

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
White matter lesions (WMLs) and lacunar infarcts (LIs) on brain magnetic resonance imaging (MRI) are common in elderly people and are believed to be caused by microvascular disease or small vessel disease (SVD) [1]. The prevalence of cerebral SVD varies among races [2]. For example, its prevalence in the South Asian population is about 40-60%, higher than that in the white population [3, 4]. In South Korea, lacunar cerebral infarctions are much more common than in the Western world [5, 6]. The exact causes of WMLs and LIs remain unclear, but chronic cerebral ischemia has been regarded as the main pathomechanism [7-10]. When WMLs and LIs coexist, they appear to have the same pathomechanism, although other causative factors may contribute to pathogenesis in individuals with isolated WMLs (without LIs). WMLs can be divided into two groups, periventricular and deep subcortical WMLs depending on their anatomical distribution. A previous radiological study showed that certain cerebral regions are more vulnerable to cerebrovascular pathology [11]. Therefore, it remains unclear whether periventricular and deep subcortical WMLs result from the same or different vascular pathological processes. Studies of the relationship between WMLs, LIs and cognitive function in demented and nondemented elderly individuals have yielded inconsistent findings [12-17]. For example, periventricular WMLs have been associated with cognition [18] and deep subcortical WMLs with depression [19] or cognition [20]. We therefore sought to identify which subtype of WMLs is more closely related to LIs and, in addition, their relationship to cognitive impairment and activities of daily living (ADL) in a group of patients with vascular cognitive impairment with subcortical vascular lesion (VCI-S).
METHODS
1. Subjects
Data were derived from the MRI300 study, part of the Clinical Research for Dementia of South Korea (CREDOS) study, a nationwide multicenter study starting in 2005 of elderly individuals with dementia in South Korea. This study developed common protocols, including its own ischemic scale, and recruited patients with subjective memory impairment, mild cognitive impairment (MCI), MCI of a subcortical vascular type, Alzheimer's Disease (AD), and subcortical vascular dementia (SVaD). The MRI300 project, which was devoted to evaluate the relationship between various clinical variables and WMLs in patients with mild-to-moderate dementia, recruited approximately 300 patients with newly diagnosed mild-to-moderate dementia (clinically probable AD or SVaD) from March 2007 to April 2008, and was performed at 13 dementia clinics in university or general hospitals throughout the country.
Patients included in the MRI300 study were as follows: 1) aged 50-85 years; 2) had mild to moderate dementia, as determined by evaluations such as a complete medical history including vascular risk factors (such as hypertension, diabetes, hyperlipidemia, previous stroke history, and smoking), physical and neurologic examinations, neuropsychological tests; vascular risk factors were regarded as positive either if the patient had previously been diagnosed with associated diseases or if he or she was currently under medications for those diseases. 3) had undergone MRI scans; 4) had a standard laboratory dementia screen (complete blood counts, blood chemistry panels, vitamin B12/folate levels, syphilis serology, and thyroid function tests); 5) provided a written informed consent; and 6) had a primary caregiver who could supervise evaluations assessing the condition of the patient throughout the study, and to provide input into efficacy assessments in accordance with all protocol requirements. Mild-to-moderate dementia was defined as a clinical dementia rating (CDR) of 0.5, 1, or 2 [21]. Patients had either AD with varying degrees of white matter changes or SVaD. All patients diagnosed with clinically probable AD fulfilled the criteria for probable AD proposed by the NINCDS ADRDA (National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association)[22]. Patients diagnosed with SVaD had to have symptoms fulfilling both the clinical criteria for vascular dementia as described in the Diagnostic and Statistical Manual of Mental disorders, 4th edition (DSM-IV) and the imaging criteria of the CREDOS study. These criteria included periventricular capping or banding ≥10 mm in length and deep WMLs ≥25 mm in length.
Patients falling between the full diagnostic criteria for AD and SVaD were regarded as having AD, with or without WMLs. Therefore, rather than dichotomizing these patients into either AD or SVaD categories, we classified all patients according to the ischemic scale the CREDOS defined (Table 1). We therefore excluded patients with degenerative etiologies other than AD, such as idiopathic Parkinson's disease, diffuse Lewy body disease, corticobasal degeneration, and progressive supranuclear palsy. We also excluded patients with structural lesions such as territorial infarction, intracranial hemorrhage, brain tumor, and hydrocephalus. Those with current or past neurological or psychiatric illnesses such as schizophrenia, epilepsy, encephalitis, and severe head trauma were ruled out.
To investigate the relationship between WMLs and LIs, we selected from the MRI300 study patients with SVaD and those with AD containing moderate degree of WMLs. We considered the latter as having AD with cerebrovascular disease (CVD), one of the subtypes of vascular cognitive impairment (VCI) [23, 24]. We designated these two groups of patients as having with vascular cognitive impairment with subcortical vascular lesion (VCI-S). Of the 289 patients enrolled into the MRI300 study, 128 (44.2%) were chosen, including 106 with AD with CVD and 22 with SVaD.
The study was approved by the institutional review board of all participating centers. Written informed consent was obtained from patients and their caregivers.
2. MRI scanning
All subjects were assessed in 2005 and 2006 by MRI, following a standard protocol within 6 months of the clinical investigation. Cerebral MRI included axial T1-, T2-weighted images, gradient echo sequences, and fluid-attenuated inversion recovery (FLAIR) images (1.5T Vision Philips, Siemens, General Electric). The entire brain was imaged in the axial plane with 1.6-10 mm slice thicknesses.
3. Assessment of white matter lesions
Three neurologists trained in rating ischemic white matter changes, and blinded to clinical and functional data, rated the white matter changes on the T2 axial and/or FLAIR images. The CREDOS rating scales were developed by the CREDOS study steering committee, with modifications from Fazekas' [25] and Scheltens's [26] scales. WMLs were evaluated in periventricular WML (P rating) and deep subcortical WML (D rating) areas separately and the D and P ratings were combined to provide a final ischemia degree. Deep subcortical WMLs were divided into D1 (deep subcortical WML<10 mm), D2 (10≤deep subcortical WML<25 mm), and D3 (≥25 mm) based on the longest diameter of lesions. Periventricular WMLs were classified into P1 (capping and banding <5 mm), P2 (between P1 and P3), and P3 (capping or banding≥10 mm) based on the size of cap and band, which were perpendicular and horizontal to the ventricle, respectively. The results were combined to provide a ischemia rating as mild (D1P1, D1P2), moderate (neither minimal nor severe group), or severe (D3P3)(Table 1). As previously mentioned, D3P3 was used as the imaging criteria for SVaD diagnosis. The inter-rater reliabilities for assessment of periventricular, deep, or total white matter changes were excellent (κ=0.726-0.905).
4. Lacunar infarcts
The number of lacunae was rated visually by a single rater (HY Kim, MD) blinded to clinical information and diagnosis. LIs were defined as areas of focal hyperintensity on T2-weighted images, hypointensity on T1-weighted images and hypointensity with perilesional halo on FLAIR of size 3 to 20 mm and located in the subcortical white matter, basal ganglia and thalamus. Non-lacunar territorial infarcts were excluded from the counting of LIs. Ambiguous lesions were reviewed through consultation with a neuroradiologist (RH Juh, PhD), blinded to patient history and clinical information.
5. Image analysis of white matter volume
The ANALYZE software package (Mayo Clinic, USA), version 9.0, was used to process Images, to estimate WML volume and to rate LIs. Due to the different slice thicknesses of the FLAIR images, we utilized ANALYZE software to resample the original FLAIR images with slice thicknesses 4 mm, followed by the use of the region-of-interest (ROI) function within the package, allowing the rater to create automated traces along with WML on individual images. When the largest diameter of a WML was adjacent to the ventricular lining (e.g. adjacent to the occipital and frontal horns, or the lateral ventricles), that WML was considered periventricular; otherwise, it was considered deep subcortical WML. To measure its volume, the ROI of each slice was multiplied by the slice thickness (4 mm) and all ROI volumes from each images was summed to calculate the total volume, in cubic milliliters. All summation processes were performed automatically by the ANALYZE program.
6. Cognitive function and activities of daily living
General cognitive function was measured using in Korean version of Mini-Mental State Examination (K-MMSE) and instrumental ADL (IADL) tasks were measured using the Seoul-Instrumental Activities of Daily Living (S-IADL) [27]. We evaluated the S-IADL from the perspective of current performance.
7. Data analysis
Since WML volume data were positively skewed, we assessed the relationship between the natural log of WML volume and LIs. Univariate comparisons between demographic data and periventricular and deep subcortical WML volume and the number of LIs were performed using univariate Poisson log-linear models. Periventricular and deep subcortical WML volumes were entered separately, along with adjusted variables, into the multivariate Poisson log-linear models. Adjusted variables were selected for multivariate analysis if their p values were below 0.2 in the univariate log-liner model. Spearman's correlation analysis was used to assess the relationship among K-MMSE, S-IADL and WML volume. Statistical significance was set at p<0.05. All statistical analysis was performed using SPSS for Windows version 18.0 (Windows, Chicago, IL, USA) or SAS, version 9.1 (SAS Institute, www.sas.com).
RESULTS
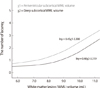
Baseline characteristics of WMLs (periventricular WML and deep subcortical WML) and LIs of the study population were presented in Table 2. Seventy patients (54.7%) had at least one lacune. The distribution of the number of LIs was right skewed, whereas the distribution of WML volume was left skewed. Univariate Poisson log-linear models were used to assess the relationships of baseline characteristics (age, sex, vascular risk factors and previous stroke history) with WML volume and LIs, respectively. We found that history of hypertension, history of stroke and both WML volume (periventricular and deep subcortical) were associated with LIs (Table 3). Each unit of natural logarithm of deep subcortical and periventricular WML volume had multiplicative impact of 1.487 and 1.566, respectively, on the number of LIs. Fig. 1 shows the association between each type of WML volume and the number of LIs. To assess the independent association of each WML subtype with LIs, each WML with other variables (history of hypertension and history of stroke) were entered simultaneously into multivariate Poisson log-linear models. We found that an increase in both subtypes of WML volume (deep subcortical WML p=0.013, periventricular WML p=0.010) and a history of hypertension (p=0.004) were independently associated with LIs (Table 4). Spearman's correlation analysis, however, did not show any significant relationship between K-MMSE and either periventricular WML (p=0.30) or deep subcortical (p=0.86) WML. We also found that total current S-IADL score was not related to periventricular (p=0.06) and deep subcortial (p=0.73) WML.
DISCUSSION
The primary result of this study was that LIs were associated with WMLs regardless of their subtypes in patients with VCI-S, a subgroup of a well-defined large Korean cohort of patients with dementia. These findings may suggest that both types of WMLs (periventricular and deep subcortical) share the same vascular pathomechanism as LIs, SVD, a finding in agreement with earlier observations [28].
WMLs and LIs have been generally regarded as SVD. A few population-based studies have reported on the correlation of between these MRI abnormalities. A small community based study showed that periventricular, deep subcortical and total WMLs were highly correlated with each other [29]. In contrast to the SVD pathology almost inherent in LIs, WMLs have various underlying pathologies [7, 30, 31] including mild reactive astrocytic gliosis, dilatation of perivascular spaces and the loss of myelin, axons and oligodendroglial cells. In addition, a large population study showed no significant interaction between LIs and total WMLs in non-demented patients, with both WMLs and LIs independently associated with general cognitive function [32]. In the present study, using a semiquantitative MRI volumetric method, we found that both types of WMLs, whether they are periventricular or deep subcortical, were equally related to LIs. We deliberately included subjects who showed moderate or severe WMLs on MRI and excluded those with mild WMLs. It would be more reasonable to include them all in order to better look at the relationship between WMLs and LIs because it could cover the whole spectrum of the amount of WMLs. However, we thought that approach would seriously undermine the homogeneity of study population. AD with mild WMLs is more likely to belong to pure AD, nullifying the prerequisite of vascular cognitive impairment. Besides, WMLs in this group were so minimal-cap or band<5 mm and deep WML<10 mm in length-that they would escape from any meaningful analysis.
Contrary to our expectation, we did not find any significant relationship between age and WMLs. It has been a general understanding that WMLs go in parallel with increasing age. Also, we found that WML volumes were not associated with general cognitive function and severity of IADL. This disparity may be due to differences in the methods used to assess WMLs with some studies evaluating the presence of WMLs and others using ischemic rating scales. Alternatively, it may be due to our widespread inclusion of patients with SVaD and those with AD with CVD all together, since the underlying AD pathology in the latter group may have dominantly contributed to cognitive dysfunction and the severity of IADL. Given the majority of subjects consisting of AD with CVD (82.8%), the impact of AD pathology would be considerable. Our study is limited by relative inhomogeneity of the study population and by the lack of information on the involvement of Alzheimer's pathology such as hippocampal atrophy, apolipoprotein E4 genotype, and cortical amyloid deposition. Furthermore, although tests of frontal executive function are known to be more sensitive in capturing the effect of SVD, we only assessed general cognitive function to make the correlation with WMLs and LIs. MMSE was not sufficient enough to represent general cognitive function and measure their relationship in this study population.
Among other limitations, we used our own ischemic rating scale to stage WMLs, although we did not show the usefulness of our scale as a valid rating method. In addition, we did not take into consideration cerebral microbleeds (MBs) which is now being regarded as another important marker of SVD. The strength of this study lies in a relatively large number of individuals with mild to moderate dementia selected from a well-designed Korean database. In addition, we adopted a quantitative volume analysis rather than using a qualitative measurement for WMLs, which could provide more accurate and objective results in assessing WMLs.
In conclusion, we clarified the strong correlation of LIs with each type of WMLs, suggesting that they all represent a continuum of cerebral SVD. Therefore, WMLs and LIs should be regarded as markers of SVD, emphasizing the importance of identifying and controlling modifiable vascular risk factors to arrest the SVD process in vascular cognitive impairment.




 XML Download
XML Download