

 Citation
Citation Print
Print



INTRODUCTION
Diabetic nephropathy is one of the most common causes of end-stage renal disease (ESRD) worldwide.123 As the prevalence of diabetes has continued to increase, a parallel increase has been seen in the prevalence of dialysis patients and associated costs. This increase in the number of patients with chronic kidney disease (CKD) has led to social and economic problems in many countries.1 Moreover, the clinical course of diabetic nephropathy is usually characterized by relatively rapid progression compared with CKD due to other causes.4 In addition, as diabetic ESRD patients are more prone to cardiovascular morbidity and mortality than other ESRD patients, early identification of diabetic nephropathy and prompt renoprotective treatment are critical for the prevention of end organ damage.5 Previous studies have shown that intensive control of blood glucose and blood pressure are not sufficient to prevent or delay the development of diabetic nephropathy.56 However, effective therapy is not available yet, and integrated treatment strategies are therefore needed to improve the management of diabetic nephropathy.56
The so-called ‘uremic toxins,’ such as indoxyl sulfate, are biologically active substances involved in the progression of renal failure.7 Both clinical and experimental studies have suggested that indoxyl sulfate plays an important role in the progressive loss of intact nephrons through induction of an inflammatory reaction and enhanced expression of profibrotic cytokines.7 AST-120 (Kremezin®), a spherical adsorptive carbon preparation, absorbs and removes uremic toxins such as indoxyl sulfate in the digestive tract.8 To date, the renoprotective effects of AST-120 have been determined mostly in patients with advanced CKD with inconsistent results.91011 Furthermore, little is known about the efficacy of AST-120 and which clinical and biochemical variables predict response to AST-120 treatment in diabetic nephropathy.
We therefore aimed to determine whether the addition of AST-120 to conventional treatments is effective to attenuate the progression of renal dysfunction in patients with type 2 diabetes and CKD. We also examined which clinical variables and biochemical tests, particularly oxidative stress markers, could predict beneficial effects of AST-120 in diabetic nephropathy.
METHODS
Study subjects
This study was a prospective, single-arm, open-label, multi-center study performed in subjects with overt diabetic nephropathy. Outpatients with type 2 diabetes and renal dysfunction who had not previously undergone dialysis from eight hospitals in Korea were prospectively enrolled in this study from 2008 to 2009. Study subjects had serum creatinine (sCr) levels ranging from 1.5 to 3.0 mg/dL measured at least three time points over a period of 12 months prior to treatment. We excluded any patients with active liver disease, acute infection, and those who had recent (< 6 months) acute coronary syndromes and cerebrovascular disease. After confirming a negative slope of the reciprocal serum creatinine level (1/sCr) time plot, oral administration of AST-120 6 grams per day was started and continued for 24 weeks.
Clinical and laboratory examination
Blood pressure was measured with the participant in a seated position after 5 minutes of quiet rest. Blood samples were collected after overnight fasting. Blood urea nitrogen, creatinine, glucose, and lipid profiles were measured. Insulin resistance was estimated by the homeostasis model assessment of insulin resistance: [fasting insulin (μIU/mL) × fasting glucose (mmol/L)]/22.5.12 sCr was measured by the standard enzymatic method. Creatinine clearance (CrCl) was estimated by the Cockcroft-Gault equation; CrCl = [(140 − age) × weight (kg)]/sCr × 72 (× 0.85, if women).13 Glomerular filtration rate (GFR) was estimated using the Chronic Kidney Disease Epidemiology Collaboration equation.14 Diabetic retinopathy was diagnosed by an experienced ophthalmologist or diabetologist based on retinal images.15 Superoxide dismutase (SOD) activity in serum was determined with the Superoxide Dismutase Assay kit (Cayman Chemical Company, Ann Arbor, MI, USA), which utilizes a tetrazolium salt for detection of superoxide radicals generated by xanthine oxidase and hypoxanthine. One unit of SOD is defined as the amount of enzyme needed to exhibit 50% dismutation of the superoxide radical. Serum lipid peroxidation (LPO) was determined by a colorimetric assay using the Bioxytech LPO-586 kit (OxisResearch, Portland, OR, USA). Urinary excretion levels of 8-hydroxydeoxyguanosine (8-OHdG) were measured with an enzyme-linked immunosorbent assay (8-Hydroxydeoxyguanosine Check; Japan Institute for the Control of Aging, Shizuoka, Japan).
The rate of progression of renal dysfunction was assessed as the gradient of the reciprocal serum creatinine level (1/sCr), as described by Mitch et al.,16 before and after the initiation of treatment. The 1/sCr was plotted against time, and the regression coefficient was determined by least-square linear regression analysis as previously described.17 In our study, the primary endpoint was improvement in renal function as the ratio of the 1/sCr-time slope for post- to pre- AST-120 therapy. Based on the ratio changes of the regression coefficients of 1/sCr before and after treatment, efficacy of this drug was defined as follows: 1) definitely improved: ≤ 0.30; 2) moderately improved: 0.31–0.60; 3) slightly improved: 0.61–0.90; 4) unchanged: 0.91–1.09; and 5) deteriorated: ≥ 1.10. Subjects in the definitely, moderately, or slightly improved groups (ratio ≤ 0.9) were classified as responders and those in the unchanged and deteriorated groups were considered non-responders. To determine whether baseline sCr levels affect the efficacy of AST-120 treatment, patients were divided into three groups according to the baseline sCr tertile values. The secondary endpoints were changes in 1) CrCl; 2) 1/sCr-time slope pre- and post- AST-120 treatment; and 3) oxidative stress markers. Changes in sCr, serum urea nitrogen, hematocrit, glucose, lipid profile, and systolic and diastolic blood pressure after AST-120 therapy were also compared.
Statistical analysis
Data are expressed as means ± standard deviations. The χ2 test, Fisher's exact test, and Mann-Whitney test were used to compare the characteristics of study subjects. Parameters before and 24 weeks after AST-120 were compared by paired t-test. The clinical per-protocol (PP) population was defined as all patients taking the study medication for 24 weeks with a compliance rate of ≥ 70%, and 76 patients were enrolled for PP analysis. The primary end point was analyzed based on the PP population to better report additional efficacy.18 Other secondary endpoints were analyzed based on the intention-to-treat population, which consisted of all patients taking at least one dose of study medication. Missing data were input using the last-observation-carried-forward procedure. To assess the utility of the predictive factor for efficacy of AST-120, we conducted receiver operating characteristics (ROC) curves and calculated the areas under the curve (AUC). All statistical analyses were performed using PASW version 18.0 (SPSS, Chicago, IL, USA). A P value < 0.05 was considered significant.
Ethics statement
The investigators explained the purpose of the study to the patients at the time of study entry and written informed consent was obtained from all patients. The study was approved by the Institutional Review Board (IRB) of each participating center and was conducted in accordance with the Declaration of Helsinki (Samsung Medical Center IRB No. 2008-02-015).
RESULTS
Table 1 shows the baseline characteristics of the patients. The mean age was 62.6 years and 77% of study participants were men. Eighty-nine percent of patients were taking an angiotensin-I-converting enzyme (ACE) inhibitor and/or angiotensin II receptor blocker, and 83% were taking a statin. The mean estimated GFR was 34.7 mL/min/1.73 m2 and 17, 51, 32 subjects were CKD stage 3a, 3b, and 4, respectively. We analyzed 76 subjects for the primary endpoint and 100 subjects for the secondary endpoints.
Table 1
Baseline characteristics of study participants treated with AST-100 (n = 100)
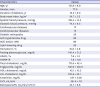
Data are expressed as means ± standard deviation or percentages.
ACEi = angiotensin-I-converting enzyme inhibitor, ARB = angiotensin-II-receptor blocker, HbA1c = hemoglobin A1c, HOMA-IR = homeostasis model assessment of insulin resistance, HDL = high-density lipoprotein, LDL = low-density lipoprotein, CrCl = creatinine clearance, GFR = glomerular filtration rate.
![]()
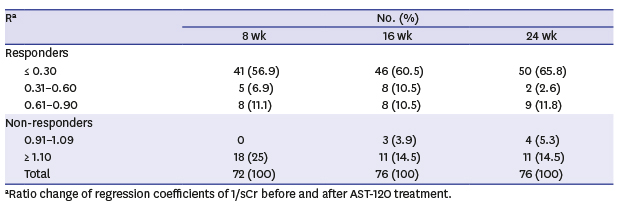
Of 76 patients (PP population) analyzed for the primary endpoint, 50 were definitely improved, 2 were moderately improved, and 9 were slightly improved responders after 24 weeks of treatment with AST-120. Among non-responders, 4 were unchanged and 11 were deteriorated based on the criteria for changes in sCr levels described above. As a result, 61 patients (80.3%) were categorized as responders and 15 patients (19.7%) were non-responders to the AST-120 therapy (Table 2).
Table 2
Efficacy of AST-120 after treatment for 8, 16, and 24 weeks

![]()
Next, we determined baseline characteristics of the responder and non-responder groups. There were no differences in age, gender, previous treatment modalities, baseline sCr or CrCl, lipid profile, and blood glucose levels between the two groups; however, diastolic blood pressure was significantly different (Table 3). The non-responder group had a higher diastolic blood pressure than the responder group (79.3 ± 11.1 mmHg vs. 73.5 ± 9.5 mmHg, respectively; P = 0.046). We also analyzed the efficacy of 24-week AST-120 treatment according to baseline sCr tertile. All three groups demonstrated a significant improvement in renal function determined by the ratio changes of regression coefficients of 1/sCr after AST-120 treatment. In particular, individuals with lower baseline sCr (lower and middle tertiles) were more likely to show improved renal function after AST-120 treatment compared to individuals with higher baseline sCr (upper tertile) (P = 0.024) (Table 4).
Table 3
Comparison of baseline characteristics between responders and non-responders
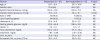
Data are expressed as means ± standard deviation or number (percentages).
ACEi = angiotensin-I-converting enzyme inhibitor, ARB = angiotensin-II-receptor blocker, HbA1c = hemoglobin A1c, CrCl = creatinine clearance, GFR = glomerular filtration rate, NS = not significant.
![]()
Table 4
Efficacy of 24 weeks of AST-120 treatment according to baseline sCr tertile

P value for the comparison between responders and non-responders across the tertiles.
sCr = serum creatinine.
aRatio changes of regression coefficients of 1/sCr before and after AST-120 treatment.
![]()
Table 5 shows clinical and laboratory findings before and after AST-120 treatment in the responder and non-responder groups. Administration of AST-120 significantly increased serum SOD level in both the responder and non-responder groups. In addition, serum LPO level was significantly decreased in the responder group (from 2.25 ± 0.56 μmol/L to 1.91 ± 0.72; P = 0.002), but not in the non-responder group. Urine 8-OHdG levels showed no significant changes in either the responder or non-responder groups. AST-120 treatment had no significant effect on the other clinical or biochemical parameters tested including blood urea nitrogen, hematocrit, glucose, and lipid profile in either the responder or non-responder groups. The renal function in all patients was maintained and no patients started dialysis therapy.
Table 5
Clinical and laboratory findings after 24 weeks of AST-120 treatment in the responder and non-responder groups

Data are expressed as means ± standard deviation.
CrCl = creatinine clearance, HbA1c = hemoglobin A1c, LDL = low-density lipoprotein, HDL = high-density lipoprotein, SOD = superoxide dismutase, LPO = lipid peroxidation, 8-OHdG = 8-hydroxydeoxyguanosine, NS = not significant.
![]()
DISCUSSION
The present study involved 100 undialyzed patients with diabetic nephropathy from eight tertiary centers in Korea. These patients were confirmed to have progressive renal dysfunction under conventional treatments based on negative 1/sCr gradients observed over a period of one year prior to treatment. Rates of decline in 1/sCr were compared before and after AST-120 treatment. Treatment with AST-120 for 24 weeks significantly attenuated the progression of renal dysfunction in 80.3% of patients with diabetic nephropathy. These results suggest that co-administration of AST-120 with conventional treatments may delay the progression of renal dysfunction in diabetic nephropathy. In addition, improvement in the 1/sCr slope was independent of sCr levels before AST-120 treatment. With the exception of diastolic blood pressure, there were no significant differences in other background factors including age, gender, previous treatment modalities, renal function, lipid profile, and fasting plasma glucose level between the responder and non-responder groups. These findings imply that the therapeutic effect of AST-120 is basically independent of previous treatment modalities, hyperlipidemia, anemia, and hyperglycemia, and indicate that AST-120 could be an effective treatment modality for diabetic nephropathy in patients with diverse baseline clinical features. However, lower baseline diastolic blood pressure may predict a better response to AST-120 treatment. When we performed the ROC analysis, the optimal discriminating cutoff value of diastolic blood pressure for detecting subjects with non-response was 79.5 mmHg, with a sensitivity of 60.0% and specificity of 68.9% (AUC = 0.67; 95% confidence interval, 0.51–0.83; P = 0.047; data not shown).
Our findings are consistent with previous observations in patients with diabetic nephropathy.192021 In a study performed in 276 patients with advanced diabetic nephropathy and sCr levels ranging from 3.4 to 4.5 mg/dL, treatment with AST-120 for six months decreased the sCr level in 30% of patients. In addition, the beneficial effect of AST-120 was more evident in patients with normal blood pressure and a hematocrit of 30% or above.20 In another study performed in 16 patients with CKD and type 2 diabetes (sCr < 1.5 mg/dL and urinary protein > 0.5 g/day), administration of AST-120 initiated in overt diabetic nephropathy delayed the progression of renal dysfunction.19
The optimal time to initiate AST-120 treatment in patients with CKD remains unclear. It was suggested that CKD patients with sCr levels ≥ 3.0 mg/dL have increased serum indoxyl sulfate levels.22 Shoji et al.23 showed that AST-120 treatment in CKD patients tended to be more effective in delaying GFR decline in the high GFR (≥ 31.4 mL/min) group than in the low GFR (< 31.4 mL/min) group. In addition, other studies showed a renoprotective effect of AST-120 even in early-stage CKD. A Japanese study reported that AST-120 had renoprotective effects in patients with CKD whose creatinine concentrations were between 1.2 and 3.0 mg/dL.24 Furthermore, AST-120 treatment delayed an increase in sCr level even in patients with early diabetic nephropathy, in which mean baseline estimated GFR ranged from 60.0 to 84.2 mL/min/1.73 m2.19 Consistent with these observations, the baseline mean sCr level in our study was approximately 2.0 mg/dL and individuals with lower baseline sCr were more likely to show improved renal function after AST-120 treatment compared to individuals with higher baseline sCr. Although we are unsure of the underlying mechanism, it is possible that AST-120 treatment is more effective in delaying the deterioration of renal function in early stage CKD in which more severe metabolic abnormalities and irreversible structural changes in the renal parenchyma have not yet occurred. In addition, a recent post hoc analysis of the EPPIC study population demonstrated that treatment with AST-120 delayed time to dialysis and prevented depression in renal function in patients with higher baseline proteinuria and positive hematuria.25 Although we did not measure proteinuria or hematuria in the current study, it would be interesting to determine whether proteinuria or hematuria is a marker of response to AST-120 in patients with diabetic kidney disease. Disruption of antioxidant systems is one of the crucial factors that promote renal dysfunction.26 Superoxide anion radicals and their metabolites are well-known harmful reactive oxygen species. Oxidative stress produces oxidized low-density lipoproteins and degenerate lipoproteins. Products of LPO play important roles in vascular sclerosis including nephrosclerosis. Peroxidation of lipids is known to be one of the aggravating factors in the progression of CKD in humans and animal models.2728 In addition, SOD is a principal active component against oxidative stress and is disturbed in uremic state.29 In this study, we investigated the renoprotective mechanism of AST-120 focusing on changes in oxidative stress markers. As the lipid profile was not changed after AST-120 treatment in either the responders or non-responders, the renoprotective effect of AST-120 cannot be attributed to a reduction in serum cholesterol. However, AST-120 treatment significantly increased serum SOD levels in both the responder and non-responder groups. In particular, after AST-120 treatment, serum lipid peroxide levels significantly decreased only in the responder group. These results indicate that the antioxidant activity of AST-120 may play a critical role in delaying the progression of renal dysfunction in patients with diabetic nephropathy.
This study has some limitations. First, since all enrolled subjects were treated with 6 g/day AST-120 (Kremezin®) for 24 weeks, there was no control group. Second, we were not able to measure indoxyl sulfate or proteinuria during the experimental period. Third, due to the short duration of intervention, the development of ESRD events could not be assessed. Fourth, although not statistically significant, there were numerical differences in the percentage between responders and non-responders who took medications that may affect renal function including ACE inhibitor, angiotensin II receptor blocker and lipid-lowering drugs. Despite these limitations, our study demonstrates the renoprotective effect of AST-120 with a relatively large number of patients with diabetic nephropathy and suggests a potential renoprotective mechanism of AST-120.
In conclusion, our data suggest that co-administration of AST-120 with conventional treatments may delay the progression of renal dysfunction in diabetic nephropathy, and lower diastolic blood pressure could be a predictor for better response to AST-120 treatment. We also found that a decrease in oxidative stress might be responsible for the efficacy of AST-120 treatment in diabetic nephropathy. Given the increasing incidence of diabetic nephropathy as the underlying cause of CKD, our findings suggest that AST-120 may prevent deterioration in renal function in CKD. Further large-scale studies are warranted to determine the long-term cardiovascular benefits of AST-120 treatment.
 XML Download
XML Download