

 Citation
Citation Print
Print



INTRODUCTION
Diabetes is a global health emergency. One in 11 adults has diabetes, with 5 million diabetes-related deaths having occurred in 2015.1 In Korea, the prevalence of diabetes has increased drastically from 1.5% in the 1970s to > 10% in the early 2000s.2 According to the Korea National Health and Nutritional Examination Survey (KNHANES [2013–2014]) results, approximately 4.8 million Koreans (13.7%) aged 30 years or older have diabetes, and nearly 25% of adult Koreans are prediabetic.3 Diabetes is frequently associated with complications such as retinopathy, renal failure, neuropathy, nephropathy, cardiovascular disease, and amputations.4 Diabetic retinopathy (DR) is the leading cause of preventable vision loss in working-age adults in developed countries and has a global prevalence of 35.4%.56 According to earlier KNHANES (2008–2011) results, 15.8% of diabetic patients in Korea have DR, 2.8% of whom also have diabetic macular edema (DME), an advanced and severe form of DR.78 The worldwide increase in diabetes coupled with a complex comorbidity profile has resulted in concomitantly increased healthcare utilization, healthcare costs, and lower productivity in this population.91011 Furthermore, the incidence of comorbidities and healthcare resource utilization and associated expenditures, including healthcare visits, diagnostic procedures, and treatments requiring frequent monitoring and injections, is higher in diabetic patients with DME versus those without DME.111213
DME was traditionally treated with laser photocoagulation, but treatments have evolved to include intravitreal anti-vascular endothelial growth factors (anti-VEGFs; e.g., ranibizumab, bevacizumab, and aflibercept) and corticosteroid injections (e.g., triamcinolone acetonide).1415161718 In landmark clinical trials, frequent (typically monthly) intravitreal injections of anti-VEGF agents, such as ranibizumab (Lucentis®, Genentech, Inc., South San Francisco, CA, USA)19202122 and aflibercept (Eylea®, Regeneron Pharmaceuticals, Inc., Tarrytown, NY, USA),202324 were efficacious in improving visual and anatomic outcomes in patients with DME. In these trials, patients received an average of 8 to 12 intravitreal injections per eye in the first year. In more recent trials, a sustained-release dexamethasone intravitreal implant (Ozurdex®, Allergan plc, Dublin, Ireland) demonstrated sustained efficacy for up to 6 months after a single implant.2526
Off-label intravitreal DME treatments, including the anti-VEGF agent bevacizumab (Avastin®, Genentech, Inc.) and various corticosteroid preparations, have been available in Korea for several years. Furthermore, the Ministry of Food and Drug Safety (MFDS) in Korea approved ranibizumab in 2011 and aflibercept and sustained-release dexamethasone intravitreal implant in 2014. However, data on real-world treatment patterns for DME patients and related healthcare resource utilization in Korea are limited.27 Therefore, we sought to characterize DME treatment patterns in Korea and to examine the impact of treatment on healthcare resource utilization and visual acuity (VA) outcomes.
METHODS
Study design
This retrospective chart review of consecutive patients with DME who received treatment between January 1, 2012 and December 31, 2013 (patient selection period) was conducted at 11 hospital ophthalmology clinics across Korea (5 in Seoul and Gyeonggi, 3 in Daegu, 2 in Busan, and 1 in Daejeon). The baseline date was considered to be January 1, 2009, or the date on which the first treatment of the second or only eye was conducted, whichever was later. The pre-index period was from January 1, 2009 to the day before the index date (in 2012 or 2013) and the post-index period was from the day after the index date to September 30, 2014 (chart extraction date), resulting in a total observation period from January 1, 2009 to September 30, 2014 (Fig. 1). An electronic database containing medical records of eligible patients was created and all data were de-identified.

Patients
Patients were eligible if they had a clinical diagnosis of DME, received ≥ 1 laser or pharmacotherapy treatment(s) during the patient selection period, and had ≥ 1 follow-up visit. Patients with concurrent progressive retinal disease (e.g., neovascular age-related macular degeneration [AMD] and retinal vein occlusion [RVO]) requiring treatment to prevent vision loss or those participating in a clinical trial were excluded. Patients with concurrent stable retinal disease (e.g., RVO or dry AMD) not requiring treatment to prevent vision loss were included at the investigator's discretion.
Outcomes
Primary outcomes were healthcare resource utilization (defined as clinic visits, DME treatment visits, and visits during which optical coherence tomography [OCT] and fluorescein angiography [FA] were performed), time from diagnosis of DME to treatment, change in distribution of DME treatments over time, and proportion of affected eyes undergoing a treatment switch. All outcomes were assessed from the baseline visit to the end of follow-up.
Secondary outcomes included change in VA (in approximate Early Treatment Diabetic Retinopathy Study [ETDRS] letters), use of FA and OCT in deciding treatment, and safety. VA was originally determined as per the Snellen chart and converted to an ETDRS letter score using a published algorithm.28 To ensure comparability of the central macular thickness (CMT) measurements across the different OCT machines used, CMT measurements were transformed to Stratus-equivalent values using published algorithms.2930
Data collection
We reviewed eligible patients' charts and extracted data between October 2014 and January 2015. Patient demographics and disease characteristics were collected from baseline. If a characteristic was not recorded at baseline, a search of the 12 months following (preferentially) or preceding the baseline visit was performed. Characteristics not documented during that period were marked as “missing.” For each clinic visit, data collection included the type of treatment administered (laser photocoagulation, intravitreal corticosteroid [triamcinolone acetonide injection or dexamethasone implant], intravitreal anti-VEGF [ranibizumab or bevacizumab], or other) if applicable, VA of each eye, whether FA was performed, and CMT as measured by OCT. Any treatment received before January 1, 2009 was recorded as medical history. Adverse events (AEs; elevated intraocular pressure, cataract requiring extraction, endophthalmitis, stroke, myocardial infarction, and hospital admissions) occurring from 2009 onward were recorded when available.
Statistical analyses
Descriptive statistics were used for demographic and disease-related data. Chi-squared tests and one-way analysis of variance F-tests were performed to determine the statistical significance of differences between proportions and means, respectively. The standard error of the mean change in VA from baseline was estimated by taking into account multiple post-baseline measurements for each eye. A subanalysis was performed to evaluate the association between anti-VEGF treatment and healthcare resource utilization and patient outcomes. The 95% confidence interval (CI) for each AE rate was calculated by assuming that the number of events followed Poisson distribution. All analyses were performed using the Stata software versions 13, 14 (StataCorp LP, College Station, TX, USA).
Ethics statement
The study protocol was approved by the Institutional Review Board (IRB) of Daegu Catholic University Medical Center (IRB approval No. CR-14-125) at each site and conducted in accordance with the Declaration of Helsinki. Since this was a retrospective chart review, informed consent was waived by the IRB. The sponsor was involved in the study design; collection, analysis, and interpretation of data; writing of the report; and in the decision to submit the article for publication. No honoraria or payments were made for authorship.
RESULTS
Baseline characteristics
Data were extracted from the charts of 522 patients (842 DME eyes) who met the eligibility criteria. Overall, 55.2% of the patients were men, and mean (standard deviation [SD]) age was 59.0 (10.9) years (Table 1). Among patients with available diabetes-related data, almost all (96.7% [444/459]) had type 2 diabetes and approximately half (51.3% [214/417]) had the disease for > 10 years. Nearly half (46.4% [97/209]) of the patients had a glycated hemoglobin (HbA1c) value > 8% and 56.32% had bilateral DME. DME was diagnosed within 30 days of the first recorded treatment for 75% of the eyes; of these, 26.4% eyes were pseudophakic. At baseline, 69.4% of eyes had VA between 20 and 70 ETDRS letters (Snellen, 3/60 to 6/12) and 76.2% had CMT ≥ 300 µm. Most patients had their baseline visits in 2012 (38.9%) and 2013 (41.2%).
Table 1
Demographics and baseline characteristics
Table 2 shows the baseline characteristics of patients categorized by the intravitreal DME treatment received during the first 6 months of treatment.
Table 2
Baseline characteristics of patients categorized by intravitreal DME treatment received during the first 6 months of treatment

Primary outcomes
Healthcare resource utilization
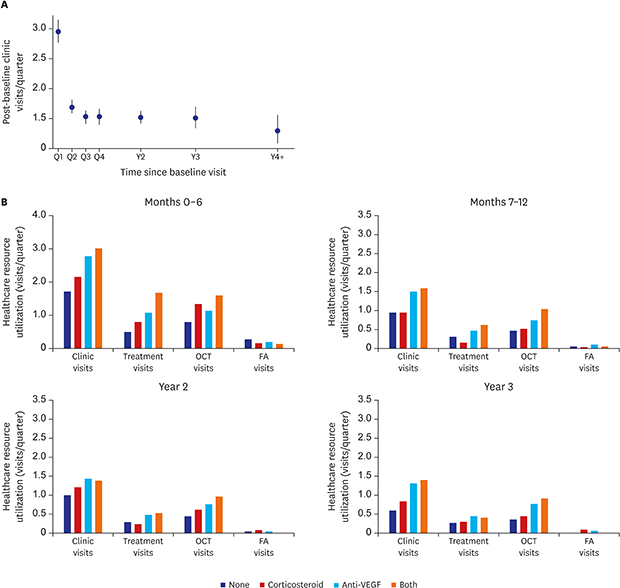
Overall, 522 patients had a total of 5,311 clinic visits for a total follow-up period of 2,995 person-quarters. The average clinic visit rate was 1.8 per quarter through the study period. In the first year post-baseline, the clinic visit rate was 3.0 in quarter 1, indicating that the baseline visits were most likely the patients' first visits; however, this rate reduced to 1.7 in quarter 2 and halved to 1.5 in quarters 3 and 4 thereafter (Fig. 2A).
Fig. 2
Healthcare resource utilization for treatment of diabetic macular edema in Korea. (A) Overall clinic visit rate and (B) Healthcare resource utilization by treatment category over time.
FA = fluorescein angiography, OCT = optical coherence tomography, Q = quarter, VEGF = vascular endothelial growth factor, Y = year.

Results of an analysis of healthcare resource utilization by DME characteristics and treatment received at baseline showed that the clinic visit rate per quarter was higher among patients with non–center-involving DME than those with center-involving DME (2.0 vs. 1.8 per quarter; P < 0.001). Of note, patients receiving anti-VEGF treatment at baseline had a higher rate of clinic visits per quarter than patients receiving laser or corticosteroid treatment (1.9, 1.4, and 1.7 visits per quarter, respectively; Table 3).
Table 3
Healthcare resource utilization by baseline characteristics of index DME eye and treatment received at baseline

Across all treatment categories (no treatment, intravitreal corticosteroid injection, intravitreal anti-VEGF injection, and both intravitreal corticosteroid and anti-VEGF injections), significantly more clinic visits, treatment visits, and OCT and FA assessments occurred per quarter in the first 6 months post-baseline compared with months 7–12, year 2, or year 3 (P ≤ 0.001) (Fig. 2B). Overall, across the observation period, patients who received anti-VEGF agents (with or without corticosteroid treatment) had the highest number of clinic visits, treatment visits, and OCT assessments per quarter.
Time from diagnosis of DME to treatment
The median time from diagnosis of DME to initiation of treatment was 1 week. Three-quarters (75%) of patients were first treated within 30 days of their diagnosis, with an additional 14% and 3% receiving their first treatment in post-diagnosis years 1 and 2, respectively (Fig. 3).
Distribution of DME treatments
During the observation period, use of laser photocoagulation therapy reduced considerably from 57.1% in the first half (H1) of 2009 to 8.7% in the second half (H2) of 2014 (Fig. 4). In contrast, use of intravitreal anti-VEGF injections increased from 28.6% in 2009 H1, plateaued at approximately 78% in 2012 and 2013, and decreased to 65.4% in 2014 H2; however, it was consistently the most commonly used treatment (except in 2009 H1). Use of corticosteroid implants increased steadily from 0.2% in 2012 H2 to 7.7% in 2014 H2. Use of intravitreal corticosteroids fluctuated between 2.4% and 18.3% between 2010 and 2014.
Fig. 4
Distribution of DME treatments during the observation period (2009–2014).
DME = diabetic macular edema, H = half, VEGF = vascular endothelial growth factor.

To avoid the confounding effects caused by temporal trends and disease progression over time, the distribution of treatment in patients with baseline visits in 2012 and 2013 (i.e., patients initiating treatment around the same time) was analyzed. The relative proportions of treatments over this time period were similar to those from 2009 to 2014.
In the subgroup of patients who did not receive intravitreal treatment during the first 6 months, 26%, 41%, and 57% received intravitreal anti-VEGF or intravitreal corticosteroid treatment during months 7–12, year 2, and year 3, respectively. Of those who received intravitreal corticosteroid treatment during the first 6 months, 0%, 47%, and 33% switched to intravitreal anti-VEGF injections (alone or concurrently) during months 7–12, year 2, and year 3, respectively. Among patients who received intravitreal anti-VEGF injections during the first 6 months, 16%, 23%, and 36% switched to intravitreal corticosteroid therapy (alone or concurrently) during months 7–12, year 2, and year 3, respectively.
Proportion of eyes that switched treatments
Initially, intravitreal anti-VEGF treatment was used for 77% of eyes, and alternative therapies were used for the remaining 23% of eyes. At subsequent visits, treatment was switched for 38% of eyes initiated on intravitreal anti-VEGF treatment and 41% of eyes initiated on an alternative treatment. Overall, 56% of patients received only 1 type of treatment (intravitreal anti-VEGF, laser photocoagulation therapy, or other), 34% received 2 types of treatment, and 10% received all 3 types of treatment.
Secondary outcomes
VA
Overall, mean annual VA improved by 1.4 ETDRS letters from baseline. Although not statistically significant, eyes treated with laser photocoagulation therapy at baseline had worsened VA (1.3 letters worse), while eyes not treated with laser photocoagulation at baseline had improved VA (1.7 letters better). Eyes treated with anti-VEGF at baseline had improved VA (1.5 letters better), which was slightly better than that for eyes not treated with anti-VEGF at baseline (1.0 letter better). Men patients had a greater improvement in VA than women patients (mean [standard error (SE)] change in VA from baseline, 1.5 [0.8] versus 1.2 [1.0] letters). In addition, younger patients had greater improvements than older patients (Table 4).
Table 4
Mean change in VA (in letters) after baseline visit by gender and age group

Use of FA
Use of FA was highest in the first quarter of year 1 (0.4 visits) and decreased to 0.01 visits per quarter by year 4 (Fig. 5A). Most FAs were performed at the baseline visit or in the preceding week. However, eliminating FAs performed at baseline did not alter the trend of FA utilization; 0.1 FAs were performed in quarter 1 of year 1, which decreased to 0.03 per quarter in year 3 and 0.01 per quarter in year 4 (Fig. 5B).

Use of OCT
Use of OCT ranged from 1.0 visit in quarter 1 to 0.8 visits in quarter 4 in year 1 post-baseline (Fig. 6). OCT use was highest in the first quarter because an OCT was performed at 66% of baseline visits, which then plateaued during years 2 and 3, and decreased to 0.7 in year 4.

Subanalysis in patients receiving anti-VEGF treatment
The association of anti-VEGF treatment frequency with patient outcomes was examined in a subgroup of 213 patients who received anti-VEGF treatment and had at least 12 months of follow-up. These patients had an average of 8.9 clinic visits, received 2.5 anti-VEGF injections, and had a mean VA improvement of 2.7 letters in the first year of follow-up. Overall, 164/291 (56.4%) patients receiving anti-VEGF injections during the first 6 months of treatment had bilateral DME; this could have had an effect on the average number of clinic visits but not on the average number of injections per eye.
Safety
The most frequently reported AEs were intraocular pressure elevation (34 cases, 0.05 events per person-year; 95% CI, 0.03, 0.06) and cataract extraction (22 cases, 0.03 events per person-year; 95% CI, 0.02–0.04). Myocardial infarction, stroke, and hospital admissions occurred at rates of 0.001 events per person-year (95% CI, 0.000–0.005), 0.001 events per person-year (95% CI, 0.000–0.005), and 0.05 events per person-year (95% CI, 0.04–0.07), respectively (Table 5). There were few hospital admissions, but the associated causes were not available.
Table 5
AEs recorded between the baseline date and chart extraction date (522 patients, 749 person-years at risk)
DISCUSSION
In Korea, there are limited real-world clinical data available on the patterns of healthcare resource utilization and treatment in diabetic patients with DME. To our knowledge, this is the first multicenter retrospective chart review of a large number of diabetic patients with DME in Korea.
The standard of care for DME treatment used to be laser photocoagulation therapy; however, this paradigm has changed with the results of clinical trials showing benefits with intravitreal anti-VEGF and corticosteroid injections.1415192021222324 Studies with intravitreal anti-VEGF agents, such as aflibercept, bevacizumab, and ranibizumab, have consistently demonstrated that these agents are effective and relatively safe for the treatment of DME, which causes vision impairment.20 Results of the current study confirm this paradigm shift. Use of laser photocoagulation therapy reduced considerably from 57.1% in 2009 H1 to 8.7% in 2014 H2. In contrast, use of intravitreal anti-VEGF injections increased from 28.6% in 2009 H1 to a peak of 78%–79% in 2012 and 2013 and then decreased to 65.4% in 2014 H2. The decrease in the use of intravitreal anti-VEGF injections toward the end of the study period could be explained by the simultaneous increase in the use of intravitreal corticosteroid injections from 10.0% to 18.3% between 2013 and 2014 and novel alternatives such as the dexamethasone intravitreal implant from 0.2% to 7.7% between 2012 and 2014.
The number of clinic visits, treatment visits, and visits where OCT and FA were performed was the highest for patients receiving intravitreal anti-VEGF injections versus intravitreal corticosteroid injections or no intravitreal treatment. However, across all treatment groups, these numbers were the highest in the first 6 months post-baseline followed by a decline over months 7–12, year 2, and year 3. A variety of reasons could account for this decrease over time. Patients with DME are a difficult-to-treat population given the high number of comorbidities and high treatment burden. This may lead to difficult treatment-decisions for patients between seeking treatment and managing work or personal commitments. Another possible reason may include partial reimbursement or lack of coverage for DME treatment by the national health insurance system. Together, this could lead to poor patient compliance and a dip in the frequency of treatment and monitoring visits.13 Furthermore, patients in clinical trials and clinical practice are inherently different, and adherence to treatment and monitoring schedules is often less in clinical practice than in clinical trials. For anti-VEGF treatment in particular, the decrease in the frequency of treatment and monitoring can be explained by the findings from recent studies, which demonstrated a lower frequency of treatment and monitoring in patients receiving intravitreal anti-VEGF treatment in clinical practice than in landmark clinical trials such as RISE and RIDE.22 The disparity between clinical practice and clinical trials indicates under-utilization of anti-VEGF treatment in real-world settings, which can negatively affect treatment outcomes.1822313233 Although in a real-world study conducted in UK, the mean gain in VA was 6.6 letters (vs. 2.7 in the current study), it is important to note that the mean number of injections received over 12 months was also considerably higher versus the current study (7.2 vs. 2.5).32
Previous phase II and phase III studies for intravitreal anti-VEGF injections have suggested a trend toward greater visual benefit associated with more frequent injections. A greater gain in ETDRS letters was observed in studies implementing a more frequent injection regimen (RISE/RIDE22 and RESOLVE34) versus those with a less frequent injection regimen (RESTORE35 and the Diabetic Retinopathy Clinical Research Network Protocol3637), even though all of them followed a monthly follow-up schedule. This possibly clarifies the findings of this study that although the frequency of treatment and monitoring in patients receiving intravitreal anti-VEGF treatment at baseline was the highest among all treatment types, it may not have been high enough, thereby leading to a small and disproportionate gain in VA (mean, 2.7 letters) versus that reported by major clinical trials.
Patients with diabetes, especially those with DME, have a considerable pre-existing healthcare burden even before deciding on a treatment for DME.11 It is therefore important to consider the treatment intensity and monitoring requirements when deciding on a therapy for this population. Monitoring requirements or additional healthcare visits associated with intravitreal treatment may not only affect the patient but also the caregivers and healthcare providers responsible for the coordination of multiple visits.1113 A treatment that offers reduced dosing and monitoring frequency without compromising VA might improve patient compliance to treatment and subsequently improve visual outcomes in the real-world clinical setting. The slight increase in the use of sustained-release dexamethasone intravitreal implant in the latter half of 2014 reflects the perceived benefit of this modality that requires a four times lower dosing frequency25 in comparison to intravitreal anti-VEGF injections that can be burdensome and uncomfortable for patients. Furthermore, dexamethasone implants are beneficial in patients refractory to anti-VEGF injections; studies have shown that eyes with DME considered refractory to anti-VEGF injections that were switched to dexamethasone implants had better visual and anatomical outcomes than those that were continued on treatment with anti-VEGF therapy.3839 A recent study conducted in Korea also demonstrated that dexamethasone implants improved VA and decreased retinal thickness in patients that did not respond to previous treatment including anti-VEGF injections and laser photocoagulation.40
We observed a radical shift in treatment patterns over the study period; use of laser photocoagulation drastically reduced, whereas use of anti-VEGF and corticosteroid injections considerably increased. A variety of reasons could account for the change in the distribution of DME treatments over time in Korea. The positive VA improvements demonstrated by intravitreal anti-VEGF injections in landmark clinical trials could have led to their increased and continued use by Korean clinicians in patients with DME. Moreover, multiple studies in Korea demonstrated that the combination of laser photocoagulation and anti-VEGF injections did not yield better visual and anatomical outcomes than anti-VEGF therapy alone in patients with DME4142; this may possibly have discouraged the use of combination treatment in Korea and contributed to the decrease in the use of laser photocoagulation. However, this did not translate to visual outcomes similar to those reported in the major clinical trials. Furthermore, in contrast to the findings from another real-world study, intravitreal anti-VEGF injection use did not entirely eclipse laser photocoagulation therapy in our study.17 Whether this reflects suboptimal response with intravitreal anti-VEGF injections or raises concerns about their long-term effects or VEGF resistance remains to be investigated in future studies. Of note, use of the dexamethasone implant increased toward the end of the study period. Previous studies in clinical settings in Korea have demonstrated the effectiveness of dexamethasone intravitreal implants in patients with DME, especially in pseudophakic eyes, DME with subretinal fluid, or diffuse type DME.43
While this study has several strengths, including length of observation time, some limitations must be acknowledged. A retrospective design can result in selection bias and missing data, necessitating caution when interpreting results. However, our results were consistent with the findings from other real-world studies, which also observed decreased use of laser photocoagulation therapy and increased use of intravitreal anti-VEGF injections.161718 The relationship between the type of treatment received and visual outcomes should be more closely examined in future studies.
In conclusion, the results of this study demonstrated that intravitreal anti-VEGF treatment is the most frequently used treatment and accounts for the most healthcare resource utilization in patients with DME in Korea. However, the associated outcomes in real-world clinical settings are not as encouraging as those observed in the landmark clinical trials, possibly because of a lower frequency of treatment and monitoring in real-world clinical settings than in the clinical trials. Alternative treatments with comparable outcomes but reduced frequency of dosing and monitoring need to be explored.
 XML Download
XML Download