

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obesity is a major public health concern worldwide due to its rapidly increasing prevalence and the common association with various metabolic alterations, also known as metabolic syndrome. It is characterized by a collection of risk factors for cardiovascular disease and type 2 diabetes mellitus, such as abdominal obesity, an elevated level of triglycerides, hyperglycemia, elevated blood pressure, and low high-density lipoprotein [1].
Obesity is a key component of metabolic syndrome, and their components are linked to a clustering feature, which is well-known as the common soil hypothesis. The main pathophysiologic processes of common soil are oxidative stress, inflammation, and insulin and leptin resistance (Table 1) [23]. Erectile dysfunction (ED) has recently become a concern as a factor of metabolic syndrome in men [4].
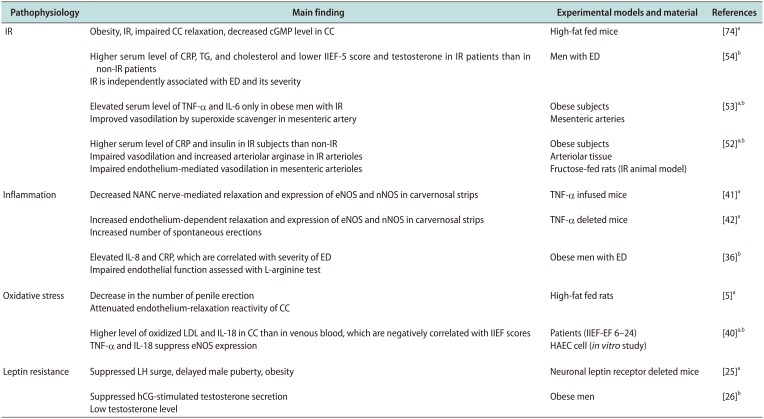
Table 1
Summary of the common pathophysiology of obesity and ED
| Pathophysiology | Main finding | Experimental models and material | References |
|---|---|---|---|
| IR | Obesity, IR, impaired CC relaxation, decreased cGMP level in CC | High-fat fed mice | [74]a |
| Higher serum level of CRP, TG, and cholesterol and lower IIEF-5 score and testosterone in IR patients than in non-IR patients | Men with ED | [54]b | |
| IR is independently associated with ED and its severity | |||
| Elevated serum level of TNF-α and IL-6 only in obese men with IR | Obese subjects | [53]a,b | |
| Improved vasodilation by superoxide scavenger in mesenteric artery | Mesenteric arteries | ||
| Higher serum level of CRP and insulin in IR subjects than non-IR | Obese subjects | [52]a,b | |
| Impaired vasodilation and increased arteriolar arginase in IR arterioles | Arteriolar tissue | ||
| Impaired endothelium-mediated vasodilation in mesenteric arterioles | Fructose-fed rats (IR animal model) | ||
| Inflammation | Decreased NANC nerve-mediated relaxation and expression of eNOS and nNOS in carvernosal strips | TNF-α infused mice | [41]a |
| Increased endothelium-dependent relaxation and expression of eNOS and nNOS in carvernosal strips | TNF-α deleted mice | [42]a | |
| Increased number of spontaneous erections | |||
| Elevated IL-8 and CRP, which are correlated with severity of ED | Obese men with ED | [36]b | |
| Impaired endothelial function assessed with L-arginine test | |||
| Oxidative stress | Decrease in the number of penile erection | High-fat fed rats | [5]a |
| Attenuated endothelium-relaxation reactivity of CC | |||
| Higher level of oxidized LDL and IL-18 in CC than in venous blood, which are negatively correlated with IIEF scores | Patients (IIEF-EF 6–24) | [40]a,b | |
| TNF-α and IL-18 suppress eNOS expression | HAEC cell (in vitro study) | ||
| Leptin resistance | Suppressed LH surge, delayed male puberty, obesity | Neuronal leptin receptor deleted mice | [25]a |
| Suppressed hCG-stimulated testosterone secretion | Obese men | [26]b | |
| Low testosterone level |
ED: erectile dysfunction, IR: insulin resistance, CC: corpus cavernosum, cGMP: cyclic guanosine monophosphate, CRP: C-reactive protein, TG: triglycerides, IIEF-5: international index of erectile function-5, TNF-α: tumor necrosis factor-alpha, IL: interleukin, NANC: nonadrenergicnoncholinergic, eNOS: endothelial nitric oxide synthase, nNOS: nervous nitric oxide synthase, LDL: low-density lipoprotein, HAEC: human aortic endothelial cell line, LH: lutenizing hormone, hCG: human chorionic gonadotropin.
aBasic research. bClinical research.
![]()
There is evidence from animal to human research supporting the association between obesity and ED. In particular, De Souza et al [5] reported that high caloric diet-induced ED resulted from endothelial damage in rats. A 14-year prospective study demonstrated that obesity is an independent risk factor for ED [6]. Fillo et al [7] observed that men with abdominal obesity had a higher incidence rate of ED and the incidence rate was elevated in proportion to the degree of obesity. Moreover, the severity of ED has been shown to be correlated with comorbid medical conditions including obesity, which results in a reduced responsiveness to phosphodiesterase 5 (PDE5) inhibitors in severely obese patients [8]. Weight reduction with bariatric surgery has been reported to improve ED in obese men significantly [9]. An animal study demonstrated that bariatric surgery improves glucose tolerance and elevates intracavernosal pressure and endothelial nitric oxide synthase (eNOS) and nervous nitric oxide synthase (nNOS) expressions in Otsuka Long-Evans Tokushima fatty rats [10]. Moreover, Kun et al [11] observed that gastric bypass surgery decreases serum cholesterol and triglycerides levels and carvernosal intima-media thickness and increases endothelial function score in a clinical study. Lifestyle modification and exercise also improve ED [121314]. The major connections between obesity and ED are derangements of hypothalamic regulation of the neuroendocrine system and endothelial dysfunction [15].
In this aspect, concomitant treatment of metabolic derangements associated with obesity in patients with ED who are obese would improve treatment efficacy in patients with ED and reduce the refractory response to penile vasodilators because obesity and ED may share common soil.
In this review, we discuss the linking factors between obesity and ED as well as possible combined treatment modalities.
Go to : 
OBESITY
Although obesity is induced when caloric intake chronically exceeds expenditure, its causes are complicated and heterogeneous. The human body has fine regulating mechanisms to control body weight homeostasis. However, these mechanisms often fail because of various causes, such as genetic, hormonal, psychological, metabolic, physical, and social defects [16].
The hypothalamus is the center for regulating body weight homeostasis and consists of various input signals such as leptin, insulin, ghrelin, and the autonomic nervous system. Output signals regulate appetite and thermogenesis [17]. The classic and most important input signal is the leptin circuit. Leptin, an ob gene product secreted by adipose tissue acts on the hypothalamus, induces suppression of appetite and increases thermogenesis [18]. The mutation of the ob gene or the leptin receptor leads to severe obesity, such as in ob/ob and db/db mice. However, the leptin concentration is elevated in obese rodents and humans owing to leptin resistance. In addition to body weight regulation, the hypothalamus also controls the endocrine system, reproduction, body temperature, and the autonomic nervous system [19].
1. Leptin resistance and low testosterone level
Obesity is not considered a pathologic condition of adipose tissue per se, but a systemic condition that affects various tissues from the hypothalamus to peripheral tissues. The main pathological features of obesity are elevated lipid concentrations in the blood; secretion of adipokines from hypertrophied adipocytes; and inflammatory responses due to the infiltration of immune cells into the adipose tissues, with resultant leptin and insulin resistance [1820].
Elevated free fatty acids (FFA) induce lipotoxicity and oxidative stress in peripheral tissues as well as generate an inflammatory response in the hypothalamus the control center for metabolism and reproduction. The inflammatory response in the hypothalamus disturbs normal regulatory processes, such as neuroendocrine regulations and maintenance of leptin sensitivity [21]. Among these disturbances, the decreased secretion of gonadotropin-releasing hormone (GnRH) associated with leptin resistance reduces the levels of testosterone, which is one of the causes of ED. Leptin resistance is a characteristic feature of obesity, and it is well known that leptin affects reproduction [19]. One of the possible mechanisms for leptin-resistance-induced GnRH suppression in the hypothalamus is overexpression of agouti-related peptide and neuropeptide Y, which results from a lack of inhibition by leptin and leads to the suppression of GnRH secretion in mice [22]. In addition to leptin's stimulatory effect on GnRH secretion, leptin inhibits testosterone secretion at the testicular level. Thus, obesity with leptin resistance and secondary hyperleptinemia shows lowered testosterone because of a weakened stimulatory effect of leptin on GnRH secretion and the inhibitory effect of leptin on testicular testosterone secretion [23]. Similarly, suppression of luteinizing hormone surge has been reported in leptin receptor-deficient obese Zucker rats [24] and neuronal leptin receptor deleted mice [25]. Moreover, human chorionic gonadotropin-stimulated testosterone secretion is suppressed in obese men [26].
Another mechanism for the low testosterone levels seen in obesity is that elevated aromatase by hypertrophied adipose tissue increases the conversion of testosterone to estradiol and elevated estradiol suppresses GnRH in the hypothalamus via a negative feedback mechanism [27].
In an epidemiology study, Knoblovits et al [28] studied the relationship between obesity and testosterone level and reported that body mass index (BMI) is negatively associated with the free testosterone level and erectile function. Moreover, testosterone replacement for 5 years has shown a progressive and sustainable reduction of body weight in obese subjects with hypogonadism [29], suggesting a close association between obesity and testosterone levels.
2. Endothelial dysfunction and insulin resistance
Another connection between obesity and ED is endothelial dysfunction due to obesity-associated derangements, such as elevated FFA level, adipokines, inflammation, and oxidative stress, and insulin resistance. The main features of endothelial dysfunction are reduced production of nitric oxide (NO), which result in difficulties in the smooth switch of vessels between dilation and constriction [30]. Chronic high-fat feeding induces endothelial dysfunction and ED in rodents [5]. We also previously demonstrated that high-fat feeding decreases penile eNOS expression in rats [31], and palmitate induces endothelial cell damage through reactive oxygen species (ROS) generation in vitro [32]. Taken together, the elevated FFA levels associated with high-fat feeding induces ROS elevation and NOS suppression via the downregulation of 5′-adenosine monophosphate-activated protein kinase (AMPK)-phosphatidylinositol 3-kinase (PI3K)-eNOS pathway in the endothelium and results in decreased NO generation [30].
A possible process for induction of inflammation by elevated FFA is that FFA activates Toll-like receptors, an innate immune receptor, and trigger intracellular signaling molecules, such as myeloid differentiation primary response gene 88 and nuclear factor κB; a transcription factor for pro-inflammatory cytokines, and consequentially produces inflammatory cytokines [3334], which suppress eNOS/NO pathway [35], then leads to endothelial dysfunction. Consistently, a human study demonstrated that C-reactive protein, a systemic inflammatory marker, is higher in obese men with ED than in obese men without ED and is correlated with the severity of ED [36]. These are supported that antiinflammatory agent protects ED in diabetic rats [37] and improves erectile function scores in a human study [38].
Adipokines are adipose tissue-driven cytokines. They involve various metabolic processes, such as energy metabolism, inflammatory response, and vascular function. In an obese state, adipokines are hyper- or hyposecreted and have a pro- or anti-inflammatory effect on vascular endothelium. This dysregulation of adipokine production results in the generation of ROS and induces endothelial dysfunction. Tumor necrosis factor-alpha (TNF-α) and interleukin-6 are major pro-inflammatory cytokines produced by hypertrophied adipocytes. They induce inflammatory gene transcript in endothelial cells [39] and suppresses eNOS expression [40]. Corpora cavernosa from TNF-α-infused mice shows attenuated nonadrenergic-noncholinergic nerve-mediated relaxation and suppressed eNOS and nNOS gene expression [41]. Moreover, TNF-α depleted mice show increased endothelium-dependent relaxation in isolated corpora cavernosa and elevated eNOS and nNOS expression [42]. In human studies, plasma levels of these inflammatory cytokines are correlated with BMI and generate inflammatory reaction and insulin resistance [43] and high levels of TNF-α were significantly associated with ED [44].
Adiponectin, one of the most abundant hormones produced mainly by adipose tissue, is differently regulated by obesity than other adipokines, and the concentration is decreased in an obese state [45]. Adiponectin has anti-diabetic, anti-inflammatory, anti-atherogenic effects, as well as insulin-sensitizing effects on the vascular endothelium [46]. Adiponectin attenuates the production of ROS induced by palmitate in endothelial cells [47]. Adiponectin also increases phospho-eNOS in endothelial cells, and adiponectin knockout mice have shown impaired endothelium-dependent vasodilation [48]. Thus, decreased adiponectin levels in obesity induce insulin resistance, proinflammatory activation, and finally endothelial dysfunction. These alterations of adipokines are strongly associated with obesity because weight reduction from exercise, diet, or surgery reverses these pathological conditions [4950].
Insulin induces vasodilation through increased expression of eNOS and NO production via the activation of PI3K-Akt pathways [51]. Thus insulin resistance, which is commonly associated with obesity, plays a role between obesity and NO deficiency [52]. This is supported by a human study that demonstrated obesity without insulin resistance preserved endothelial function while insulin-resistant obese individuals had endothelial dysfunction [53]. A clinical study also showed that insulin resistance is an independent determinant of ED in young adult men [54]. Insulin resistance elevates oxidative stress and inflammatory cytokines in endothelial cells, which decreases NO bioavailability, and induces endothelial dysfunction [5556].
Go to :
ERECTILE DYSFUNCTION
ED is a frequent medical consequence in the elderly. Its pathologic features are classified as psychogenic and organic in origin. Organic ED is vasculogenic, neurogenic, anatomic, and endocrinologic origin. Vasculogenic ED, the most common form, mainly results from endothelial dysfunction. Moreover, cases of vasculogenic ED have been shown to be more closely associated with obesity and associating hormonal alterations, compared with other cases of ED [57]. PDE5 inhibitors are the most widely prescribed medicine for patients with ED. Currently available PDE5 inhibitors are sildenafil (Viagra; Pfizer, New York City, NY, USA), vardenafil (Levitra, Staxyn), tadalafil (Cialis; Eli Lilly), avanafil (Stendra; VIVUS Inc., Campbell, CA, USA), udenafil (Zydena; Dong-A PharmTech, Seoul, Korea), and mirodenafil (Mvix; SK Chemical, Seongnam, Korea) [58].
As described above, ED is associated with obesity and its concomitant metabolic derangements. High-fat diet-induced obese rodents are commonly used as an animal model for ED [59], whereas acute correction of obesity by bariatric surgery improves ED [911]. These findings suggest a causal relationship between obesity and ED.
In a study from Slovakia, 73% of men older than 40-years-old with abdominal obesity had some degree of ED [60]. In another study, 79% of men presenting with ED had a BMI of 25 kg/m2 or higher and obese men, over 30 kg/m2, had 3 times greater risk for sexual dysfunction than the general population [61]. Furthermore, the degree of ED in obese patients is more severe than that in non-obese patients, resulting an increased refractory rate to PDE5 inhibitors in severely obese patients [15]. According to a meta-analysis, the overall refractory rate for sildenafil, tadalafil, and vardenafil is 30% to 35%, which is reduced to less than 20% when improving comorbid conditions [62].
Go to :
COMBINED TREATMENT WITH METFORMIN AND PHOSPHODIESTERASE 5 INHIBITORS
As described above, obesity and ED may share common features including obesity-associated metabolic alterations. Among them, insulin and leptin resistance are central pathologic conditions inducing ED [63]. Their amelioration would be helpful to treat patients with ED. Metformin originally was developed as an insulin sensitizer six decades ago. Currently, it has been reported that metformin also improves leptin resistance [186465]. Therefore, metformin has become a strong candidate to normalize obesity-associated pathologic internal environments and resulting potentiation of the efficacy of ED treatment with PDE5 inhibitors. In this aspect, we discuss combined treatment of metformin and PDE5 inhibitors.
1. Metformin's effect on erectile dysfunction
Metformin is an anti-diabetic agent that been shown to have anti-inflammatory [66] and anti-obesity effects [186465]. Although Rey-Valzacchi et al [67] hypothesized that its beneficial effect on cavernosal NO signaling resulted from improving metabolic profile, the vascular change by metformin was induced even when there is no significant glycemic control effect by metformin in streptozotocin-diabetic rats [68]. This suggests that metformin has a primary and secondary effect on vessels.
The major target molecule of metformin is AMPK, a cellular energy sensing molecule activated under an energy deprivation state. Although the molecular mechanism of metformin is not completely understood, AMPK has been shown to mediate diverse biological effects on the endothelium, such as activating NOS [31], reducing oxidative stress [32], elevating FFA oxidation, and suppressing endoplasmic reticulum stress [69]. Chantler et al [70] also demonstrated that metformin preserved the bioavailability of vascular NO in the abdominal aorta of obese Zucker rats by improving insulin resistance, which is a cause of NO deficiency [2]. In another study, metformin was shown to reverse intracavernosal muscle tone and elevate eNOS phosphorylation in an angiotensin II-induced ED model [71].
Because obesity is frequently associated with a chronic low-grade inflammatory state and related conditions, including ED and atherosclerosis, suppression of inflammation may improve ED. Rodent and human studies have reported that metformin has positive effects on the endothelium. In particular, Jing et al [72] presented that metformin improves obesity-associated inflammation by altering macrophage polarization. Metformin may protect against coronary atherosclerosis in prediabetes and early diabetes mellitus among men [73]. Silva et al [74] reported that metformin improves ED in obese mice by improving in vitro endothelial and nitrergic cavernosal relaxation. Vignozzi et al [75] reported that metformin increases adenosine signaling in HF-fed rabbits. Vitale et al [76] demonstrated that metformin improves endothelial-dependent vasodilation in patients with metabolic syndrome. Moreover, Giagulli et al [77] have shown that metformin treatment combined with testosterone boosts erectile function in patients with obesity and hypogonadism.
2. Systemic beneficial effects of phosphodiesterase 5 inhibitors
PDE5 inhibitors are widely prescribed for the treatment of patients with ED. PDE5 inhibition prevents the degradation of cyclic guanosine monophosphate and elevates NO bioavailability [78]. In addition, numerous studies have reported that PDE5 inhibitors have beneficial systemic effects. It is well established that PDE5 inhibitors have anti-inflammatory effects based on studies ranging from rodents to humans [798081]. Nunes et al [80] suggested that AMPK, a major target molecule of metformin, was associated with the anti-inflammatory effects seen in sildenafil. Santi et al [81] demonstrated that PDE5 inhibition improves endothelial inflammatory parameters in patients with diabetes and ED. De Toni et al [82] reported that vardenafil elevates mitochondrial biogenesis via the activation of peroxisome proliferator-activated receptor-γ and adiponectin in human adipose tissue ex vivo.
Moreover, sildenafil therapy lasting 12 weeks reduced visceral fat in humans and murine models of diabetes [83]. PDE5 inhibition in sildenafil also enhances insulin sensitivity in human umbilical endothelial cells [84] and overweight individuals with prediabetes assessed by the hyperglycemic clamp technique [85]. Although Ho et al [86] fail to show improvements in insulin resistance with tadalafil in obese individuals, they demonstrate a favorable effect on β-cell compensation by tadalafil.
Recently we also demonstrated that udenafil has weight loss effects in high fat-fed obese mice and directly suppresses hypothalamic Toll-like receptor 4, a receptor trailing proinflammatory responses and activated by long chain fatty acids [34]. Furthermore, it was reported that PDE5 inhibitors lowered the risk of overall mortality in patients with type 2 diabetes in a retrospective cohort study [87].
3. Combination of phosphodiesterase 5 inhibitors and metformin
It has been established that obesity and ED share an internal pathological environment, thus, targeting obesity as an underlying factor of ED may be an important therapeutic approach to maximize the efficacy of treatment. Moreover, once daily prescription for a long time with low dose PDE5 inhibitors is settled down as a trend of ED treatment currently [78]. It has become increasingly important to focus on the systemic and metabolic effects of PDE5 inhibitors, especially in patients with ED and comorbid medical conditions. Combination therapy would be helpful and efficient in this respect.
Although data on the clinical effect of combined treatment of metformin and PDE5 inhibitor are lacking, several studies have evaluated the combined effects of metformin and PDE5 inhibitors. In a prospective, randomized, double-blind study, researchers demonstrated that the addition of metformin to sildenafil improved erectile function in patients with ED, a poor response to sildenafil, and insulin resistance [67]. They postulated that the beneficial effects of metformin result from the improvement of insulin resistance because PDE5 inhibitors require adequate levels of NO to be effective and insulin resistant states have decreased NO levels. Similarly, Giagulli et al [77] reported that combined treatment metformin with testosterone improves ED considerably and lowers body weight in men with diabetes who are obese. Park et al [3] observed that atorvastatin partially improves erectile function in streptozotocin-induced diabetic rats and recommended combination therapy to treat severe diabetes-associated ED.
However, an animal study demonstrated that sildenafil blocked metformin's vasodilatory effect in freshly-isolated rat tail arteries [88]. Another combination treatment with anti-hypertensive drugs was shown to not significantly affect the efficacy of udenafil [89].
Further study is needed to evaluate the combination treatment with PDE5 inhibitors and metformin.
Go to :
CONCLUSIONS
To maximize the efficacy of treatment in patients with ED who are obese, managing obesity as an underline disease for ED is an important therapeutic approach because obesity and ED share an internal pathological environment. The long-term once daily administration of low-dose PDE5 inhibitors rather than on demand prescription has recently become popular. Thus, we have to focus on the systemic and metabolic effects of PDE5 inhibitors and recommend combination therapy.
Although there is not enough research to evaluate the clinical effect of combined treatment of PDE5 inhibitors and metformin in patients with ED who are obese, several studies have reported optimistic outcomes, and combination therapy is strongly recommended especially in severe systemic disease-associated ED. Further studies are warranted.
Go to :
 XML Download
XML Download