads to irreversible changes in the airway. Therefore, it would be advisable to start AIT earlier in the disease process. Our data showed no differences in allergy symptoms between patients of ages less than 15 years and those older than 15 years, but showed a significant difference in guideline-based disease severity and medication use after AIT, especially in asthmatics. Previous studies have reported similar results as ours. SLIT with house dust mite extracts seems to be as effective in school-age children and adolescents as in adults; however, the degree of reduction in medication use tended to be higher in the young age group than in the adolescent group.27 Interestingly, a significant difference in disease severity was found only in asthma, but not in allergic rhinitis. Airway remodeling such as collagen deposition could prominently occur in suboptimally treated or untreated asthma, in contrast, those features are not prominent in allergic rhinitis. We thought the above difference may attribute to our results in asthma and rhinitis. Moreover, some discrepancies in satisfaction rates with AIT for asthma between patients and physicians may have been attributed to the lack of objective monitoring tools such as pulmonary function tests to patients. Further studies are needed to confirm our findings.
Patients should be educated about AIT before the start of AIT because AIT requires a long treatment duration and sometimes causes hypersensitivity reactions. In this study, only 5.9% of the patients had heard about AIT from general practitioners. The Internet, media, or acquaintances were important sources of information on AIT. This could disseminate incorrect knowledge about AIT to many allergic patients. This finding was also in line with those of previous studies concerning the sources of information on AIT.131525 Approximately 30% of patients expected immediate therapeutic effects from AIT, and about 20% of the patients wanted the treatment to be performed for a short period of time.25 Our results can explain the reasons why AIT is not frequently offered to patients and why many patients hold misconceptions about AIT in Korea. We should consider the education of general practitioners and the use of multimedia for better understanding and more prescriptions of AIT in Korea.
AIT significantly decreased all clinical symptoms in patients with asthma or allergic rhinitis as reported in previous studies.2829 More than 80% of patients reported an ‘improved’ or ‘much improved’ state in regarding to clinical symptoms after AIT. In addition, disease severity, an objective parameter, was also reduced after AIT in many patients. In this study, 81.2% of allergic rhinitis patients showed a moderate to severe persistent state before AIT; 64.8% of the patients changed to mild intermittent state; and only 20.2% of the patients showed a moderate to severe intermittent state after AIT. Similarly, 7.9% of intermittent asthma patients turned to 63.4% after AIT. These results are also consistent with those of previous studies demonstrating that the severity of allergic rhinitis was reduced from moderate to severe severity to mild severity in 49.1% of patients.26 This study also showed the decreased medication prescription rate after AIT in both allergic rhinitis and asthma patients. Taken together, AIT might be very effective in improving disease severity and reducing the frequency of medication use.
Our survey evaluated the time of symptom improvement. About 15% of patients reported symptom improvement within 3 months, more than 30% of the patients within 6 months, and 75% of patients within 1 year. It is conceivable that AIT can show quick therapeutic effects through early desensitization of mast cells within 1 week and production of regulatory cytokines, such as IL-10 and TGF-beta, within 6 months.3031 Although further studies are needed to confirm our findings, time to symptom improvement can help to explain the onset timing of AIT to allergic patients.
Our study has some limitations. First, we only analyzed results from patients receiving subcutaneous immunotherapy. In a previous study in Korea, SLIT was usually prescribed by otolaryngologists.32 However, enrolled doctors in our study were only from internal medicine and pediatrics. This is the reason why the number of patients receiving SLIT was small in our study. Secondly, we could not compare the efficacy and safety of AIT between AIT products or administration methods. The questionnaire developed by an expert panel of the allergen and immunotherapy workgroup of the KAAACI was inadequate for these purposes. Our workgroup is planning to compare AIT products in future studies. However, the strengths of the present study are that data were collected in real-life settings and that relevant data based on current guidelines were provided for the management of patients receiving AIT, emphasizing the importance of the patient's point of view on AIT. Thirdly, since some children may have spontaneous remissions of allergic symptoms as they become older, we cannot confirm the superiority of AIT in childhood asthma on the basis of the above results.
In conclusion, in this study evaluating the perspectives on AIT in both patients and physicians, the majority of patients and physicians were satisfied with the efficacy and safety of AIT, except for its cost. Physicians who treat allergic patients should recognize the strength and weakness of AIT and recommend more AIT to allergic patients.
 XML Download
XML Download