

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Metabolic syndrome (MetS) describes a cluster of abnormalities including obesity, dyslipidemia, hypertension, and insulin resistance. Its discovery goes back to early twentieth century when Kylin [1] first described a combination of metabolic disturbances, namely hypertension, hyperglycemia and gout. In the 1940s, Vague [2] noticed an association between upper body adiposity, hypertension and diabetes, which allowed Haller and Hanefeld [3], in 1975, to coin the term MetS, defining it as a combination of simultaneous risk factors (diabetes, cardiovascular disease) that are hazardous to human health. Other nomenclatures came out in later years such as Syndrome X (1988) [4], the Deadly Quartet (1989) [5], and the Insulin Resistance Syndrome (1992) [6]. Nevertheless, disparity still exists regarding the exact diagnostic criteria used to define MetS; therefore guidelines proposed by the International Diabetes Federation (IDF) [7], National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) [8] and World Health Organization (WHO) [9] are commonly utilized to recognize this condition in clinical practice (Table 1).
The systemic nature of MetS motivated the investigation of its deleterious effects once it may potentially affect many aspects of human physiology. Male infertility is one condition that can be influenced by the subject's metabolic status. Recent evidence suggests that a direct association between the different components of MetS and sperm production and function exist. Infertility affects about 15% of couples attempting to conceive after 1 year of regular unprotected intercourse. Male factor contributes to 20% to 50% of the causes of infertility among couples. The increase in the prevalence of MetS perceived in recent years has coincided with a decrease in semen quality among adult males. It is therefore intuitive to investigate the available literature linking these two conditions together, which was the primary objective of this review article.
DEFINITIONS AND EPIDEMIOLOGY OF METABOLIC SYNDROME
Various definitions for MetS exist and all of them are based on physiological parameters, such as obesity, glucose and lipid blood levels, and blood pressure [7891011] (Fig. 1). The WHO first developed its definition in 1998 [12]. Because insulin resistance was felt to be central to the pathophysiology of MetS, evidence for insulin resistance is an absolute requirement in the WHO definition, without it, even if all the other criteria were met, the patient would not have MetS (Table 1). The NCEP ATP III [8] criteria classifies an individual with MetS when he presents with three of the 5 components described in Table 1. MetS, according to IDF [7], is met when an individual presents with central obesity (high waist circumference [WC]) plus any two of the criteria present in Table 1.
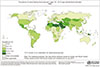
The absence of a standardized definition for MetS is one of the reasons why it became difficult to have a clear estimate about its prevalence. Representations of the global patterns of the components of MetS in males has been published by the WHO (Fig. 2, 3, 4, 5). These metabolic derangements are influenced by lifestyle factors, age, sex, and race and are increasing worldwide, thus becoming a subject of concern and an object of research.
When analyzing the prevalence of MetS, it is necessary to take many factors into account. In younger generations, the prevalence of MetS is mainly influenced by the adopted diagnostic criteria followed by age and ethnicity (for review [13]). The prevalence of MetS is inversely related to the education level, the lifestyle (high fat diet and lack of exercise) and socioeconomic status. Rapid urbanization has been considered a principle factor for the increasing incidence of MetS (for review [13]). It is currently believed that approximately one in five US adults meet the criteria for MetS [14]. The prevalence of MetS worldwide can go from <10% to 84%; this high variation is dependent on the geographic localization, age, race, and ethnicity, as well as the accepted definition [15]. Moreover, all the already mentioned factors, genetic background, family history of diabetes and smoking are additional risk factors that influence the prevalence of MetS and its components [15].
THE LINK BETWEEN METABOLIC SYNDROME AND MALE FERTILITY
Although each disease that is part of MetS definition has effects on male fertility separately, when put together, these metabolic elements can have additive effects on fertility. Studies exploring the effects of MetS on male fertility are recent (Fig. 6). In 2013, Lotti et al [16] studied the association between MetS and clinical characteristics of men of infertile couples. In this study, an age-adjusted model showed that MetS was associated with a decline in total testosterone without alterations in gonadotropin levels. The same study reported a negative correlation between the number of MetS components and progressive motility as well as normal morphology in a univariate analysis; however, adjusting the study for age and total testosterone, only normal morphology showed the same negative correlation. The risk of erectile dysfunction (ED) increased with the number of MetS factors, even after adjusting for age and testosterone levels. This study demonstrated an association between MetS and the presence of hypogonadism, decreased normal sperm morphology and ED in men of infertile couples. The same group, one year later [17], explored the association between MetS and prostatic abnormalities in infertile men. In an age adjusted model, the authors identified that insulin levels increased as a function of MetS components and showed an inverse correlation with total testosterone levels. This study also reported a negative correlation between MetS components and normal sperm morphology and a positive correlation between MetS components and interleukine-8 (a prostate inflammation marker), prostate total and transitional zone volume, arterial peak systolic velocity, texture homogeneity and calcification size in an age-testosterone-insulin adjusted model. Leisegang et al [18] compared male patients, with and without MetS, and reported lower sperm concentration, total sperm count, total motility, sperm viability, mitochondrial membrane potential, free testosterone and progesterone levels, and higher sperm DNA fragmentation in men with MetS. In 2016, Ventimiglia et al [19] examined men presenting with primary infertility with or without MetS according to the NCEP-ATPIII criteria. Compared with infertile men without MetS, infertile men with MetS were more likely to be hypogonadal, had lower levels of total testosterone sex hormone-binding globulin (SHBG), inhibin B and anti-Müllerian hormone (AMH). However, no differences were found in semen parameters between the two groups [19]. On the other hand, a recent study compared semen and hormone parameters of fertile men to infertile men. Except for a significant negative association between MetS and total testosterone levels in both groups, the authors failed to reproduce a significant independent effect for MetS on major fertility parameters of both groups [20]. These studies suggest that MetS may carry a detrimental effect on important reproductive functions such as endocrine status or semen parameters and call for the development of further research of superior design to accurately determine this association.
OBESITY AND MALE FERTILITY
1. An overview on obesity
Obesity is classified according to body mass index (BMI) which was promoted by Ancel Keys in 1972 and describes a person's leanness based on their height and weight (weight per height squared, kg/m2) [21]. The WHO defines overweight and obesity when the BMI is ≥25 kg/m2 and ≥30 kg/m2, respectively [22]. Obesity is further divided into three classes; class I (BMI, 30.0–34.9 kg/m2), class II (BMI, 35.0–39.9 kg/m2), and class III (BMI, ≥40.0 kg/m2) [2123]. Obesity can also be diagnosed based on abdominal fat defined as WC ≥102 cm for men and WC ≥88 cm for women [24]. The origin of obesity is multifactorial, and involves an interaction between the environment, genetic backgrounds, and hormones [25]. Many hormones are involved in the patho-etiology of obesity especially that the adipose tissue is now recognized as an endocrine organ with its excess being a cause for comorbidities (Fig. 1) [26]. Obesity results from excessive accumulation of adipose tissue and consequently weight gain, because of an imbalance between energy intake and expenditure [2627].
Leptin, a hormone produced by the adipose tissue [28], regulates energy homeostasis [29] and is an essential intermediary of inflammation in obesity [30]. Obese men develop leptin resistance and hence have high levels of leptin in their circulation [31]. Ghrelin, a hormone secreted by the stomach, is responsible for regulating appetite [32] and is negatively correlated with BMI, meaning that it is lower in the obese [32]. Peptide YY (PYY), glucagon like peptide-1 (GLP-1), and cholecystokinin (CCK) are produced by the gastrointestinal tract after food intake [21], augmenting satiety [33]. Obese people secrete lower levels of PYY, GLP-1, and CCK in comparison to people with normal weight [3435] (Fig. 1).
The hormonal disturbances causing obesity can have genetic and congenital backgrounds, such as Prader-Will syndrome, leptin deficiency, and Cohen syndrome among others. The ingestion of extreme amounts of food increases inflammation [36], which is also observed with the excessive consumption of salt, sugars, alcohol, and fats [37]. This, coupled with smoking and lazy lifestyle, places obese people at risk for a number of chronic diseases, such as hypertension, cancer, and diabetes. The increase in the BMI has been associated with an increase in risk of developing myeloma, leukemia, rectum, thyroid, kidney, colon, and esophageal cancer [38].
2. The link between obesity and male fertility
Recent reports showed a relationship between an increase in obesity rates and a decrease in birth rates. The effects of overweight and obesity on male fertility is a hot topic in our days with a good number of studies reporting significant effects of excessive weight on semen parameters and/or hormonal profile of men (Fig. 1).
A systematic review of 21 cross-sectional and prospective cohort studies originating from 12 countries and including a total of 13,077 individuals recruited from the general population or fertility clinics was conducted to assess the relationship between sperm count and BMI. The authors found a J-shaped association between BMI and abnormal sperm count. Compared with men of normal weight, the odds ratios (95% confidence interval) for oligozoospermia were 1.11 (1.01–1.21) for overweight men, 1.28 (1.06–1.55) for obese men, and 2.04 (1.59–2.62) for morbidly obese men. This meta-analysis quantifies a two-fold increase in risk of oligozoospermia in morbidly obese men [39]. More recent studies have also confirmed this negative association between BMI and various semen parameters. Tang et al [40] assessed the correlation between BMI and semen analysis parameters of infertile patients finding a significant negative correlation between BMI and sperm motility. Another study of similar design reported significant negative correlation between BMI and sperm concentration [41]. Bieniek et al [42] conducted a multi-institutional study including infertile men looking for a relationship between semen and hormone parameters and the patients' BMI. The authors found a significant inverse relationship between BMI and sperm concentration, sperm morphology, total testosterone, and testosterone: estradiol ratio. Studies exploring the impact of BMI on advanced sperm function test also have yielded detrimental effects where a significantly increased rate of sperm DNA damage and lower mitochondrial activity have been observed in obese men compared with men of normal weight [4344]. Furthermore, the impact of obesity on sex hormone levels has been more evidently acknowledged with a negative correlation between total or free testosterone [454647], luteinizing hormone (LH) [4546], SHBG [4647], inhibin B [47], and AMH [47] and increasing BMI have been reported.
Overall, a clear association between altered sperm parameters, DNA fragmentation and fluctuations in hormonal levels and obesity was detected by several studies. The effects of obesity on male fertility and sperm functions can occur as a consequence of several mechanisms: i) an imbalance between testosterone and estradiol ratio and consequently other sexual hormones due to the excessive aromatization in adipocytes; ii) excessive inflammation and oxidative stress resulting from the high levels of adipokines and toxins in adipose tissue of obese men; iii) increase of gonadal temperature due to an accumulation of fat tissue in the scrotal region impairing spermatogenesis; iv) dysregulation of several hormones, such as leptin that can alter the hypothalamus-pituitary-gonad (HPG) axis (Fig. 1, 6).
The maintenance of testosterone levels is crucial for male fertility status (Fig. 6). The link between obesity and testosterone deficiency is supported by many studies [454647]. Testosterone levels in obese males are commonly related with levels similar to hypogonadal men [2148]. In obese men, an increase in the activity of aromatase enzyme in the adipocytes results in the peripheral conversation of testosterone into estradiol [2148]. Once the levels of estradiol rise, a negative feedback on LH secretion is observed, leading to the suppression of the HPG axis and consequently a reduction in testosterone production by Leydig cells [48]. Estradiol also plays a critical role in the development of germ cells and variations in levels of estrogen can affect spermatogenesis (for review [49]). Adipocytes are the main producers of leptin, and this hormone per se affects LH and follicle-stimulating hormone (FSH) release from the pituitary, altering not only the amplitude of the released pulses, but also the pulsatility; this affects the balance of the HPG axis in case of excess of adipose tissue [5051]. The deposition of fat tissue around the scrotal vessels can reduce spermatogenesis in obese men decreasing blood cooling and consequently increasing testicular temperature [5253]. The relationship between scrotal lipomatosis and male infertility was described in a study that confirmed a diffuse pattern of fat deposition around the structures of the spermatic cord in obese men [52]. Another study showed an improvement of sperm quality after a scrotal or suprapubic lipectomy [53]. More recent studies explored the connection between oxidative stress and the fertility status of obese men. Oxidative stress is an acknowledged cause of sperm dysfunction as it causes sperm membrane lipid peroxidation, DNA fragmentation, and aggravates apoptosis [54]. Obese men are particularly prone to oxidative stress. The excess in adipose tissue is associated with an increase in local and systemic production of pro-inflammatory adipocytokines [55], which induce the production of reactive oxygen species (ROS). Furthermore, increased oxidative stress leads to important changes in adipose tissue, promoting a systemic low-grade inflammatory response with adverse effects throughout the body including the reproductive tract (for review [56]). Finally, ED is another important factor to consider in patients seeking fertility. Obese men are at higher risk of ED [57] due to lower testosterone levels and high levels of inflammatory factors [5859].
GLUCOSE METABOLISM AND MALE FERTILITY
1. An overview on the impairment of glucose metabolism
The maintenance of plasma glucose is crucial for the physiological functions of the body. Glucose is the sole energy fuel for cells protected by blood-barriers, such as the brain [60] and testes [61]. The diagnosis of glucose impairment is achieved through monitoring glucose levels in blood stream, such as measuring the fasting glucose or with an oral glucose tolerance test. For the measurement of fasting glucose, the cut point for prediabetes is 100–125 mg/dL, while that for diabetes mellitus (DM) is ≥126 mg/dL [62]. After an oral glucose tolerance test, prediabetes is diagnosed when the blood sugar is 140–199 mg/dL and DM is diagnosed when the blood sugar is ≥200 mg/dL [62]. Hypoglycemia is defined as abnormally low glucose concentration that is harmful for the patient with values <70 mg/dL considered alerting. On the other hand, hyperglycemia is detrimental to human health as a slight increase in plasma glucose concentrations can raise the risk of cardiovascular diseases. While obesity is considered a major risk factor for dysregulation of glucose metabolism, other environmental and genetic factors can also contribute to this condition [63]. Impairment of glucose metabolism is a key component of MetS. Insulin is the principle regulator of glucose metabolism. This hormone is produced by the pancreatic β-cells to facilitate uptake of glucose from the blood stream into cells and tissues. Insulin resistance is defined as the reduced sensitivity of cells to stimulation by insulin in normal or elevated levels of glucose. As a result, the pancreas will secrete more insulin, resulting in a state of hyperinsulinemia. With continued insulin resistance, hyperglycemia ensues, causing glucose intolerance and finally type 2 DM (T2DM) (for review [63]).
2. The link between impairment of glucose and male fertility
Similar to obesity, studies demonstrated a correlation between the increase in the incidence of DM and a decrease in the fertility rates [64]. A study comparing patients with T2DM to non-diabetic men attending a fertility clinic showed lower progressive motility and an increase in sperm DNA fragmentation in diabetic patients [65]. Also the clinical pregnancy rate and the miscarriage rate was higher when the male partner was diabetic [65]. Another study of similar design also confirmed the presence of lower sperm concentration and total count in semen of diabetic patients compared with healthy individuals [66]. A study conducted in normozoospermic T2DM and non-diabetic men detected higher levels of malondialdehyde, a marker of oxidative stress, in diabetic patients that was consistent with lower sperm concentration, motility and normal morphology in this group compared with non-diabetic men [67]. In addition to the negative effects on sperm count, motility, and DNA integrity, lower ejaculate volumes were also observed in diabetic men [68]. The aforementioned studies provide solid evidence on the negative effects of diabetes on male fertility. The pathophysiology of these effects have been studied in a number of human and animal models and are believed to occur secondary to alterations in testicular environment, testosterone homeostasis, ejaculatory function, and libido (for review [69]).
Testicular environment is highly controlled by glucose homeostasis that can be deregulated in DM thereby impairing spermatogenesis [7071]. Animal studies reported excessive damage to seminiferous tubules early in the development of DM impairing the gonadosomatic index, as well as sperm quality [72]. Experimental induction of DM in mice resulted in enhanced lipid peroxidation in testis (cytosol and mitochondria) and epididymal sperm and increased ROS production as early as 5 days following the experiment [73]. This suggests that oxidative stress is increased in diabetes due to overproduction of ROS. Associated with the ROS generation is a decreased efficiency of antioxidant defenses, which is a process that starts very early and worsens over the course of the disease. Many studies have focused on the derangement in testosterone levels in men presenting with DM (Fig. 6). A cause-effect relationship exists between testosterone and DM where lower levels of testosterone are typically present in diabetic men, increasing the risk for developing T2DM occurs when testosterone concentrations are low (for review [74]). This is because testosterone improves insulin sensitivity and hence glucose homeostasis. Testosterone is also an important regulator of spermatogenesis as a number of genes and kinases on Sertoli cells are directly influenced by testosterone levels [75]. Therefore, the decreased testosterone levels could help explain the alteration in sperm production seen in diabetic patients. Sexual dysfunctions such as erectile and ejaculatory dysfunction as well as decreased libido are common in patients with DM [76]. Retrograde ejaculation (RE) occurs as a consequence of a diabetic autonomic neuropathy [77]. It has a devastating effect on male fertility potential as it decreases the ejaculate volume and hence the sperm quantity. The sympathetic nervous system plays an important role during emission and expulsion phases of ejaculation. It orchestrates smooth muscle contraction of the seminal vesicles and ejaculatory ducts and simultaneously ensures bladder neck closure to prohibit retrograde flow of semen into the bladder. Sympathetic nervous system dysfunction has been detected in patients with DM resulting in RE (for review [78]). One study reported the presence of RE in 34.6% of diabetic men in comparison to 0% in non-diabetic men, demonstrating the presence of aspermia in diabetic men with RE [77]. ED is more prevalent in diabetic men compared with the general population [79]. Diabetic patients are prone to neurovascular alterations which can induce impairment of the endothelial function of the corpus cavernosum and therefore result in organic ED [8081]. Endothelial dysfunctions are a reflection of decrease/loss of nitric oxide (NO) biological activity and/or biosynthesis at endothelial level [82]. Although, in diabetic men, the pathogenic mechanisms of endothelial function still remain unclear; impairment of NO activity, an essential molecule for penile vascular and cavernous smooth muscle activity has been observed in diabetic men [83].
DYSLIPIDEMIA AND MALE INFERTILITY
1. An overview on dyslipidemia
Dyslipidemia is defined as the abnormal amount of lipids including triglycerides, cholesterol, and fat phospholipids in the blood steam (Fig. 1). It can occur primarily due to several genetic disorders or secondary to environmental factors or other diseases. The elevation of biochemical makers in blood analysis such as total cholesterol and low-density lipoprotein cholesterol (LDL-C) received more attention as they are particularly sensitive to lifestyle changes [84]. Other biochemical markers of importance in dyslipidemias are the very low density lipoproteins (VLDL), triglycerides, and the high-density lipoprotein-cholesterol (HDL-C) levels [84]. The production of lipoproteins is regulated by substrate supply and hormonal levels. Insulin and glucagon are essential hormones involved in the regulation of lipoprotein production [85]; however the exact role of these hormones remains to be elucidated. On the other hand, the availability of substrates regulates gene expression in lipid metabolism. Some transcriptional factors such as hepatic nuclear factor, retinoid X receptor, peroxisome proliferator activated receptor, were identified as targets for fatty acids (for review [86]). Screening of the lipid profile is recommended for men over the age of 40 years, individuals presenting risk factors for atherosclerosis, such as diabetes, hypertension, obesity, some autoimmune chronic inflammatory conditions, among other medical conditions, and in case of hereditary dyslipidemia. Assessing the lipid profile is a method of dyslipidemia evaluation, which encloses the determination of total cholesterol, LDL-C, apolipoprotein B, non-HDL-C and triglycerides.
2. The link between dyslipidemia and male fertility
The role of cholesterol in post-testicular modification of sperm plasma membrane composition and dynamics is essential for fertility; however, the impact of high cholesterol and other dyslipidemias in fertility remains to be elucidated (Fig. 6). Aiming to evaluate the association between men's serum lipid concentrations and semen quality parameters, Schisterman et al [87] examined semen samples from male partners of couples desiring pregnancy. The authors detected higher levels of serum total cholesterol, free cholesterol, and phospholipids in patients with a significantly lower percentage of spermatozoa with intact acrosome and smaller sperm head area. In another study, the same authors observed higher levels of cholesterol in couples who had a significantly longer time to conception [87]. Hagiuda et al [88] assessed the relationship between dyslipidemia and sperm quality and serum hormone levels in male patients in Japan. Serum triglyceride level had a positive association with sperm morphologic traits and a negative association with serum testosterone level. Another study reported that VLDL, in addition to serum triglycerides, had an inverse relationship with sperm motility proposing that these lipids, in excess, may have deleterious effects on spermatogenesis [89]. Oxidative stress, which often accompanies the derangement in serum lipid concentration, may be the driving force behind the impact that dyslipidemia has on male fertility. This hypothesis was supported by the work of Shalaby et al [90] who examined the effects of highcholesterol diet and anti-cholesterol therapy on male rat fertility. The authors demonstrated significant decline of fertility, testicular weight, and sperm parameters in male rats fed with a high-cholesterol diet compared to a cholesterol-free diet. Male rats on a high-cholesterol diet were then treated with no-intervention, alpha-tocopherol (an antioxidant), simvastatin (a lipid-lowering agent), or both therapeutic agents. Treatment with alpha-tocopherol, simvastatin, and the two in combination significantly increased testicular weight and sperm parameters together with an improvement in fertility index (mating success rate). This improvement was more prominent with combination therapy compared with both individual therapies. The authors not only demonstrated decreased fertility with a high-cholesterol diet, but they also showed therapeutic gain in fertility with antioxidant and lipid-lowering agents.
HYPERTENSION AND MALE INFERTILITY
1. An overview on hypertension
Hypertension, a disease of the vascular system, results from the improper functioning of the arterial pressure control mechanisms. Hypertension is diagnosed when systolic pressure >140 mmHg or diastolic pressure >90 mmHg during repeated measurements of blood pressure. Hypertension can be classified into different grades, according to the European Society for Hypertension/European Society for Cardiology where grade 1 is considered when the systolic pressure is 140–159 mmHg and the diastolic pressure is 90–99 mmHg; Grade 2 when the systolic pressure is 160–179 mmHg and the diastolic pressure is 100–109 mmHg; Grade 3 when the systolic pressure is ≥180 mmHg and the diastolic pressure is ≥100 mmHg [91]. Hypertension is a multifactorial disease, and the development of this condition has some risk factors such as: food habits, lifestyle, ethnic, and genetic predisposition.
2. The link between hypertension and male fertility
Existing data suggest an association between hypertension and impaired semen quality. Guo et al [92] revealed that men with hypertension had lower semen volume, motility, total count, and total motile count when compared with men without hypertension. In an attempt to study the relationship between semen quality and current health status, Eisenberg et al [93] described higher rates of semen abnormalities in men with diseases in the circulatory system particularly hypertensive disease, peripheral vascular disease, and non-ischemic heart disease. Such an association was not thoroughly investigated and the direct end-organ effects of hypertension on the testes is not well characterized. Theories linking hypertension with reproductive dysfunction are mainly based on endocrine derangements or ED that may accompany this disease. A cross-sectional study identified a negative correlation between testosterone and systolic blood pressure [94]. This finding was replicated in another case-control study by Fogari et al [95] who quantified a 10% reduction in total testosterone levels in hypertensive men compared to normotensive men. ED is more prevalent in hypertensive men with a 2-fold increased risk than the general population [969798]. The causes are related to structural lesions that result from high blood pressure in penile arteries which are aggravated by atherosclerosis resulting in impairment of blood flow [99100]. Again, compelling evidence linking hypertension to impairment in testicular function is still lacking and requires further experimental research.
DOES THE TREATMENT OF METABOLIC SYNDROME AFFECTS FERTILITY?
Weight loss through adoption of a healthy lifestyle in addition to regular physical activity is the cornerstone treatment for MetS. An improvement in sperm quality is expected as weight reduction would alleviate the previously mentioned deleterious effects of obesity on human reproduction. This belief has been proven in studies that explored the effect of natural weight reduction on male fertility. Håkonsen et al [101] studied semen samples men with BMI >33 kg/m2 who underwent a 14-week weight loss program. Following the intervention, the median percentage weight loss was 15%. An increase in total sperm count, semen volume, testosterone, SHBG, and AMH were also observed. A larger study by Jaffar [102] included obese men who underwent diet counselling and exercise resulting in mean BMI loss of 2.2 kg/m2. The author observed a significant positive correlation between weight loss and percentage of progressive sperm motility and static percentage. On the other hand, the effect of weight loss following bariatric surgery on semen parameters and male fertility is still controversial with some studies reporting no or worse influence while others finding an improvement in semen parameters following bariatric surgery. The imbalance in electrolytes and nutrients observed after these mal-absorptive surgeries may explain the observed worsening in semen parameters that occur shortly after surgery [103104]. However, newer evidence detected significant improvements in semen parameters with longer periods of follow-up after surgery [105].
CONCLUSIONS
MetS is increasing worldwide almost approaching the pandemic state. Its key components, namely, obesity, insulin resistance, dyslipidemia, and hypertension can have detrimental effects on various aspects of human health. Male fertility is one condition that can be influenced by MetS through several mechanisms. Endocrine system dysregulation, scrotal temperature elevation, oxidative stress, and alteration of the erectile and ejaculatory functions are well recognized MetS consequences that can impair sperm production and function, ultimately affecting male fertility. A healthy lifestyle characterized by good nutrition and regular physical activity is key to prevent the unwanted effects of MetS not only on fecundity but also on health and well-being overall.






 XML Download
XML Download