

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In 2014, there were 112,882 newly diagnosed cases of cancer among males in South Korea [1]. The development of new chemotherapy and radiotherapy techniques has increased the survival rate for many types of cancer from 50% in the 1970s to 70% in 1990s [2]. The current cure rate for patients with testicular cancer and lymphoma are as high as 90% [2]. However, cancer therapies, including chemotherapy and radiation therapy, can impair male reproductive function by directly damaging the germinal epithelium, causing oligozoospermia or azoospermia, or by damaging the neural pathways that regulate erection and ejaculation [3]. In addition, cytotoxic chemotherapy may also lead to transmission of genetic damage to children conceived after tretment [3]. The effect of cancer treatment on the incidence and severity of testicular dysfunction depends on various factors, including type of therapeutic regimen and cumulative dose [4].
It is difficult to predict which cancer patients will recover spermatogenesis function and which will remain infertile. Therefore sperm cryopreservation before cancer treatment is the most valuable and effective method to preserve the reproductive capacity for males of reproductive age undergoing cancer treatment [5]. Moreover, a patient's knowledge that his fertility can be secured through sperm cryopreservation may help in the emotional battle against cancer [6].
Fertility Center of CHA Gangnam Medical Center (Seoul, Korea) has performed sperm cryopreservation in patients diagnosed with cancer since January 1996. We evaluated data from our 21 years of experience with banked sperm by examination of cancer type, semen quality at banking, and current status of cryopreserved sperm including use rate or ongoing preservation rate. These long-term data could be helpful for oncologists and patients who are considering sperm cryopreservation before cancer treatment.
Go to : 
MATERIALS AND METHODS
1. Subject and study design
A total of 721 patients with cancer successfully performed sperm cryopreservation for fertility preservation through masturbation at our fertility center from January 1996 to December 2016. Patients who failed to cryopreserve semen because of azoospermia or having insufficient sperm quality for freezing, or who banked testicular sperm after testicular sperm extraction were not included. The medical charts of all patients were retrospectively reviewed and data on patient age, marital status, cancer type (determined by the oncologist's referral document), semen volume, sperm count and motility, length of storage, and current banking status were extracted. All semen samples were collected in sterile plastic containers by masturbation. After liquefaction, semen parameters were determined according to World Health Organization guidelines at the time of sample collection [789]. Semen samples were cryopreserved if motile sperm were present. Semen was mixed with the same volume of Sperm Freezing Medium (Origio, Denmark), and then incubated at room temperature for 10 minutes. The mixture was then dispensed into cryogenic tubes consisting of ionomer resin (CBS™ High Security cotton-plugged sperm straws; Cryo Bio System, L'Aigle, France). Prepared samples were suspended just above the surface of liquid nitrogen for 30 minutes, and then immersed into the liquid nitrogen (−196℃).
The initial duration of sperm cryopreservation was 3 years. Then, freezing was extended each subsequent year after confirmation by direct contact or a telephone call with the patient or legal guardian. Patients had the option to discard the frozen samples or to proceed with assisted reproductive technology (ART) at another fertility center, in which case the sample was transferred. If the patient died during or after cancer treatment, all samples were discarded. The current banking status (determined in October 2017) includes samples used in our fertility center, transferred to other centers, electively discarded, discarded secondary to death, and those still in storage.
2. Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board of CHA Gangnam Medical Center of CHA University (Reg. No. GCI-17-83).
All patients provided informed written consent before sperm cryopreservation. If the patient was a minor, informed written consent was obtained from the parents or legal guardians. For married patients, spousal consent was required for sperm banking.
3. Statistical analysis
All data are presented as means±standard deviations or medians and ranges. The significance of differences between groups was evaluated using analysis of variance (ANOVA) and the Mann-Whitney U-test. An alpha value of 5% was considered the threshold for significance. SPSS ver. 12.0K (SPSS Inc., Chicago, IL, USA) was used for statistical analysis.
Go to :
RESULTS
The major types of cancer in the 721 patients (Table 1) were leukemia (n=205, 28.4%), lymphoma (n=132, 18.3%), testis cancer (n=72, 10.0%), severe aplastic anemia (n=61, 8.5%), sarcoma (n=35, 4.8%), thyroid cancer (n=29, 4.0%), rectal cancer (n=20, 2.8%), myelodysplastic syndrome (n=18, 2.5%), brain tumor (n=10, 1.4%), stomach cancer (n=9, 1.2%), lung cancer (n=7, 1.0%), other hematologic cancers (n=7, 1.0%), colon cancer (n=6, 0.8%), prostate cancer (n=5, 0.7%), mediastinal cancer (n=5, 0.7%), and multiple myeloma (n=5, 0.7%). There were fewer than 5 patients per cancer type for 36 patients (5.0%; including bladder cancer, skin cancer, retroperitoneal tumor, breast cancer, urachal cancer, biliary duct cancer, and tongue cancer) and 59 patients (8.2%) had insufficient medical chart information. Analysis of marital status indicated 584 patients (81.0%) were unmarried, 80 (11.1%) were married, and 57 (7.9%) had unknown status.
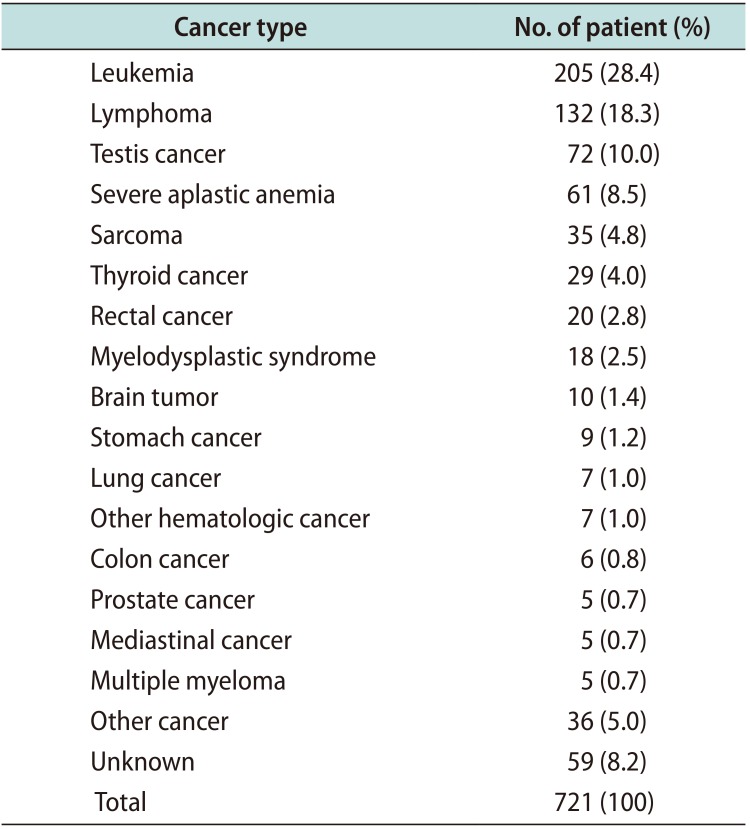
Table 1
Cancer type of patients who underwent sperm cryopreservation
![]()
The mean patient age at sperm cryopreservation was 27.0±7.9 years (range, 13–65 years). A total of 1,120 sperm samples were collected, and there was a mean of 3.1±1.7 samples per patient (range, 1–10). The mean sperm concentration was 66.7±66.3 ×106/mL (range, 0.09–420 ×106/mL) and the mean sperm motility was 33.8%±16.3% (range, 0%–77%).
A one-way ANOVA indicated a relationship of semen parameters with type of cancer (Table 2). In particular, the sperm concentration in patients with testis cancer (37.9±40.5 ×106/mL) was significantly lower than that of patients with other cancers, including leukemia, lymphoma, sarcoma, thyroid cancer, rectal cancer, and myelodysplastic syndrome. This may be because 40 of the 72 patients (55.6%) with testis cancer received unilateral radical orchiectomy before sperm cryopreservation. Sperm motility in patients with leukemia (28.1%±16.6%) was significantly lower than that of patients with lymphoma, testis cancer, sarcoma, thyroid cancer, rectal cancer, and stomach cancer (Table 2).
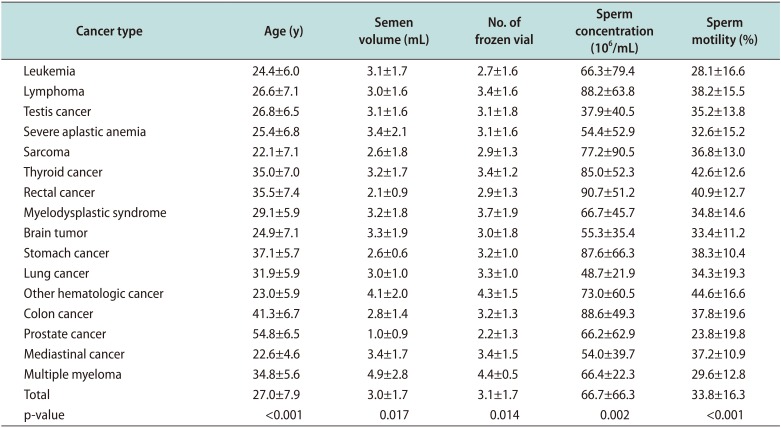
Table 2
Semen characteristics at cryopreservation according to cancer type
![]()
In spite of recommendations to perform sperm banking before cancer treatment, 111 patients (15.4%) underwent sperm cryopreservation during or after cancer treatment. Relative to patients who banked sperm before cancer treatment, those who banked sperm during or after cancer treatment had a significantly lower sperm concentration (p<0.001) and lower sperm motility (p<0.001) (Table 3).

Table 3
Semen characteristics at cryopreservation according to cancer treatment
![]()
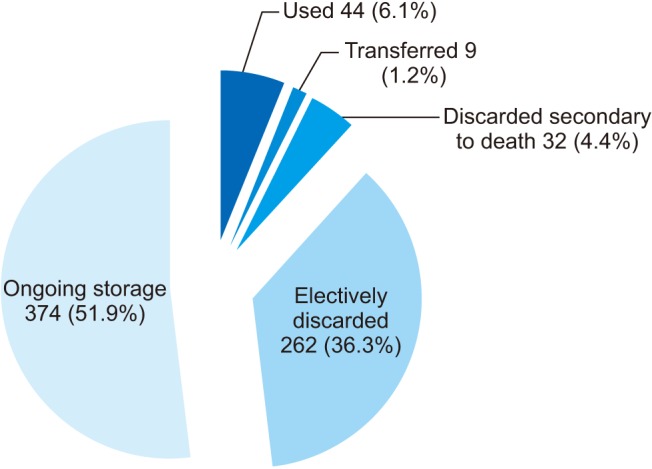
Our fertility center initially banks the sperm of cancer patients for 3 years, and provides additional storage for 1 year at a time after patient confirmation. During the follow-up (median duration, 75 months; range, 1–226 months), 44 patients (6.1%) used banked sperm from our fertility center for ART, 9 patients (1.2%) transferred their banked sperm to another center before starting ART, samples from 32 patients (4.4%) were discarded due to patient death, 262 patients (36.3%) electively discarded their samples, and 374 patients (51.9%) requested continuation of storage (Fig. 1). Among the 44 patients who used banked sperm for ART, the median duration from sperm cryopreservation to sperm use was 51 months (range, 1–158 months). Analysis of the types of cancer in these 44 patients indicated that 9 had thyroid cancer, 7 had lymphoma, 6 had leukemia, 5 had severe aplastic anemia, 4 had sarcoma, 1 had testis cancer, 1 had rectal cancer, 1 had prostate cancer, 1 had urachal cancer, 1 had bile duct cancer, and 8 had unknown types of cancer. Thus, the overall rate of sperm use for ART was 31.0% (9/29) for thyroid cancer patients, 5.3% (7/132) for lymphoma patients, 2.9% (6/205) for leukemia patients, 8.2% (5/61) for severe aplastic anemia patients, and 11.4% (4/35) for sarcoma patients. However, because of the small number of patients who used their sperm for ART during the study period, longer investigations are needed to confirm any effect of cancer type on use of ART. Among the 44 patients who used banked sperm for ART, ART information was only available for only 38 patients. Clinical pregnancy was confirmed in 22 patients by ultrasound visualization of a gestational sac. Sperm used for ART after 158 months of cryopreservation led to clinical pregnancy in 2 patients.
Go to :
DISCUSSION
The use of chemotherapy or radiotherapy to treat various cancers in men may lead to temporary, longterm, or permanent gonadal toxicities, depending on the type and dose of the therapeutic agent [10]. More specifically, chemotherapy induces the depletion or arrest of spermatogonial differentiation and mutagenesis in cells at later stages of development [4]. In contrast, radiotherapy affects the spermatogonia, the most radiosensitive cells due to their intense mitotic activity and spermatids [4]. Spermatids are unprotected because they lack mechanisms for DNA repair due to postmeiotic differentiation and chromatin condensation [411]. Patients receiving high doses of alkylating agents are very likely to become azoospermic, although spermatogenesis may recover over time [12]. Although male cancer patients receiving low doses of cytostatic agents may expect recovery of spermatogenesis at about 12 weeks after the end of chemotherapy, permanent azoospermia occurs in more than 50% of patients receiving high doses of these drugs [13]. All men with cancer who are of reproductive age should be counseled regarding the possible effects of cancer treatment on testicular function and risk of potential sperm DNA damage. Previous research indicated an increased frequency of sperm aneuploidy after the initiation of chemotherapy, and that this may persist up to 18 months or longer [14]. The American Society of Reproductive Medicine Ethics Committee and the American Society of Clinical Oncology both recommended that physicians inform all cancer patients about options for fertility preservation before treatment [1516]. If this is not possible, then patients should be warned of the increased potential of genetic damage to sperm after initiation of chemotherapy or radiotherapy [3]. Although sperm banking is recommended before cancer treatment to obtain good sperm quality and to prevent potential DNA damage, some patients undergo cryopreservation during or after cancer treatment because of the urgency of treatment or a lack of information on the best methods for preservation of fertility. A survey by Schover et al [17] showed that although 91% of USA oncologists agreed that sperm banking should be offered to all male cancer patients, 48% admitted to never bringing up the topic or mentioning it to less than 25% of eligible men. The present study of 721 men with cancer indicated that 111 patients (15.4%) performed sperm cryopreservation during or after cancer treatment. As expected, patients who banked sperm during or after cancer treatment had significantly lower sperm concentrations and lower sperm motility than those who banked their sperm before cancer treatment. This supports the policy that sperm banking should be offered to all men undergoing potentially gonadotoxic cancer therapy before the onset of treatment. Regular communication between oncologists and reproductive specialists and provision of complete information to patients of reproductive age is required not to miss the chance or not to be too late for fertility preservation.
Previous reports on sperm banking in cancer patients demonstrated that testicular cancer patients had the lowest median pre-thaw counts and motility [1819]. Ku et al [20] performed a small retrospective study on sperm banking and reported that patients with testis cancer had significantly lower sperm concentrations than those with other cancers. van Casteren et al [21] noted that poor semen quality was common before the start of chemotherapy in men with testicular tumors, especially those with a non-seminoma testis cancer. In addition, Williams et al [22] showed that men with pretreatment testicular cancer had significantly lower semen quality than those with other malignancies, and suggested the possible causes were preexisting defects in germ cells, local tumor effects, endocrine disturbances, and autoimmune and systemic effects of cancer [23]. We found that the sperm concentration of patients with testis cancer (37.9±40.5 ×106/mL) was significantly lower than that of patients with other cancers including leukemia, lymphoma, sarcoma, thyroid cancer, rectal cancer, and myelodysplastic syndrome. This may be because 40/72 patients (55.6%) with testis cancer received unilateral radical orchiectomy before sperm cryopreservation.
Among our 721 cancer patients who performed sperm cryopreservation, 44 (6.1%) used their banked sperm at our fertility center for ART and 9 (1.2%) transferred their banked sperm to another center for ART during median follow-up duration of 75 months (range, 1 to 226 months). The median duration from cryopreservation to sperm use for ART was 51 months (range, 1 to 158 months), which is similar to previous report. van Casteren et al [24] reported that among 557 patients who banked semen, 42 (7.5%) requested use of the banked sperm after a mean time of 57 months (range, 15 to 130 months). If we classify transferred sperm as being used for ART, 7.4% of our banked sperm was used for ART. The rate of banked sperm use in our study is comparable with that reported in other large studies. The rate of cryopreserved semen use among cancer patients is often less than 10% to 15%, and differs widely among studies [24]. A recent systemic review showed the rate of cryopreserved semen use among cancer patients ranged between 2% and 60%, with an aggregate value of 8% (95% confidence interval, 8%–9%) [25]. Patient survival, recovery of spermatogenesis, and follow-up duration could all affect the rate of banked sperm use. We expect the use of banked sperm will increase over time, as more men decide to use their semen to conceive children. Therefore, longer follow-up data are needed to estimate the cumulative rate of frozen sperm use.
The limitations of our study include its retrospective design and the lack of detailed data on ART outcomes including live birth rate. However, to our knowledge, this study is among the largest studies and used among the longest follow-up periods to examine cryopreserved semen of cancer patients in a single fertility center. These long-term data could be helpful for oncologists and patients who are considering sperm cryopreservation before cancer treatment.
Go to :
CONCLUSIONS
Sperm cryopreservation before gonadotoxic treatment is the most reliable and noninvasive method to preserve male fertility. Sperm cryopreservation should be offered to all men who plan to receive cancer therapy. Efficient communication and counseling among the oncologist, patient, and reproductive specialist is mandatory so that fertility can be preserved for cancer patients of reproductive age. Even though only 6.1% of our patients used their banked sperm at our fertility center for ART and 1.2% transferred their sperm to another center for ART, we expect that a large number of men will use their samples for ART in the future.
Go to :
 XML Download
XML Download