

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Following the widespread implementation of the rotavirus vaccine, the incidence of rotaviral enteritis has declined. However, enteritis with a bacterial etiology, such as that caused by Salmonella, Campylobacter, enteropathogenic Escherichia coli, enterohemorrhagic E. coli, is emerging as a major issue in clinical field.1) Recently, the clinical application of polymerase chain reaction (PCR) has contributed to the precise molecular biological diagnosis of infectious agents, facilitating the investigation of detailed clinical presentations leading to therapeutic advancements, from an empirical to a pathogen-specific approach.
Campylobacter species are gram-negative, comma- or S-shaped rods that causes zoonotic infections. They can be transmitted via the fecal-oral route, by person-person contact, or by ingestion of undercooked contaminated poultry, meat, or milk. Campylobacter enteritis was introduced as a new disease by Skirrow2) in 1977, and various studies on Campylobacter enteritis have been published worldwide for over 40 years. Campylobacter infection is known to be a major cause of acute diarrhea. The most common clinical symptoms are fever, bloody diarrhea and colicky abdominal pain. Abdominal pain is continuous, and radiates to the right iliac fossa, mimicking acute appendicitis.3) Most of these studies are confined to adults, and studies in children are limited.
Recent studies have shown a significant increase in the rate of Campylobacter isolated from pediatric enteritis patients, compared with E. coli or Salmonella.
12) However, there have been limited studies that include patient cohort sizes larger than 100 Campylobacter enteritis in children in Korea. The present investigation was undertaken to describe the clinical and laboratory features of Campylobacter enteritis diagnosed at the Nowon Eulji Medical Center (NEMC) over a period of 6 years.
MATERIALS AND METHODS
1. Subjects and specimens
This cross-sectional study was conducted retrospectively at the department of pediatrics in NEMC between January 2012 and December 2017. We obtained stool specimens from the suspicious of gastroenteritis patients with symptoms such as vomiting, diarrhea, fever, or abdominal pain. With the stool specimens, culture or PCR was routinely performed to identify the causative organisms. Subjects of this study were positive for Campylobacter spp. in the test. This study was performed according to the guidelines of Helsinki Declaration and was approved by the Institutional Review Board of NEMC (approval number: 2017-03-002-001).
2. Investigational flow for collected stool specimen
Campylobacter infection was confirmed by using two flows. The first flow involved obtaining a positive confirmation from EnterNet,1) an acute enteritis surveillance program in the Public Health and Environment Research Institute (PHERI), on the basis of the stool culture and PCRs performed on refrigerated stool samples of the patients with suspected gastroenteritis, which were sent once a week. Campylobacter spp. was cultured in mCCDA medium at 37°C for 48 hours to select gray irregular colonies for further identification. In this flow, both bacterial cultivation and PCR testing were performed in EnterNet, an acute enteritis surveillance program. The results of EnterNet were obtained from the PHERI (Table 1). More information on EnterNet can be found in the previous paper.1) In the second flow, multiplex PCR (Acute bacterial diarrhea screening test®; Greencross Reference Laboratory, Yongin, Korea) was performed at the request of clinicians when they suspected bacterial enteritis since March 2014. Nine bacterial pathogens were detected using the Seeplex Diarrhea-Bacteria ACE Detection kit (Seegene Inc., Seoul, Korea) (Table 2). In some cases, neither methods were performed because of failings in securing stool specimens.
Table 1
Isolation rate of bacterial pathogens over 6 years (2012–2017) from Nowon Eulji Medical Center stool samples submitted to the EnterNet surveillance systems
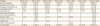
Values are presented as number of patients (%).
*Viral causes are Rotavirus, Norovirus, Adenovirus, and Sapovirus.
![]()
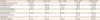
Table 2
Isolation rate of bacterial pathogens over 4 years (2014–2017) from Nowon Eulji Medical Center stool samples by multiplex polymerase chain reaction
![]()
3. Review of medical records
The medical records of each patient of Campylobacter enteritis were reviewed, and the following data were collected: age, sex, date of hospitalization or outpatient visit, presence of fever, headache, abdominal pain or vomiting, laboratory results, diagnostic imaging, antibiotic use, outcomes, and concomitant infection.
4. Statistical analysis
Statistical analysis was performed using IBM SPSS version 20.0 (IBM Co., Armonk, NY, USA). Categorial variable were compared using the χ2 test. The Student's t-test was used to compare continouous variables. A P-value of <0.05 was considered statistically significant. The temperature data was provided by the Korea Meteorological Administration. And the monthly average temperature of Seoul for 6 years was estimated.
RESULTS
1. Subject specimen tested via two flows
One thousand three hundred ninety-six samples were obtained from children with acute enteritis from 2012 to 2017, and tested by EnterNet. Among them, the number of multiplex PCR samples is 593 from March 2014 to December 2017. Sixty patients were diagnosed as having Campylobacter enteritis by EnterNet and 110 by the multiplex PCR. After excluding duplicates from the patient lists diagnosed by each flow, 123 patients were finally included in the study.
2. Pathogen distribution in EnterNet
Out of 1,396 stool specimens, enteric viruses were detected in 466 (33.4%) cases by PCR, whereas bacterial pathogens were cultured in 328 cases (23.5%). Specifically, the isolation rates were: 8.4% (n=117) for Staphylococcus aureus, and 4.8% (n=67) for pathogenic E. coli., 4.3% (n=60) for Campylobacter spp., 3.8% (n=53) for Salmonella spp. (Table 1).
3. Pathogen distribution in multiplex PCR
Out of 593 stool specimens, bacterial pathogens were detected in 209 cases (35.2%). Specifically, the detection rates were: 18.5% (n=110) for Campylobacter spp., 6.6% (n=39) for Clostridium perfringens, and 4.9% (n=29) for Clostridium difficile, 2.5% (n=15) for Salmonella spp. (Table 2).
4. Children diagnosed with Campylobacter enteritis
1) Demographics and seasonal distribution
The yearly distribution of the diagnosed cases was as follows: 2 patients in 2012, 7 patients in 2013, 15 patients in 2014, 32 patients in 2015, 41 patients in 2016, and 26 patients in 2017, indicating an increased yearly incidence of infections (P<0.05). The male to female ratio was 1.05:1, with 63 male (51.2%) and 60 female (48.8%) patients. The participants' ages ranged from 0 to 18 years. The median age of patients was 12 years (interquartile range [IQR], 8 to 16 years). Of these, one patient was less than a year-old, 14 patients were aged between 1 and 5 years, 36 patients aged between 6 and 10 years, 40 patients between 11 and 15 years, and 32 patients between 16 and 18 years. Campylobacter enteritis was diagnosed throughout the year, with highest incidence (71 cases, 57.7%) in summer. Between June and September, a total of 87 cases (70.7%) were diagnosed. There was a significant positive correlation between the number of cases of Campylobacter enteritis and monthly mean temperature in Seoul, Korea (r=0.878, P<0.01) (Fig. 1).

2) Clinical presentation
Among the patients with Campylobacter enteritis, 105 cases (85.4%) were inpatients and 18 cases (14.6%) were out-patients. The most common symptoms were diarrhea (120 cases, 97.6%), fever (119 cases, 96.7%) and abdominal pain (116 cases, 94.3%). Other symptoms included vomiting (46 cases, 37.4%) and headache (42 cases, 34.1%). The median duration of diarrhea was 4 days (IQR, 2 to 5 days). In one of three cases without diarrhea, a 14-year-old boy complained of fever, nausea, and abdominal pain but not of diarrhea. Although he was discharged following resolution of his abdominal pain, he reported episodes of loose stools two days later. The remaining four cases without fever included. One of them, a 16-year-old boy was subsequently diagnosed with irritable bowel syndrome (IBS).
Fresh blood was seen in the stool samples of 12 patients (9.8%), including infant patients. A rash was observed in only 2 cases (2.1%). Guillain-Barré syndrome was suspected in 1 patient (1.0%) with muscle weakness. Muscle weakness of the extremities recovered one week after the fever subsided. There were no cases of seizure or paralysis (Table 3).
Table 3
Symptoms of patients with Campylobacter enteritis
![]()
3) Laboratory results
A complete blood count was performed in 117 patients (95.1%). Six outpatients did not have their laboratory tests performed according to the physician's clinical judgment. Median white blood cell (WBC) count was 10,860/mm3 (IQR, 8,565–13,405/mm3); 16.2% patients had WBC count >15,000/mm3. Median C-reactive protein (CRP) level was 5.34 mg/dL (IQR, 2.81–9.1 mg/dL) (Table 4).
Table 4
Laboratory data of patients with Campylobacter enteritis

| Characteristics | Median | IQR |
|---|---|---|
| WBC (/mm3) | 10,860 | 8,565–13,405 |
| CRP (mg/dL) | 5.34 | 2.81–9.1 |
Values are presented as median and IQR. Maximum value during hospitalization or out-patient department was recorded if serum test was run several times.
Abbreviation: IQR, interquartile range; WBC, white blood cell; CRP, C-reactive protein.
![]()
There were 5 cases (4.1%) with alanine aminotransferase over 40 IU/L. The median aspartate aminotransferase and alanine aminotransferase levels were 33 IU/L (IQR, 31–237 IU/L) and 72 IU/L (62–238 IU/L), respectively. All cases were young male adolescents (aged >14 year) who had no history of underlying liver conditions such as fatty liver disease. None of the patients with elevated liver enzymes developed jaundice, and the liver enzyme levels returned to normal after the disease was treated.
Urinalysis was performed in 102 cases. Of these, there were 2 cases (2.0%) of microscopic hematuria and 1 (1.0%) of proteinuria. A 18-year-old boy with both hematuria and proteinuria also developed hypocalcemia and thrombocytopenia. The patient was suspected of post-infectious nephritis but was not confirmed due to further evaluation. Six months later, a follow-up urine analysis showed complete recovery from Campylobacter enteritis. Another 17-year-old boy reported hematuria with any urinary symptoms and lower leg petechiae on follow-up after discharge with full recovery of Campylobacter enteritis. The petechiae disappeared on subsequent follow-up and the patient was referred to the urology department for investigation of the hematuria. This also resolved without any treatment.
Stool occult blood test was positive in 77 cases (89.5%) out of 86 cases. A stool smear was performed in 94 cases. Red blood cells were found in 29 cases (30.9%) and WBCs were found in 52 cases (55.3%).
Additional enteric pathogens were identified in 16 cases (13.0%), including C. perfringens (8 cases), Aeromonas spp. (3 cases), and verocytotoxin-producing E. coli (1 case). There was co-infection with C. difficile and C. perfringens in 1 case and C. perfringens and Aeromonas spp. in 3 cases.
4) Diagnostic imaging
Computed tomography (CT) scanning was performed in 33 patients (26.8%). Of these, 31 patients (25.2%) who complained of aggravating abdominal pain were subjected to abdominal CT scanning: in the emergency room for 23 patients and in the pediatric ward after admission for the remaining eight patients. Majority of 31 patients (28 cases) were young adolescents. Diffuse edematous wall thickening of the colon (19 cases, 61.3%) and reactive mesenteric lymph nodes (17 cases, 54.8%) were the major findings of CT, which were suggestive of enterocolitis. Ultrasonography was performed in 4 cases (3.3%) revealing colitis with reactive lymph nodes in the mesentery. In 2 patients (aged 8 and 18 years) suspected of having appendicitis or perforated appendicitis on ultrasonography, abdominal CT scanning was ordered. All two CT scannings were normal looking appendix, diffuse edematous wall thickening in right side colon.
5) Antibiotic use
Among the 123 cases of Campylobacter enteritis, treatment for symptomatic relief was administered in 42 patients (34.1%), whereas empirical treatment with oral (PO) azithromycin was administered in 46 patients (37.4%) and intravenously (IV) cefotaxime in 30 cases (24.4%). In one case a combination of PO azithromycin and IV cefotaxime was administered.
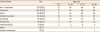
Of 105 hospitalized patients, 33 (31.4%) were treated with PO azithromycin. The mean duration of admission in the azithromycin treated group was 3.9±1.5 days, which was shorter than 4.5±1.5, 4.1±1.5 days in the other antibiotics use group, no antibiotic use group, respectively (P<0.05) (Table 5).
Table 5
Length of stay of admitted patients with Campylobacter enteritis between groups with and without azithromycin use

![]()
6) Outcomes
Among the 123 patients, no one of the children who returned to the hospital through the outpatient or emergency room died or developed a severe disability. Here are some of the unusual symptoms experienced by patients with the Campylobacter enteritis infection.
Gastrointestinal complication: Out of 116 patients with abdominal pain, eight children (8.9%) complained of ongoing abdominal pain after the fever subsided. Of these, five patients were treated conservatively and three were treated with antibiotics other than azithromycin. And a 16-year-old male patient developed IBS during follow-up.
Skin complication: A 9-year-old boy exhibited maculopapular rashes on the palms, soles, and trunk, associated with fever, abdominal pain, and diarrhea. The rashes resolved after treatment. In a 17-year-old male inpatient who was discharged after recovery, petechiae on both lower legs were noticed at one-week follow-up visit. The petechiae disappeared on subsequent follow-up.
Recurrence: One patient had a recurrence of the disease. Eleven-year-old boy was diagnosed with multiplex PCR for the first episode of Campylobacter enteritis and was treated with oral azithromycin on outpatient base. Two months later, he was admitted with same symptoms. On the second episode, both PCR and stool culture indicated Campylobacter enteritis, and azithromycin treatment was resumed.
DISCUSSION
This study aims to bring clinical and laboratory feature about Campylobacter enteritis in children including patient cohort sizes larger than 100, first in Korea. We present result of our study of data totaling 123 Campylobacter enteritis cases retrospectively from 1,396 gastroenteritis patients. In this study, we aimed to identify the pathogen of enteritis by two flows. The first flow, EnterNet was only epidemiologic purpose, not intended for clinical care because the test results could be confirmed several weeks later. On the other hand, multiplex PCR, the second flow, was used to diagnose and treat the children immediately after receiving the stool specimen within one day. In the first flow, stool specimens were examined for both viral and bacterial etiology. Particularly during testing for bacterial pathogens, stool culture was performed first, followed by PCR in fecal specimens with positive results. Specimens with a negative final PCR despite a positive bacterial culture result were reported as negative. The prevalence of Campylobacter enteritis was 4.3% in EnterNet (Table 1). There was no comparable study of the proportion patients with Campylobacter enteritis in enteritis, it is difficult to determine whether the prevalence of Campylobacter enteritis was real. Because we stored stool samples at refrigerator temperature (4°C) and sent them only once a week to PHERI, we guess the sensitivity could be low. The male to female ratio of Campylobacter enteritis in children has been reported around 6:4,45) which is slightly different with the 5:5 ratio observed in the current study. According to previous study, two peaks in age distribution of Campylobacter enteritis were observed: in children (aged 1 to 4 years) and in young adolescents (aged 15 to 24 years).6) Interestingly, the second peak was not observed in Shigella or Salmonella enteritis and unique to Campylobacter enteritis.6) In the present study, it was difficult to identify the second peak because of age range difference from the previous study. And there was difference in culture by country and poultry consumption patterns. In this study, the highest incidence of Campylobacter enteritis in school-aged children and young adolescents was observed only once, different with the two peaks of the previous study. This result was common with age distribution of bacterial enteritis, which was contrasted with the highest incidence of viral enteritis in children aged under 5 years.
In China, Campylobacter enteritis peaks between late spring and summer and a lower second peak is observed in late autumn.4) Previous studies457) reported a disease peak between May and October, representing 95.0% of annually cases of Campylobacter enteritis. In the current study, a comparable peak was observed between May and October, accounting for 79.7% of cases with Campylobacter enteritis.
Campylobacter infection includes acute enteritis, sepsis, and extra-intestinal local infection. Campylobacter spp. is well recognized major cause of acute enteritis.8) After a latent period of 1 to 7 days, Campylobacter spp. induces periumbilical pain, diarrhea, or mucous and bloody stools. Nausea is a common manifestation across all ages, whereas vomiting frequently occurs at a younger age.9) Surgical abdomen, such as appendicitis or intussusception, is characterized by a similar presentation. Clinical symptoms were comparable to those in previous studies. Diarrhea, fever, and abdominal pain were observed in a majority of the younger patients. Other symptoms included headache, vomiting, and macroscopic hematochezia.
WBC levels over 10,000/mm3 were observed in 67 patients (57.3%), with 19 patients over 15,000/mm3 (16.2%). And few of the patients (58 cases, 47.2%) the CRP levels were significantly elevated (over 1.2 mg/dL). 10) Moreover, in 45 patients (36.6%), the CRP level was above 3.5 mg/dL,10) which represents screening points for bacterial infections. Kim et al.1) reported that CRP levels were higher in patients infected with Salmonella spp. or Campylobacter spp. than in those infected with S. aureus or pathogenic E. coli. Marked rise of CRP in Campylobacter infection was observed in the current study, and is consistent with the findings of previous reports.1)
In the majority of patients, imaging findings were diffuse edematous wall thickening of the colon and reactive mesenteric lymph nodes, indicative of enterocolitis. Yoon11) found that enteritis caused by Campylobacter spp. and Salmonella spp. involved edematous changes in the terminal ilium and proximal colon, which may include involvement of the whole colonic wall. Furthermore, according to the previous study,11) ultrasound findings include hypoechoic luminal wall thickening and increased Doppler blood flow to mucosa due to inflammation, which may be associated with large hypertrophic mesenteric lymph nodes. This finding is consistent with the results of abdominal enhanced CT and abdominal sonography in this study.
The first line therapy of Campylobacter enteritis is IV hydration and conservative management. Consistently with the previous research, this study showed that the early initiation of a 3-day-regimen of azithromycin could improve prognosis.1213) So, azithromycin use can be considered in pediatric patients with severe suspected Campylobacter enteritis. In this study, IV ceftriaxone was often prescribed as the antibiotic of choice in pediatric patients with high CRP levels because of the possibility of Salmonella-induced sepsis. However, Kim et al.1) reported that there were 22 cases (12%) of Salmonella infection of 183 diagnosed cases of bacterial enteritis, but no cases of Salmonella-induced sepsis were reported. Furthermore, the present study showed that the use of azithromycin was significantly associated with hospitalization within 3 days (P<0.05). Therefore, azithromycin can be considered as the first choice of antibiotics in pediatric patients with enteritis, with clinically severe symptoms and high CRP levels, in order to cover the possibility of infection with bacterial pathogen, such as Campylobacter spp. and Salmonella spp.
Recurrent infection was suspected in one patient. The first episode manifested as a 3-week history of continuous diarrhea and the patient was treated with azithromycin. The patient complained of on-going abdominal pain following the completion of the antibiotic regimen, although the pain subsequently decreased. Two months later, the patient was diagnosed with recurrent Campylobacter enteritis again, although with milder symptoms. Azithromycin was administered, which led to the resolution of symptoms with no complications. The incubation period of Campylobacterium is between 2 and 7 weeks in the feces of patients with Campylobacter enteritis in the absence of antibiotic administration. In this case, antibiotics were administered during the first infection. Second, Campylobacter was positive in stool culture and on PCR analysis after 9 weeks. In developing countries, recurrent infection has been reported in children, but it is rarely found in adults, who are considered to have been immunized through repeated infection.14) The recurrent infections in the 11-year-old boy in this study were also consistent with the findings of previous studies.
Food-borne infection, particularly due to undercooked meat, unpasteurized milk, and poultry, is the leading cause of Campylobacter enteritis.151617) Once infected, the host can contribute to the propagation of the pathogen for weeks to months. Furthermore, as neonates are vulnerable to all kinds of direct contact with infected sources, such as pets, meat products, or even diapers from daycare centers, careful history taking is crucial.18) Breast feeding is recommended in infants' owing to its protective effects.19) The 9-month-old patient in this study was fed with formula and delivered weaning food available in market.
The current study was a single institution study, and the study population does not represent the general Korean pediatric patients. However, the significance of this study lies in the fact that we analyzed more than 100 pediatric patients with Campylobacter and observed their clinical progress with accumulated data for 6 years. The complication and recurrence rates may be lower than those observed because of the follow-up losses, which frequently occur in retrospective studies. We reported several complications following Campylobacter infection and prospective cohort study may also be warranted in the future.
Selection bias could have affected the result as NEMC is the secondary hospital with an emergency department, which means that patients with more severe enteritis attend the hospital. So, treatment by using antibiotics had to be considered frequently in current study, allowing for the severity of the laboratory findings and symptoms such as fever, abdominal pain. Furthermore, it is not a standard practice to consider PCR routinely or in patients with milder symptoms.
Campylobacter spp. is a major cause of bacterial enteritis in pediatric patients. It commonly occurs in summer, and most often affects young adolescents. Clinical symptoms are of relatively severe and includes high fever, diarrhea, headache, and severe abdominal pain, with bloody stool. A thorough understanding of the clinical presentation of Campylobacter enteritis and early suspicion in pediatric patients may minimize unnecessary CT scanning and enable the appropriate initiation of an azithromycin regimen, potentially shortening the duration of symptoms and lowering the rate of complications. As the number of patients diagnosed with Campylobacter enteritis increases, future approaches are suggested to include a stool culture and antibiotic susceptibility testing of Campylobacter spp. that can help identify the infection source and to perform a prospective randomized controlled study that can compare antibiotic administration effects.
 XML Download
XML Download