

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Mycoplasma pneumoniae (MP) is the most common pathogen of community-acquired pneumonia in school-aged children and adolescents and is usually a benign self-limited disease; however, some cases are known to develop severe life-threatening pneumonia with acute respiratory failure. A case report of acute respiratory failure due to mycoplasma is more rare in children than adults. The exact incidence, risk factors, and prognoses of acute respiratory failure in children have not yet been reported. MP is reported to progress to acute respiratory distress syndrome (ARDS) requiring mechanical ventilation in approximately 0.5–10.9% of all adult and geriatric patients hospitalized due to MP.12) Some children can recover from acute respiratory failure345); however, it can lead to death when accompanied by multiple organ failure.67) Herein, we report a case of fatal pneumonia caused by MP with ARDS and multiple organ involvement in a school-aged boy who recovered after being treated with extracorporeal membrane oxygenation (ECMO) and continuous renal replacement therapy (CRRT).
CASE
An 8-year-old boy who presented with an acute condition and difficulty of breathing visited the emergency department of our institution. He had been diagnosed with autism and was attending a special-education school. Although the patient had been diagnosed with asthma, he had never undergone appropriate treatment for it. The patient had had a fever without any evident respiratory symptoms within 1 week prior to the visit. He had been diagnosed with acute pharyngotonsillitis and treated with antibiotics of unknown type. Although he did not have fever afterward, he tended to fall asleep and seemed to lack energy at school and had breathing difficulty; hence, he visited our hospital. At the time of visit, a stridor sound when breathing, cough, and phlegm were noted. During the physical examination, tachypnea (respiratory rate >36/min) and lethargy were observed. Wheezing and rales were heard in both lungs upon auscultation. Percutaneous oxygen saturation (SpO2) was only 88% when measured while administering oxygen at a high concentration of 10 L/min. The patient did not respond to short β2-agonist bronchodilator (Ventolin®; GlaxoSmithKline, Brentford, UK) and glucocorticoid inhalation therapy. Initial chest X-ray scans showed diffusely increased opacity and moderate pleural effusion in both lungs (Fig. 1).
 | Fig. 1Chest radiographic changes (A) Diffuse increased opacity in both lower lobe, pleural effusion both at admission (HD#1). (B) Diffuse increased opacity, right lung, consolidation in left upper lobe and left lower lung zone after ECMO catheter removal (HD#18). (C) Atelectasis in the central portion of left upper lobe before discharge (HD#105). (D) Diffuse bronchial wall thickening in both lungs, and suspicious peribronchial infiltration in right lower lobe (326 days after discharge).Abbreviation: HD, hospital day; ECMO, extracorporeal membrane oxygenation.
|
The results of the initial venous blood gas analysis performed at the time of visit were as follows: pH, 7.27; partial pressure of CO2, 44 mmHg; partial pressure of oxygen, 70 mmHg; bicarbonate, 20.2 mEq/L; base excess, −6.5; SpO2, 91% (100% oxygen administered at 10 L/min); white blood cell (WBC) count, 17,100/µL (segment neutrophil 82.1%) indicative of leukocytosis; and C-reactive protein, 15.0 mg/dL. The serum aspartate aminotransferase (AST) level was 6,536 U/L; alanine aminotransferase (ALT), 1,083 U/L; blood urea nitrogen (BUN), 22.0 mg/dL; and creatinine (Cr), 0.96 mg/dL (Table 1). Under the suspicion of pneumonia caused by bacteria or MP infection, cefotaxime and clarithromycin were intravenously administered, and ventilator care was started. However, even with the ventilator setting with the pressure control (assist control mode), positive end expiratory pressure (PEEP) of 12 mmHg, peak inspiratory pressure (PIP) of 20 mmHg, fraction of inspired oxygen (FiO2) of 100%, and respiratory rate (RR) of 24/min, the oxygen index was 22.0 and oxygen saturation index was 16.5, which indicates severe ARDS. The pulse oximeter showed SpO2 of ≤92%, and lung parenchymal infiltration worsened. On hospital day 2, echocardiography was performed due to ARDS and multiple organ failure affecting the liver and kidneys. After confirming that the patient had a normal cardiac function, veno-venous (right common femoral vein drainage and right internal jugular vein infusion) ECMO was administered. A mycoplasma serology test performed upon admission showed mycoplasma immunoglobulin (Ig) M (+, 5.1; positive ≥1.1 index, ELISA; DIESSE, Siena, Italy), IgG (+, 100 AU/mL, positive ≥18 AU/mL, ELISA; DIESSE), and cold agglutinin 1:256. In the MP polymerase chain reaction (PCR) test (Seeplex® PneumoBacter ACE Detection (V3.0); Seegene Inc., Seoul, Korea) from transtracheal aspirates, the patient tested positive for MP (Table 2). The lactate dehydrogenase (LDH) level was elevated above the maximum normal limit (11,000 U/L) (Table 1). On hospital day 2, serum concentration levels of IgG, IgA, IgM, and IgE were 338 mg/dL (reference range, 608–1,572 mg/dL), 38 mg/dL (reference range, 43–207 mg/dL), 46 mg/dL (reference range, 33–236 mg/dL) and 11.1 IU/mL (reference range, 0–230 IU/dL). In addition, 400 mg/kg/day of intravenous IgG was administered for 5 days (total 2 g/kg/day). Chest tube insertion was performed due to pleural effusion that persisted in both lungs for 2 hospital days. In a pleural fluid test, a serosanguinous colored fluid was drained from the both lungs (pleural fluid analysis results: red blood cell 70,000/μL, WBC 190/μL, polymorphonuclear neutrophil 80%, pH 7.6, glucose 99 mg/dL, and protein 3.3 g/dL). A culture of the pleural fluid did not grow any organisms. After the use of ECMO, azotemia, Cr, LDH, and blood cytokine levels started to increase on hospital day 2, and CRRT was performed. ECMO was used for a total of 17 days and was weaned on hospital day 18 without any complications (Fig. 2). CRRT was weaned on hospital day 34 after monitoring the urine output. The maximum serum Cr level was reached on hospital day 7 (4.29 mg/dL). AST level increased up to 10,258 U/L on hospital day 3, and ALT level increased up to 1,447 U/L on hospital day 2. On hospital day 11, improvements on simple chest radiographs were noted, and the pleural effusion also appeared to improve. The chest tubes were removed from the left lung on hospital day 17 and from the right lung on hospital day 22. ECMO was removed after observing stable blood gas levels on hospital day 18. The patient was continuously treated with a mechanical ventilator with the following settings: pressure control (assist control) mode, PEEP 10 mmHg, PIP 18 mmHg, RR 20/min, and FiO2 55%.
Table 1
Laboratory test result changes
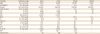
Abbreviation: HD, hospital day; WBC, white blood cell; AST, aspartate aminotransferase; ALT, alanine aminotransferase; LDH, lactate dehydrogenase; BUN, blood urea nitrogen; Cr, creatinine; CRP, C-reactive protein; PT, prothrombin time; aPTT, activated partial thromboplastin time; FDP, fibrin degradation product.
![]()
Table 2
Test results for mycoplasmal infection

![]()
 | Fig. 2Progression of the patient's condition and treatment.Abbreviation: Ig, immunoglobulin; ECMO, extracorporeal membrane oxygenation; CRRT, continuous renal replacement therapy; HD, hospital day.
|
Due to poor response to antibiotic treatment, cefotaxime was changed to meropenem, and multidrug-resistant Acinetobacter baumannii was noted from tracheal aspirate cultures on hospital day 11. Endotracheal extubation was consistently attempted, but antibiotics had to be continuously used due to fever. Antibiotics were used due to repeated atelectasis and hospital-acquired infection (multidrug-resistant A. baumannii was isolated in the transtracheal aspiration on hospital day 12 and Candida albicans was isolated in the transtracheal aspiration and urine culture on hospital day 31), and weaning failure persisted. For effective lung care, tracheostomy was performed on hospital day 43, and the patient was transferred to a general ward on hospital day 52 to continue the treatment. The patient underwent pulmonary rehabilitative therapy, and the tracheal tube was removed on hospital day 101. In the last blood test performed before discharge, the patients blood component levels were found to have returned to normal with BUN of 14.7 mg/dL and serum Cr of 0.27 mg/dL. The serum AST and ALT levels were also decreased to 39 and 65 IU/mL, respectively. Although kidney sonography revealed mildly increased echogenicity of its cortex on hospital day 15, no evidence of kidney injury was found in a test performed before discharge. Brain magnetic resonance imaging (MRI) performed on hospital day 111 did not show any evidence of ischemic injury, infarction, or hemorrhage. The patient was discharged without respiratory support on hospital day 113. The patient was continuously treated with Ventolin® (GlaxoSmithKline), budesonide, and inhalation therapy after discharge.
DISCUSSION
MP pneumonia may improve without treatment and is effectively treated with macrolides. However, fulminant cases including ARDS have been reported.89)
Patients with MP pneumonia have shown extrapulmonary symptoms such as hemolysis, skin reactions (e.g., Steven Johnson syndrome), and central nervous system complications. The patient in this case report showed kidney and liver symptoms as well as multiple organ failure.
The immune mechanism is important in the pathogenesis of MP pneumonia. The host-cell immune response has been reported to play an important role in the occurrence of MP pneumonia in patients with severe pneumonia.10) Lymphocytes that have been sensitized from an early infection become activated when the next infection occurs and secrete an excessive amount of mediators. These mediators destroy local tissues and induce a series of inflammatory responses, suggesting that an excessive host-cell response against microorganisms can cause lung damage. In the present case, long-term infection can cause a marked increase in the levels of inflammatory markers such as LDH.
A case report of ARDS due to mycoplasma is more rare in children than adults. It has been reported in adolescent aged 12, 14, and 17 years in Korea.56) Children who had ARDS only without multiple organ failure showed relatively good outcomes.5) However, a high mortality rate was observed in cases of ARDS accompanied by multiple organ failure or ARDS quickly progressed to become fulminant.6) It is also more commonly reported among younger adults than among older adults.
Cellular immunity is considered important in the etiology of Mycoplasma infection, early-phase impairment of cellular immunity may be correlated to the etiology of fulminant MP pneumonia.11)
Although case reports have been intermittently published, one study analyzed the clinical manifestations of fulminant MP pneumonia (defined as the apparent presence of MP infection with hypoxia) in 52 patients.11) Most patients (72.5%) were young adults without underlying diseases (52% of MP pneumonia occurred in patients aged ≤49 years). About 15% had chronic bronchitis, asthma, or pulmonary disease. Although the study could not clearly identify the risk factors of MP pneumonia as it was a small retrospective study, it suggested that an inappropriate antibiotic therapy be performed in the early period of infection as a possible risk factor if early antibiotic therapy was unsuccessful. For this reason, an early diagnosis of MP pneumonia using PCR and serological tests is important.12)
Early administration of steroids, which are cellular immunity inhibitors, in addition to anti-mycoplasma is necessary to treat fulminant MP pneumonia.11) The progression of MP pneumonia, which does not respond well to antibiotic therapy, appears to be associated with cellular immune response,1314) which may be inhibited by steroids to reduce lung damage.15) Meduri et al.16) and Radisic et al.13) reported that the use of steroids could potentially be effective in ARDS. Studies have also reported improvements in lung infiltration and clinical symptoms such as fever following steroid administration in patients who were resistant to macrolides, which is a drug of choice for MP pneumonia, or who showed no response to macrolides and eventually developed fulminant MP pneumonia (although it was not possible to find whether MP pneumonia progressed to fulminant MP pneumonia without a response to macrolide administration or MP pneumonia progressed to fulminant MP pneumonia regardless of macrolide administration).8) Researchers claim that empirical steroid therapy must be considered for respiratory failure.8) A treatment progress may be shortened by using high-dose therapy.5) However, although the patient in this case report was treated with high-dose steroids in the early period, we could not investigate its effects.
The patient had asthma; therefore, identifying whether appropriate antibiotic therapy had been performed in the early period is not possible. However, macrolide administration was immediately started upon admission to our institution, and steroid pulse therapy was performed at hospital day 2 (30 mg/kg, 3 days); however, improvements after the treatment were not assessed. The patient also exhibited hypoxia due to respiratory failure and required mechanical ventilation, which may have negatively affected the treatment outcomes. However, the early use of ECMO and CRRT appeared to improve the treatment outcomes. The patient showed a large increase in serum AST/ALT that persisted for a longtime period and suggested inflammation. ECMO was immediately performed, and an increase in total bilirubin levels was observed afterward. Thus, it was impossible to assess if the patient had impaired renal function. The patient showed a slight increase in BUN/Cr at the time of admission, but his amount of urine did not decrease, and further damage to the kidney could be prevented by the early use of CRRT. The patient had autism, and the asthma symptoms he usually experienced were likely not detected or treated. In addition, recognizing the symptoms of MP pneumonia might have been difficult, and the patient must have missed the timing for early treatment as MP pneumonia had already progressed.
ECMO is a technique developed to ensure adequate oxygen delivery in patients with cardiovascular or respiratory failure.17) Determining the timing for ECMO for acute respiratory failure is difficult. In general, a mechanical ventilation period of over 710 days is considered a relative contraindication for ECMO because of the high possibility of iatrogenic lung cancer or irreversible lung disease. Therefore, immediately determining whether to perform ECMO or not is associated with the patient's prognosis. For children, an oxygen index may be used as a good marker of ECMO adaptation. Mortality rates of 6180% have been reported when conservative treatments including high-frequency oscillatory ventilation were performed with an oxygen index of ≥40.18) ECMO has been used as an early rescue therapy for pediatric patients with ARDS. It has also been used as a rescue therapy for over 20 years with reported survival rates of 50% in children with acute lung injury/ARDS.19) ECMO must be considered when no improvements are observed after conventional ventilator therapy in children with ARDS caused by bacterial and viral infections that may result in pneumonia.
CRRT is becoming increasingly used to support patients with acute renal failure. It is indicated for hemodynamically unstable pediatric patients with hypervolemic anuric acute renal failure, electrolyte abnormalities, and multiple organ failure, or catabolic patients with increased nutritional needs and hyperammonemia. Non-renal indications include significant organ edema, especially lung, ARDS, fulminant hepatic failure, sepsis, systemic inflammatory response syndrome, lactic acidosis, and multiple organ failure.20) In this case report, CRRT may have been useful for treating acute kidney injury and for removing inflammatory mediators that were produced as a result of severe infection and inflammation. The combination of CRRT and ECMO is an effective and safe treatment to alleviate fluid overload and improve kidney function in pediatric patients with cardiopulmonary failure.21)
Severe MP pneumonia can lead to pulmonary sequelae with or without intensive care.22) The incidence of pulmonary sequelae such as atelectasis, bronchiectasis, and bronchiolitis obliterans has been reported in up to 21% of cases.23) In the present case report, the patient showed signs of bronchiolitis obliterans on computed tomography (Fig. 3. B and C). In addition, difficulties with weaning were noted due to the lack of cooperation from the patient, who was autistic, and the patient was admitted to the intensive care unit and had to undergo ventilator therapy for a long-time period, which may have led to more lung damage.
 | Fig. 3Chest computed tomographic changes (A) Atelectasis in the posterior segment of both upper lobe; superior, posterior, and lateral basal segments of right lower lobe and right middle lobe; lingular division of left upper lobe; and superior and anteromedial basal segment of left lower lobe. Multifocal intrathoracic loculated air (HD#37). (B) Diffuse mosaic attenuation in both lungs, diffuse bronchial wall thickening in right upper lobe and both lower lobe (HD#111). (C) Multifocal subsegmental/linear atelectasis in both lungs, diffuse bronchial wall thickening in left lower lobe (326 days after discharge).Abbreviation: HD, hospital day.
|
There were no ischemic injury, infarction, or hemorrhage in the brain MRI performed before discharge. This is the first reported case of ARDS due to MP infection complicated by multiple organ failure successfully treated with ECMO and CRRT in Korea, with recovery of kidney and liver function, and without neurologic sequelae.
 XML Download
XML Download