

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Benign prostatic hyperplasia (BPH) is a common disease in men over the age of 50 and its incidence increases with age [1]. Treatment of BPH begins with medical therapy, which typically includes 5-alpha reductase inhibitors (5α-RIs) [2]. In fact, less than 1 in 5 men with BPH is treated with finasteride or dutasteride. Also, many men with BPH are treated with phosphodiesterase-5 inhibitors. Among an estimated 14 million USA men with symptomatic prostatic hyperplasia, 5a-RIs exposure rose from 4.3% in 1993 to 15.2%, or 2.1 million men in 2010 [3].
However, in more than 50% of cases 5α-RI administration is associated with sexual dysfunction (SD), such as loss of libido, erectile dysfunction (ED), and ejaculatory disorders [4]. Especially in recent years, finasteride-related permanent ED and various symptoms have been reported as post-finasteride syndrome, which collectively could refers to the side effects related to 5α-RI medication. Post-finasteride syndrome includes persistent sexual side effects of finasteride in young men [56], persistent emotional and cognitive impairment [7], and psychological side effects such as anxious/depressive symptoms and even suicidal thoughts [89].
In particular, 5α-RIs has been reported to induce ED in animal model and lead to microstructural changes of the corpus cavernosum in a rat model [1011]. Pinsky et al [10] demonstrated that dutasteride has a detrimental effect on erectile function, and that enhanced inducible nitric oxide synthase (iNOS) expression may protect penile smooth muscle from fibrosis. Zhang et al [11] showed that finasteride exposure for 4 weeks decreased the weight of the penile tissue, although it did not appear to affect the erectile responses to electrical stimulation in a rat model. Furthermore, even if the 5α-RI is discontinued ED might be persistent and irreversible in the rat model [12].
Two observational studies in humans have shown that longer exposure to finasteride posed a greater risk of ED and worsening ED [1314]. This study aimed to investigate the effects of dutasteride treatment duration on causing persistent ED even after discontinuation of treatment in a rat model.
Go to : 
MATERIALS AND METHODS
1. Ethics statement
We confirm that this study was conducted with approval from the Institutional Animal Care and Use Committee of Samsung Biomedical Research Institute (No. 20160523001). All experiments were performed in accordance with the relevant guidelines and regulations.
2. Preparation of animal model
A total of 76 male Sprague-Dawley rats were used in this study. The rats were assigned to five groups: (i) normal control (n=16); (ii) dutasteride (0.5 mg/rat/d) for 4 weeks of oral administration (n=15); (iii) dutasteride for 4 weeks plus 2 weeks of rest (n=15); (iv) dutasteride for 8 weeks of oral administration (n=15); and (v) dutasteride for 8 weeks plus 2 weeks of rest (n=15). All rats except for those in the normal control group were administered oral dutasteride 0.5 mg/rat/d. At the time of the experiments, including in vivo cavernous nerve stimulation, western blotting, and histological examination, the ages of all rats were almost equal, ranging from 17 to 20 weeks. In terms of measurement time point (4-week and 8-week), we expected that rats with 4 weeks of dutasteride could be recovered through a 2-week rest period, but not in the rats with 8 weeks of dutasteride.
3. Evaluation of in vivo erectile function
In vivo cavernous nerve stimulation was performed to investigate erectile function. The detailed methodology for measuring the erectile response to cavernous nerve stimulation has been described in previous studies [15]. The electrical field stimulation (EFS) parameters were as follows: 1, 2.5, and 5 V, 5 ms, 2 Hz, and a duration of 60 s using an electric stimulator (model PG 721A; Austin Electronic Specialties, Inc., Palo Alto, CA, USA). Sub-maximal EFS was introduced with 1 and 2.5 V as previously described [15]. By subdividing the power of stimulation, the subtle effects of erection could be compared among the groups. Erectile responses to cavernous nerve stimulation were compared among the five groups under sub-maximal stimulation. At the end of sub-maximal stimulation, the full response was measured using EFS of 5 V for comparison with sub-maximal stimulation and to ensure that the cavernous nerve was intact. Systemic arterial blood pressure was monitored via carotid artery cannulation with polyethylene-50 tubing. The ratio of maximal intracavernosal pressure (ICP) to mean arterial pressure (MAP) obtained at the peak of the erectile response was determined to control for variations in MAP. In addition, the area under curve (AUC) of ICP/MAP was calculated.
4. Western blot of the corpus cavernosum
For Western blot analysis, rat penile tissues stored at −70℃ were homogenised in ice-cold protein extraction solution (PRO-PREP; iNtRON Biotechnology, Seongnam, Korea) containing 1% phosphatase inhibitor cocktail 2 and 3 (Sigma Chemical Co., St. Louis, MO, USA) and then centrifuged at 12,000 rpm for 15 minutes at 4℃. The protein concentration was determined by Bradford assay (Bio-Rad, Hercules, CA, USA), and equal amounts of protein (30 µg) were separated by 4% to 20% sodium dodecyl sulfate (SDS)-polyarcylamide gel electrophoresis at 80 V for 4 hours in Tris/glycine/SDS buffer (25 mM Tris, 192 mM glycine, 0.1% SDS, pH 8.3; Bio-Rad) and transferred onto polyvinylidene difluoride membranes. After transfer, the membranes were blocked with 5% skim milk powder in Tris Buffered Saline with Tween 20 (TBST) (66 mM Tris base, 137 mM NaCl, 2.7 mM KCl, and 0.1% Tween 20, pH 7.4) for 1 hour at room temperature. The membranes were incubated with primary antibodies at 4℃ with overnight shaking. Primary antibodies included antiendothelial nitric oxide synthase (eNOS) (1:5,000; BD Biosciences, San Jose, CA, USA), anti-neuronal nitric oxide synthesis (nNOS) (1:200; Santa Cruz Biotechnology, Inc., Dallas, TX, USA), anti-iNOS (1:200; Santa Cruz Biotechnology, Inc.), anti-α-smooth muscle actin (1:1,000; Abcam, Cambridge, UK), anti-transforming growth factor (TGF)-β1 (1:500; Abcam), anti-TGF-β2 (1:1,000; Abcam), anti-Smad2/3 (1:1,000; Abcam), and anti-p-Smad2/3 (1:1,000; Cell Signaling Technology, Danvers, MA, USA). Anti-β-actin (1:5,000; Abcam) was used as an internal control. After washing with TBST, the membranes were incubated with secondary antibody (1:2,000; Santa Cruz Biotechnology, Inc.) for 1 hour at room temperature. After washing, signals were detected using a Bio-Rad Laboratories enhanced chemiluminescence detection kit. The generated images were analysed using ImageJ software to determine the integrated density for each protein band.
5. Masson's trichrome staining of the corpus cavernosum
The proportion of smooth muscle and collagen in the corpus cavernosum was calculated and compared among the five groups. Masson's trichrome staining was carried out as described previously using a Masson trichrome kit (Abcam) [1011]. Computer-assisted colour histomorphometry was used to assess the mean percentage of smooth muscle among total erectile tissue (smooth muscle plus connective tissue). Using image analysis software we examined 10 fields (×100 magnification) of each tissue section and quantitatively assessed the areas of smooth muscle (stained red) and connective tissues (stained blue) [11].
6. Drugs and solutions
Dutasteride was kindly provided by GSK Korea (Seoul, Korea). All other chemical agents were purchased from Sigma Chemical Co. Dutasteride was dissolved in normal saline and administered at 0.5 mg/rat/d via intragastric tube. All other drugs were also dissolved in normal saline.
7. Data analysis
Erectile responses were measured with cavernous nerve stimulation and were compared among five groups: normal control, dutasteride 4 weeks, dutasteride 4 weeks plus 2 weeks of rest, dutasteride 8 weeks, dutasteride 8 weeks plus 2 weeks of rest. This comparison was also performed by serially increasing electrical stimulation voltage. The outcomes of western blot and Masson's trichrome staining were additionally compared among all five groups.
8. Statistical analysis
All outcomes were described as the mean±standard error. Data were compared using a two-tailed Student t-test and one-way ANOVA test with Bonferroni post-hoc analysis. All statistical analyses were conducted using IBM SPSS ver. 23.0 (IBM Co., Armonk, NY, USA), and p<0.05 was considered statistically significant.
Go to :
RESULTS
The mean weight of rats was 538.8±12.3 g (normal control), 471.7±8.5 g (dutasteride for 4 weeks), 504.5±8.6 g (dutasteride for 4 weeks plus 2 weeks of rest), 560.7±7.7 g (dutasteride for 8 weeks), and 540.5±7.3 g (dutasteride for 8 weeks plus 2 weeks of rest), respectively (p>0.05). In the dutasteride experimental groups, no abnormal behaviour was observed during oral administration of dutasteride.
1. In vivo erectile function of rats
In vivo erectile responses to cavernous nerve stimulation with 1, 2.5, and 5 V were increased in a stimulusdependent manner for maximal ICP, ICP/MAP ratio, and AUC of ICP/MAP (Fig. 1). Oral administration of dutasteride for 4 weeks significantly decreased all erectile parameters compared with the control group (all comparisons, p<0.05). These reduced erectile responses were almost recovered after 2 weeks of drug-free time (Fig. 1). However, 8 weeks of dutasteride oral administration led to irreversible ED in the rat model (Fig. 2). Rats in both the 8 weeks dutasteride group and the 8 weeks dutasteride plus 2 weeks of rest group showed significantly decreased erectile parameters compared with the control group (p<0.05). In the case of 8 weeks dutasteride group, decreased erectile parameters were not improved by 2 weeks of resting. Representative ICP/MAP traces for each group were shown in the supplement.
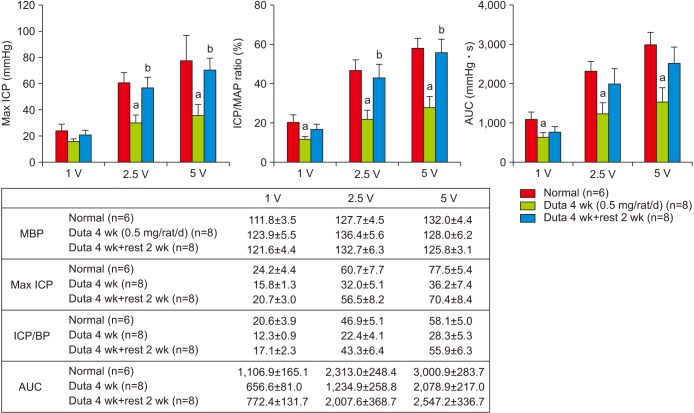 | Fig. 1In vivo erectile responses to serial electrical stimulation in the normal control, 4-week dutasteride group, and 4-week dutasteride with 2-week resting group. Duta: dutasteride, ICP: intracavernosal pressure, MAP: mean arterial pressure, AUC: area under curve. MBP: mean blood pressure, BP: blood pressure. ap<0.05 vs. Normal, bp<0.05 vs. Dutasteride 4-week group.
|
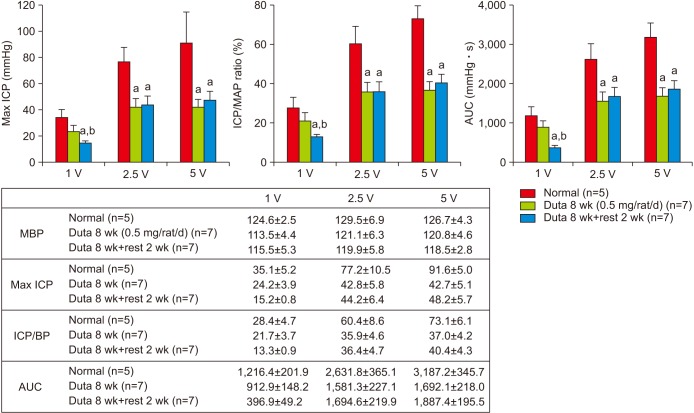 | Fig. 2In vivo erectile responses to serial electrical stimulation in the normal control, 8-week dutasteride group, and 8-week dutasteride with 2-week resting group. Duta: dutasteride, ICP: intracavernosal pressure, MAP: mean arterial pressure, AUC: area under curve. MBP: mean blood pressure, BP: blood pressure. ap<0.05 vs. Normal, bp<0.05 vs. Dutasteride 8-week group
|
2. Change in fibrotic factors in rat corpus cavernosum induced by dutasteride
There was no significant change in protein levels of fibrosis-related factors including TGF-β1, TGF-β2, and p-Smad 2/3 after 4 weeks of dutasteride oral administration (p>0.05; Fig. 3A). In contrast, expression of TGF-β1, TGF-β2, and p-Smad 2/3 was significantly enhanced by 8 weeks of treatment with dutasteride (p<0.05; Fig. 3B). Increased levels of these fibrotic factors were maintained even after 2 weeks of resting. There were subtle, but not statistically significant, changes in the level of nNOS and eNOS after medication and discontinuation. A significantly decreased level of iNOS with 4 and 8 weeks of dutasteride administration was observed, and these reductions showed compensatory rebounds over a 2-week resting period.
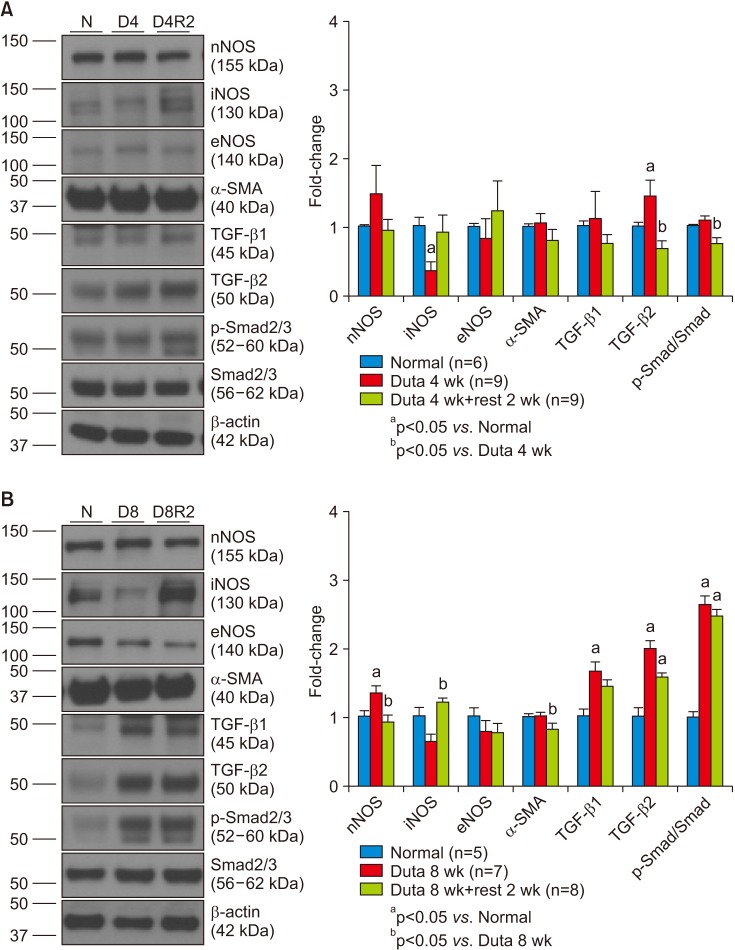 | Fig. 3(A) The changes in protein levels (protein: 40 µg) of fibrosis-related factors transforming growth factor (TGF)-β1, TGF-β2, and p-Smad/Smad (Smad 2/3) in the 4-week dutasteride group. (B) Changes in protein levels (protein: 40 µg) of fibrosis-related factors in the 8-week dutasteride group. N: normal control, D4: dutasteride 4 weeks, D4R2: dutasteride 4 weeks plus 2 weeks of rest, D8: dutasteride 8 weeks, D8R2: dutasteride 8 weeks plus 2 weeks of rest, nNOS: neuronal nitric oxide synthesis, iNOS: inducible nitric oxide synthase, eNOS: endothelial nitric oxide synthase, SMA: smooth muscle actin, Duta: dutasteride.
|
3. Change of smooth muscle contents and fibrosis in rat corpus cavernosum
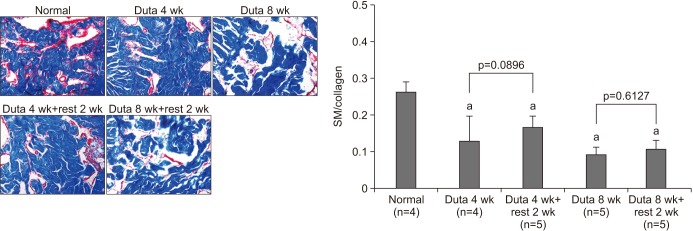
The ratio of smooth muscle (staining red) and collagen content (staining blue) in the rat cavernosal tissue was determined using Masson's trichrome staining (Fig. 4). Dutasteride administration markedly decreased smooth muscle content and increased collagen after 4 and 8 weeks of oral administration (p<0.05). There was no significant improvement in the smooth muscle to collagen ratio after the rest period in both the 4- and 8-week groups. In the 4 weeks of dutasteride, it tended to recover microstructural change through 2 weeks of resting, but not significant.
Go to :
DISCUSSION
The half-life of dutasteride is known to be 5 weeks in humans [16], so it takes at least 5 to 6 months for wash-out. In addition, 6 months to 1 year is usually needed for restoration of the structural and functional changes caused by long-term dutasteride treatment in various organs [1718]. It is assumed that almost 12 days in an adult rat is equivalent to 1 human year using a model based on comparison with normal human lifespan [19]. The half-life of dutasteride is approximately 14 hours in rats [20]. Thus, at least 1 week is necessary for complete wash-out. Taking these aspects into account, we assumed that 2 weeks of rest was a sufficient period to assess the restoration of erectile function after long-term dutasteride treatment in rats, and this was applied in our study as well as in other studies [12].
Long-term dutasteride administration induced a decrease in erectile function response to in vivo nerve stimulation and molecular changes such as a decrease in nNOS and compensatory increase of iNOS, all of which have previously been confirmed in other studies [1012]. iNOS seemed to be suppressed during treatment and then recovered during the rest period. These molecular changes were further enhanced in the rats with 8 weeks of administration compared with 4 weeks. We found that these changes recovered during a 2-week withdrawal period after 4 weeks of treatment, and not after 8 weeks.
In the present study the increase in collagen and decrease in smooth muscle content at 4 weeks were significantly meaningful. Although sexual functionality was not affected, microstructural changes in the corpus cavernosum were already beginning. In the 4 weeks of dutasteride, it tended to recover microstructural change through 2 weeks of resting, but not significant. It could be explained that the microstructural change did not occur enough to affect the erectile function. In the rat model, long-term suppression of serum dihydrotestosterone (DHT) leads to a decrease in smooth muscle and structural changes, resulting in permanent ED. On the other hand we cannot observe that dutasteride treatment affect nuclear size change of corpus smooth muscle in the current study, although there are reports that androgen deprivation therapy results in small, dense nuclei in prostate cancer [21]. Microstructural changes beyond a critical point eventually affect the function and seem to be irreversible. In this study, we determined the critical point in the rat model to be around 4 to 8 weeks of dutasteride administration. Based on these results, it can be inferred that human beings also have a critical point for 5α-RI treatment.
Androgen (including DHT) deficiency is involved in TGF-β/Smad signalling pathways that induce fibrosis and increase connective tissue deposition in several organs [2223]. TGF-β1 plays a key role in vascular fibrosis via the Smad pathway [24]. Although it differs in organ and cells, fibrosis shares some common characteristics. However, whether it plays in similar role in the pathological process of penile fibrosis induced by androgen deficiency is not clear. In the current study, the TGF-β/Smad pathway was activated in the 8-week dutasteride group and was not recovered by 2 weeks of washout. Experimental results showed that the TGF-β/Smad signalling pathway was involved in the pathological process of penile fibrosis caused by 8-week treatment with dutasteride, which might partially explain the underlying mechanism.
These results have several important implications. First, the use of dutasteride medication for longer than a specific period caused a timeframe irreversible ED in the rat model. Duration of administration might be one of the most critical factors in induction of permanent ED in the rat model. Two previous studies demonstrated that 5α-RI administration in rats increases the risk of ED and that some changes in penile smooth muscle function are persistent [1012]. In addition, the current results showed permanent ED or time-dependent recovery in rats after 5α-RI treatment. In addition to the animal model, the present outcome has a critical impact on the clinical setting as permanent ED might also be induced in men treated with long-term 5α-RIs with respect to post-finasteride syndrome. We already know the effects of intermittent androgen deprivation therapy on sexual function in patients with prostate cancer [25]. Intermittent therapy has potential benefits with respect to physical function, fatigue, urinary problems, hot flashes, libido, and erectile function [26], as well as non-inferiority to continuous androgen deprivation therapy regarding primary oncologic outcomes [2527]. Extrapolation from studies of intermittent therapy versus continuous therapy leads to the expectation of a beneficial effect of intermittent 5α-RI therapy regarding SD in patients with moderate to severe BPH. It would be clinically meaningful to determine the proper administration duration and recovery time of 5α-RIs to maintain the clinical effects on BPH while also reducing adverse events.
Despite the robust data supporting post-finasteride syndrome, little is known about the underlying aetiology driving this phenomenon. A recent meta-analysis supported the view that 5α-RIs negatively impact erectile function [28]. Some have speculated that this effect could be nocebo or physiological, resulting from changes in SHBG bound/unbound testosterone in the face of falling DHT levels. Many men have been exposed to these two medications for many years. Recently published data on a large cohort of men who were exposed to finasteride identified that 1.4% of men had persistent ED after discontinuation, and that this side effect was associated with increased treatment duration [13]. We aimed to identify the factors causing this phenomenon in rats. Our results suggest that duration of 5α-RI medication could be one of the important factors causing ED in rats.
Actual drug adherence for BPH has been reported to be considerably low in terms of 5α-RI medication with rates of 59% at 6 months and 18% at 12 months [29]. One of the most important reasons for this lack of adherence is ED. Even patients with advanced or metastatic prostate cancer still hope that they can have a decent quality of life during treatment of their malignancy. In the case of men with benign disease, such as BPH, preservation of normal sexual function and quality of life during the treatment is essential. It is well known that 5α-RIs play beneficial roles in the management of BPH [30]. Thus, ED in men treated with 5α-RIs should be managed carefully.
There are several limitations in the present study. When determining permanent ED of the rat model it is unclear what would happen with a longer wash-out time (i.e., more than 2 weeks). However, as described above 2 weeks of rest should be long enough to evaluate the obvious detrimental effects of 5α-RIs on erectile function. Second, we did not figure out more detailed time points of dutasteride administration that can cause permanent ED in the rat model. Thus, we could not determine maximal duration of dutasteride without impairment on erectile function. Third, the use of high doses of dutasteride in rats is a limitation. However, the dose was determined by reference to several papers [1012]. In general, it is common to administer high doses of drugs to produce efficacy in animal studies. Lastly, the age of the rats ranged from 17 weeks to 20 weeks and was not constant. This might had some impact on the outcome of erectile function.
Go to :
CONCLUSIONS
In a rat model, the reduction of DHT by dutasteride decreased erectile responses to electrical stimulation. This was accompanied by changes in protein levels and histological features, and resulted in increased fibrosis and decreased smooth muscle content in the corpus cavernosum. The current study demonstrated that recovery from ED depended on the duration of medication, and that administration of dutasteride for longer than a critical period (more than 8 weeks) could result in irreversible ED, even after discontinuation of dutasteride. Further studies on ED and the re-establishment of treatment in human models are essential.
Go to :
 XML Download
XML Download