

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Methods
Results
Conclusions
Figures and Tables
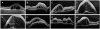 | Figure 1Optical coherence tomography images at baseline and Subretinal fluid height obtained from recurrent group. (A) Right eye of case 1. (B, C) Right and left eyes of case 2. (D, E) Right and left eyes of case 4. (F) Left eye of case 5. (G, H) Right and left eyes of case 9.
|
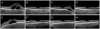 | Figure 2Optical coherence tomography (OCT) serial images obtained from case 1 of recurrent group. Left column (A–D) was OCT images of right eye, right column (E–H) was OCT images of left eye. (A, E) Serous retinal fluid (SRF) and choroidal thickening was observed at pretreatment state in both eyes. (B, F) SRF was subsided and choroidal thickness was decreased after high-dose intravenous steroid treatment. (C, G) SRF was recurred at perifoveal area during oral steroid tapering in right eye. The patient was treated with increased dose of oral steroid, oral immunosuppressant, and sub-tenon injection of triamcinolone. (D, H) SRF was completely absorbed after 24 weeks of steroid treatment.
|
 | Figure 3Optical coherence tomography (OCT) serial images obtained from case 8 of non-recurrent group. Left column (A–C) was OCT images of right eye, right column (E, F) was OCT images of left eye. (A, D) Serous retinal fluid (SRF) and choroidal thickening was observed at pretreatment state in both eyes. (B, E) SRF was subsided and choroidal thickness was decreased after high-dose intravenous steroid treatment. (C, F) OCT images after 24 weeks of high-dose intravenous steroid treatment. There was no recurrence during oral steroid tapering in both eye.
|
Table 1
Characteristics of 17 patients

‘Tapering Period’ means Duration of oral steroid tapering, ‘Initial Dose’ means Initial Oral steroid dose.
F/U = follow up period; BCVA = best corrected visual acuity; logMAR = logarithm of the minimal angle of resolution; AC = anterior chamber; OD = oculus dexter; OS = oculus sinister; SRF = serous retinal fluid; CSMT = central subfield macular thickness; Sx to Tx = symptom to treatment; Tx to Improve = duration until improvement after treatment; Recur = recurrence during oral steroid tapering; Tx to Recur = duration from treatment start to recurrence; STTA = sub-tenon triamcinolone injection; F = female; M = male; OU = oculus unitas; Tr = trace.
*Monocular patient.
![]()
Table 2
Characteristics in each group

Values are presented as mean ± standard deviation (median, range) unless otherwise indicated. ‘Group A’ means recurrence group during oral steroid tapering, ‘Group B’ means no recurrence group.
M/F = male/female; BCVA = best corrected visual acuity; logMAR = logarithm of the minimal angle of resolution; SRF = subretinal fluid; Sx to Tx = symptom to treatment; PD = prednisolone; IV = intravenous.
*The significance of the difference was assessed by the Mann-Whitney U test; †The significance of the difference was assessed by the Fisher's exact test.
![]()
 XML Download
XML Download