

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Mild cognitive impairment (MCI), particularly, amnestic MCI (aMCI) has been identified as a precursor to AD. In general, subjects with MCI convert to dementia at an annual rate in the range of 10-15% [1]. Approximately 80% of aMCI patients progress to AD dementia within 6 years [2]. Predicting who among a group of aMCI patients are most likely to further decline in cognition would enable clinicians and researchers to identify individuals for early intervention, patient education, as well as the designing clinical trials. The list of risk factors for the progression from MCI to AD dementia include advanced age [3-5], severity of cognitive impairment [6], apolipoprotein E ε4 (APOE ε4) carrier status [7-10], structural and functional changes of brain [11-16], cerebrospinal fluid (CSF) changes [17-19], and positive amyloid imaging [20, 21].
The medial temporal lobe (MTL) structures and frontal lobes generally play different, but complementary roles in episodic memory; encoding and retrieval respectively [22]. Since encoding failure with poor recognition is characteristic of memory impairment seen in AD, we hypothesized that aMCI-E is more likely to progress to AD than aMCI-R. However, the value of aMCI-E to predict the conversion to AD dementia has rarely been studied. Thus far, only a few studies have investigated the clinical significance of these different patterns of memory impairment in aMCI according to recognition performance [23, 24] and their potential use to predict the progression to AD dementia [25].
In this analysis, we divided aMCI into two subtypes according to the recognition patterns. One is aMCI with poor encoding and poor retrieval (aMCI with encoding failure, aMCI-E), and the other is aMCI with poor encoding but preserved recognition/retrieval (aMCI with retrieval deficit, aMCI-R). We compared baseline characteristics including neuropsychological, genetic, CSF biomarkers, and conversion rate between two subgroups of aMCI and also investigated the relation between aMCI-E and the known prognostic factors for conversion to AD dementia.
MATERIALS AND METHODS
1. Subjects
Data used in the preparation of this article were obtained from the Alzheimer's Disease Neuroimaging Initiative (ADNI) database (adni.loni.ucla.edu). The ADNI was launched in 2003 by the National Institute on Aging (NIA), the National Institute of Biomedical Imaging and Bioengineering (NIBIB), the Food and Drug Administration (FDA), private pharmaceutical companies and non-profit organizations, as a $60 million, 5-year public-private partnership. The primary goal of ADNI has been to test whether serial magnetic resonance imaging (MRI), positron emission tomography (PET), other biological markers, and clinical and neuropsychological assessment can be combined to measure the progression of mild cognitive impairment (MCI) and early Alzheimer's disease (AD). Determination of sensitive and specific markers of very early AD progression is intended to aid researchers and clinicians to develop new treatments and monitor their effectiveness, as well as lessen the time and cost of clinical trials.
The Principal Investigator of this initiative is Michael W. Weiner, MD, VA Medical Center and University of California - San Francisco. ADNI is the result of efforts of many co-investigators from a broad range of academic institutions and private corporations, and subjects have been recruited from over 50 sites across the U.S. and Canada. The initial goal of ADNI was to recruit 800 adults, ages 55 to 90, to participate in the research, approximately 200 cognitively normal older individuals to be followed for 3 years, 400 people with MCI to be followed for 3 years and 200 people with early AD to be followed for 2 years." For up-to-date information, see www.adni-info.org [26, 27].
A total of 397 subjects with aMCI from the ADNI study were included in the current analysis. MCI subjects fulfilled criteria for aMCI [28]: nondemented subjects with memory complaint (global CDR score=0.5, with a Memory Box score ≥ 0.5), MMSE score of 24 to 30, a Modified Hachinski Ischemic Score [29]≤4, a Geriatric Depression Score [30] (GDS, short form)<6, and preserved IADL. Subjects performed at an objective cut-off of 1.5 standard deviations (S.D.) below education-adjusted cut-off scores on the Logical Memory IIa of the Weschler Memory Scale-Revised [31].
2. Psychometric testing
The assessment relevant to this analysis included the MMSE, CDR memory box, GDS short form, the Rey Auditory Verbal Learning Test (RAVLT) [32], digit span, Trail Making A and B, category fluency, Boston Naming Test, and clock drawing. The subjects with aMCI were divided into two subtypes according the performance on the recognition test of the RAVLT. The RAVLT consists of five learning trials in which a list of 15 words is read and the subject is asked to immediately recall as many items as possible. After interference list of 15 novel words is read and recalled, subjects are then asked to recall words from the initial list (5-minute delayed recall). A 30-minute delayed recall trial and recognition test follow. For the recognition test, subjects are presented with a list of the 15 studied words and 15 non-studied foils and are asked to circle all words previously learned. Subjects who performed below an objective cut-off of 1.5 standard deviations were classified into aMCI with encoding failure, aMCI-E, while those performed above a cut-off of 1.5 S.D. fell into aMCI with retrieval deficit, aMCI-R.
3. Statistical analysis
Independent t-test to compare means, the Mann-Whitney test to compare nonparametric data, the chi-square test was used to test the differences in frequency between two subgroups were used. Odds ratio was calculated to describe the strength of association between the aMCI subtypes and the conversion to dementia, and the logistic regression for adjusted odds ratio was performed to predict the conversion to AD dementia from a number of predictor variables which showed the difference between two subgroups. The Spearman's rs test of correlation was used to measure the degree of relationship between aMCI subtypes and the prognostic factors for progression to AD dementia which were found to be statistically different between subtypes of aMCI in this study. Statistical analyses were performed using SPSS® Version 19.0 for Windows.
RESULTS
1. Demographics and CSF biomarker profile of aMCI subgroups
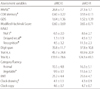
Among the 397 subjects with aMCI, 209 (52.6%) subjects were classified into aMCI-E and 188 (47.4%) into aMCI-R. Subjects with aMCI-E were younger and had lower MMSE score and higher CDR Memory score compared to those with aMCI-R. The proportion of the individuals with APOE ε4 was also significantly higher in aMCI-E group than aMCI-R group. CSF Aβ and tau assay was available in 199 subjects from two groups (106 vs. 93) for aMCI-E and aMCI-R respectively. CSF Aβ42 level was significantly lower and Tau and P-Tau181P levels were significantly higher in aMCI-E group than aMCI-R group (Table 1).
2. Neuropsychological assessments between the subgroups
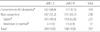
Along with MMSE score and CDR Memory, subjects with aMCI-E showed lower performance than aMCI-R in RAVLT, vegetable category fluency and clock drawing. However, scores from digit span, Trail A and B, animal category fluency, BNT, and clock copy were not different between two subgroups (Table 2).
3. Prediction of progression to AD from aMCI according to subtypes
1) Unadjusted odds ratio
More subjects with aMCI-E (102 subjects, 48.8%) progressed to AD than those with aMCI-R (57 patients, 30.3%) (Odds ratio=2.19 with 95% CI 1.45 to 3.31) during the 3-year follow-up. Individuals with aMCI-R were more likely to remain stable or revert to normal cognition from aMCI (69.7%) than those with aMCI-E (51.2%) (Table 3).
2) Adjusted odds ratio by logistic regression
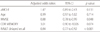
A logistic regression was performed with diagnostic conversion from aMCI to AD as the dependent variable and aMCI subtypes, age, MMSE scores, CDR Memory, and delayed recall on RAVLT as predictor variables. A total of 397 subjects were analyzed and the full model significantly predicted conversion (omnibus chi-square=49.27, df=5, p<0.001). The model accounted for 66.0% of predictions for conversion. However, probability value of aMCI-E was negated and resulted in the odds of conversion by a factor of 1.47 (95% CI 0.89-2.43). Only MMSE score and RAVLT delayed recall reliably predicted the conversion with the odds of 0.88 (95% CI 0.78-0.99) and 0.84 (95% CI 0.76-0.92), respectively (Table 4).
4. Correlations between aMCI subtypes and other prognostic factors
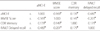
There were weak to moderate correlations between recognition performance and MMSE, CDR Memory, and RAVLT delayed recall (rs=-0.169, 0.139, -0.480, respectively, N=397, p<0.01, two-tailed) (Table 5). There was also a significant but weak negative correlation between recognition performance and CSF P-Tau181P/Aβ42 (rs=-0.281, N=199, p<0.01, two-tailed). There was also a significant but weak negative correlation between recognition performance and APOE genotypes (rs=-0.137, N=397, p<0.05, two-tailed).
DISCUSSION
Barbeau et al [23]. assessed the relative loss of cortical gray matter in aMCI patients with impaired recall but different recognition performances on visual recognition memory. Using a cut-off of 1.5 S.D. below the mean of control subjects, 16 out of 28 (57%) subjects were classified into aMCI-E and 12 (43%) into aMCI-R. Although they used visual memory test, the proportion of aMCI-E is similar to our study. The aMCI subjects with impaired recognition (aMCI-E) had gray matter loss in the right temporal and bilateral temporoparietal regions which is a pattern seen in early AD dementia, and gray matter loss was confined to frontal areas in aMCI with preserved recognition (aMCI-R). These findings suggest that the different profiles in memory impairment in aMCI patients may have different clinical implications. The cross-sectional nature of this study limits its utility in determining conversion rate to AD.
Jeong et al [24]. subdivided aMCI into retention deficit vs. retrieval deficit but did not find any statistically significant difference except hypertension. Among 62 patients, 41 (66%) were classified into aMCI-E and 21 (34%) into aMCI-R using a cut-off of 1.0 S.D. on verbal memory test. However, when we used a 1.0 S.D., 67% of aMCI subjects were classified into aMCI-E and 33% into aMCI-R, quite similar to those by Jeong et al. We used a rather conservative cut-off of 1.5.S.D., as in other previous studies using ADNI data [2, 33]. Using a cut-off of 1.0 S.D. did not change the probability value of aMCI-E to predict progression to AD and only MMSE score and RAVLT delayed recall reliably remained statistically significant like analysis using a 1.5 S.D. cut-off.
Rabin et al [25]. characterized the relative ability of memory tests to predict the progression from aMCI to AD over follow up for 4 years. Although the small sample size made the interpretation cautious regarding statistical power and generalization, logical memory recognition best predicted the progression to AD. In other words, this finding may indirectly imply that not all subjects with aMCI-E convert to AD dementia and aMCI-R may also progress to AD dementia.
In contrast to our hypothesis, the current analysis did not reveal that aMCI-E is an independent risk factor of progression to AD dementia although univariable analysis showed that odds ratio of aMCI-E to predict progression is 2.19. But there were significant correlations between aMCI-E and the severity of memory and global cognition, CSF biomarkers, and APOE ε4 genotype. This may imply that aMCI-E itself is not as strong as other known factors to be a prognostic factor. As aMCI-E, age which is one of known risk factors of progression to AD dementia did not have prognostic value. This may be ascribed to younger age of aMCI-E subjects than those with aMCI-R.
As mentioned earlier, the ADNI is devoid of aMCI subjects with vascular risk factors as indicated in the inclusion criteria with a Modified Hachinski Ischemic Score≤4. This may account for relative preservation of frontal executive function in aMCI-R patients in this study. Because aMCI is a heterogeneous condition even in terms of course and etiology, excluding those subjects with vascular risk factors will limit the generalizability of the results from this analysis to the aMCI population.
Interestingly, even in the current study which lacks vascular MCI subjects, 57 subjects (about 36%) among the 159 aMCI patients who progressed to AD dementia had aMCI-R. This consolidates the earlier point that aMCI-R is heterogeneous in terms of recognition performance on memory tests as well.
There have been debates regarding the progression of aMCI subtypes depending on the involvement of only memory function or other cognitive domains. Some evidence indicates that single domain aMCI places one at highest risk for conversion to dementia [34, 35], whereas other evidence suggests that multiple domain aMCI appear to be at greatest risk for future dementia [36-38]. The latter studies suggest that multiple domain aMCI is a transitional stage lying between single domain aMCI and AD dementia. In the current study, subjects with aMCI-E showed lower performance on vegetable category fluency and clock drawing compared to those with aMCI-R. This finding is partly supported by Barbeau et al. who showed that in aMCI-E gray matter loss was seen in the bilateral parietal lobes and left superior temporal gyrus when compared to aMCI-R, although their study used visual memory test [23]. Lower performance on vegetable category fluency and clock drawing in aMCI-E patients may indirectly imply that this group may have more individuals with multiple domain aMCI through spread of lesions to lateral temporal and parietal cortical areas, although the current analysis was not stratified according to single versus multiple domain involvement. We expect that we can get more generalizable results if we analyze the data which are not exclusive of vascular etiology for aMCI. Considering significant correlation between aMCI-E subtype and other prognostic factors for progression to AD dementia, aMCI-R may progress to involve other cognitive domains resulting in aMCI-E.
In conclusion, although this study did not show that aMCI-E subtype has statistically significant probability value to independently predict the progression of aMCI to AD dementia, aMCI-E subjects tend to be younger, with lower MMSE and higher CDR memory score compared to those with aMCI-R. aMCI-E also significantly correlated with other variables which have been known to be the prognostic factors for progression to AD. This may imply that aMCI-E subtype might be a later stage of aMCI residing between the aMCI-R and the early AD dementia, while aMCI-R might be an earlier stage of aMCI which would be a better target for therapeutic intervention than aMCI-E given that the importance of early identification of MCI, particularly aMCI, and effective early therapeutic intervention have been emphasized. However, alternative explanation for this is also possible. Pathologies of aMCI-E subtype may be closer than those of aMCI-R to AD pathology. Pathologies of aMCI-R may have more frontal dominant pathologies that those of aMCI-E, such as frontotemporal lobar degenerations other than depression and subcortical vascular pathologies which were excluded in ADNI.
This suggested hierarchy of disease stages or pathologic differences between these two subtypes of aMCI need to be validated through intraindividual longitudinal assessment of decline in recognition performance and by structural and functional studies, particularly amyloid imaging. We also expect that stratification of aMCI according to number of impaired domains using data from cohort including vascular MCI may shed more light on this topic.

 XML Download
XML Download