

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Mycoplasma pneumoniae (MP) is a frequent cause of community-acquired pneumonia in children. Although patients with MP pneumonia typically have a benign clinical course, some patients can experience refractory or severe pneumonia. Additionally, although the pathogenesis underlying MP pneumonia is not fully understood, it has been reported that various cytokines and chemokines may be associated with lung injury in MP infection.1) Although widespread dissemination of macrolide-resistant strains during epidemics is thought to cause macrolide-nonresponsive or refractory MP pneumonia, hyper-immune reactions with cytokine overproduction may be involved in the severe conditions.23)
In MP infection, role of various cytokines and chemokines have been investigated including interleukin (IL)-1, IL-2, IL-4, IL-6, IL-8, IL-10, interferon (IFN)-γ, and tumor necrosis factor (TNF)-α.1) Among the cytokines, IL-18 is a member of the IL-1 family of cytokines and plays an important role in the T-helper type 1 immune response.45) Moreover, the serum levels of IL-18 and IFN-γ-inducible protein-10 (IP-10) have been reported to correlate significantly with the severity of MP pneumonia.6789)
The aim of this study was to evaluate the relationships between cytokine and chemokine levels and the clinical severity of MP pneumonia in children.
MATERIALS AND METHODS
1. Patients
Pediatric patients admitted to the Dongsan Medical Center with MP pneumonia from August 2011 to May 2012 were included in this study. Pneumonia was diagnosed based on both clinical and radiological findings. MP pneumonia was identified using an indirect enzyme-linked immunosorbent assay (ELISA, RIDASCREEN kit; R-Biopharm, Darmstadt, Germany) for specific immunoglobulin M antibodies in the first and/or second sample, with a concentration of >71 units/mL defined as positive according to the manufacturer's instructions.
2. Clinical parameters
With regard to clinical parameters, the demographic findings of age and sex, pre-admission and total fever durations, pneumonia pattern of patients, proportion of cases receiving corticosteroids or oxygen, and hospitalization duration were evaluated.
The severity of the disease was assessed using 2 clinical parameters; the chest radiographic pneumonia patterns and the use of systemic corticosteroids. All patients were treated with antibiotics, including a macrolide (clarithromycin), and received other supportive management, such as intravenous hydration, nasal oxygen supply, and bronchodilator inhalation, as needed. Corticosteroids were administered to patients who exhibited persistent tachypnea, decreased aeration, or abnormal lung sounds despite previous management.10) According to the chest radiographic infiltration results, patients were divided into two groups; the lobar pneumonia group and the broncho-interstitial pneumonia group.
This study was approved by the Institutional Review Board of the Keimyung University Dongsan Medical Center (approval number: 2016-08-024).
3. Laboratory parameters
Blood samples were collected at admission, and the resultant serum samples were stored at −80°C until analysis. Serum levels of IL-6, IL-8, IL-10, IL-18, IP-10, macrophage inflammatory protein-1β, and TNF-α were measured using a multiplex assay with the instrument Luminex® 200™ Total System (Luminex Corporation, Austin, TX), according to the manufacturer's instructions.
Other parameters analyzed included the white blood cell count with proportions of neutrophils and lymphocytes, erythrocyte sedimentation rate (ESR), and serum levels of C-reactive protein (CRP), aspartate aminotransferase, alanine aminotransferase, and lactate dehydrogenase (LDH). Chest X-rays were performed at admission, and the pneumonia patterns were determined by a single pediatrician (Hee Joung Choi). The real-time reverse transcription polymerase chain reaction assay for detecting the metapneumovirus, adenovirus, parainfluenza virus, influenza virus, coronavirus, rhinovirus, and respiratory syncytial virus was performed with nasal swabs (RV 12 ACE Detection; Seegene, Seoul, Korea).
4. Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA), with all values reported as frequencies and medians including the range. Categorical variables were compared using the χ2 test and continuous variables using the unpaired t-test or the Mann-Whitney U test, depending on the normality of the distribution. Correlations between the fever duration and cytokine and chemokine levels were analyzed by the Spearman correlation test. A P-value of <0.05 was considered statistically significant.
RESULTS
1. Comparison according to chest radiographic findings
This study enrolled 72 patients (37 females and 35 males) with a median age of 3.9 years (range, 1–16 years). According to the patients' chest radiographic results, there were 29 (40.3%) patients in the lobar pneumonia group and 43 patients (59.7%) in the broncho-interstitial pneumonia group (Table 1). The age of the lobar pneumonia group was more than that of the broncho-interstitial group (age 5.0 vs. 3.0 years, P=0.001). The median pre-admission and total fever durations (6.0 vs. 2.0 days and 8.0 vs. 3.0 days, respectively, both P<0.001) were longer in the lobar pneumonia group than in the broncho-interstitial pneumonia group. There were no significant differences in the number of cases requiring oxygen administration, rate of steroid use, and duration of hospitalization between the 2 groups. The neutrophil differential (P=0.003), ESR (P=0.010), and serum CRP (P<0.001) and IL-18 (P=0.015) levels were significantly higher in patients with lobar pneumonia than in those with broncho-interstitial pneumonia (Fig. 1).
Table 1
Clinical and laboratory findings of the patients
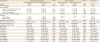
Values are presented as number (%) and median (range).
Abbreviations: ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; LDH, lactate dehydrogenase; IL, interleukin; IP, interferon-γ-inducible protein, MIP, macrophage inflammatory protein; TNF, tumor necrosis factor.
![]()

2. Comparison according to steroid treatment
Of the 72 patients, 31 (43.1%) were treated with systemic steroids and 41 (56.9%) were not. There were no significant differences in age, sex, and the total and pre-admission fever duration between these two groups (Table 1). Corticosteroid-treated patients had a higher incidence of oxygen administration (45.2% vs. 0.0%, P<0.001) and a significantly longer median duration of hospitalization (5.5 vs. 4.0 days, P<0.001). There were no differences in the cytokine and chemokine levels between the groups (Table 1).
3. Levels of cytokine and chemokine according to fever duration
Correlation analyses indicated that the ESR (ρ=0.428, P<0.001), CRP (ρ=0.373, P=0.001), LDH (ρ=0.283, P=0.023), IL-18 (ρ=0.399, P=0.001), and IP-10 (ρ=0.364, P=0.002) serum levels were significantly positively correlated with the fever duration prior to admission (Fig. 2).
 | Fig. 2Correlation between pre-admission fever duration and laboratory findings. Significant correlations were found between pre-admission fever duration and ESR (A), CRP (B), LDH (C), IL-18 (D), and IP-10 (E).Abbreviations: ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; LDH, lactate dehydrogenase; IL, interleukin; IP, interferon-γ-inducible protein.
|
4. Correlations between laboratory findings
Among the examined parameters, there were positive correlations between the IL-18 and ESR (ρ=0.368, P=0.002), IL-18 and CRP (ρ=0.410, P<0.001), and IP-10 and LDH serum levels (ρ=0.371, P=0.003) (Fig. 3).
 | Fig. 3Correlation among the cytokines. Significant correlations were found between the IL-18 and ESR (A), IL-18 and CRP (B), and IP-10 and LDH serum levels (C).Abbreviations: ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; LDH, lactate dehydrogenase; IL, interleukin; IP, interferon-γ-inducible protein.
|
DISCUSSION
In the present study, we found that patients with lobar pneumonia patterns had higher CRP, ESR, and IL-18 serum levels, suggesting that more severe systemic inflammation occurs in this type of pneumonia in MP infection. In addition, the serum levels of CRP, ESR, LDH, IL-18, and IP-10 were positively correlated with the fever duration prior to admission. And the ESR and CRP levels were positively correlated with the IL-18, and LDH, with IP-10 levels.
Previous studies have also reported that pro-inflammatory cytokines, such as IL-1, IL-2, IL-6, IFN-γ, and TNF-α, and anti-inflammatory cytokines, such as IL-4 and IL-10, were positively correlated with the severity of pneumonia.1112) In particular, IL-18, which is produced early during host responses to microbial and fungal pathogens,1314) was found to be increased in patients with severe MP infection,71516) including cases of massive pleural effusion and fibrotic lung changes.15) IL-18 levels were reported to positively correlate with IL-2 levels and the number of affected pulmonary lobes.16) Higher levels of IL-8, which promotes neutrophil infiltration, have been reported in the bronchial lavage fluid or pleural fluid of patients with MP infection.1718) However, cytokine studies on refractory or macrolide-resistant MP infection in children and adults have reported inconsistent results.7192021) Since, the high level of cytokines might not be reflected by the macrolide resistance genotype, but by the severity of inflammation, such as lung lesions and prolonged fever durations.22) In the present study, we observed similar results to those described above.
In contrast, the patients who were treated with corticosteroids; presented with severe respiratory symptoms such as tachypnea, wheezing, decreased aeration; and required oxygen administration had no significant differences in their cytokine and chemokine concentrations. The cytokines and chemokines may function primarily at the cellular level and reflect the number of activated immune cells involved in various pathological lesions of diseases, including MP infection. Thus, tiny amounts of serum inflammation-associated cytokines may be easily affected by the stage of MP pneumonia, severity of inflammation, and host response to other local insults in MP pneumonia. Thus, our results may be resulted from early sampling at the initial stage of MP pneumonia before disease progression.
Additional corticosteroids treatment may be effective in the prevention of disease progression and can be administered to reduce inflammatory cytokines.23) Higher LDH levels have been observed in severe or macrolide-refractory MP pneumonia; thus, the LDH level can be used as a biomarker for indication of corticosteroid treatment.24) Several studies have demonstrated a significant positive correlation between the LDH and IL-18 levels with the cut-off values for corticosteroid therapy.7819) In the present study, we found that the LDH level was not positively correlated with the IL-18 level, but was correlated with the IP-10 levels. And the IL-18 level was positively correlated with the ESR and CRP levels.
These findings could be due to our early sampling at the initial stage of MP infection, and LDH elevation may be associated with true lung cell injury in advanced MP and other pneumonia.
This study had several limitations. The number of study participants was small, and the study lacked a control group of healthy children. Additionally, as only one sample was obtained from each patient, we did not evaluate the function of cytokines and chemokines during a self-limited disease course.
In conclusion, we found that the CRP, ESR, LDH, IL-18, and IP-10 serum levels were associated with the severity of the disease, manifesting lobar pneumonia or prolonged fever duration prior to admission. Further studies are needed to evaluate the function of cytokines and chemokines using serial changes in MP infection.
 XML Download
XML Download