

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
We report two cases of intraocular lens (IOL) pupillary optic capture following IOL scleral fixation treated with argon laser iridotomy.
Case summary
(Case 1) A 69-year-old man presented with suddenly decreased visual acuity of the left eye. The best-corrected visual acuity was finger count (FC) 30 cm in the left eye. Slit lamp examination revealed subluxation of the left eye IOL. An IOL scleral fixation and anterior vitrectomy were performed and no specific findings were observed. During the follow-up period, pupillary optic capture was repeated without specific causes, such as trauma, or IOL decentration thus, argon laser iridotomy was performed. (Case 2) A 77-year-old man presented with a 3-day history of congestion of the left eye and decreased visual acuity. Best-corrected visual acuity was 0.4 logarithm of the minimum angle of resolution (logMAR) in the left eye. Slit lamp examination revealed subluxation of the left eye IOL. An IOL scleral fixation and anterior vitrectomy were performed, and no specific findings were observed. During the follow-up period, pupillary optic capture was found, and IOL repositioning and argon laser iridotomy were performed.
Figures and Tables
Figure 1
The anterior segment photos of 69 years old patient with a history of cataract surgery of both eyes. Color photographs shows intraocular lens dislocation (A), well-positioned intraocular lens after transscleral fixation (B), pupillary optic capture 2 months after transscleral fixation (C), repeated pupillary optic capture 5 months after transscleral fixation (D), and patent iridotomy site after argon laser iridotomy (E, yellow arrow).
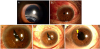
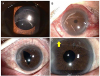
Figure 2
The anterior segment photos of 77 years old patient with a history of cataract surgery of both eyes. Color photographs shows intraocular lens dislocation (A), well-positioned intraocular lens after transscleral fixation (B), pupillary optic capture 2 months after transscleral fixation (C), and patent iridotomy site after argon laser iridotomy (D, yellow arrow).
References
1. Ridley H. Intra-ocular acrylic lenses--past, present and future. Trans Ophthalmol Soc U K. 1964; 84:5–14.

2. Malbran ES, Malbran E Jr, Negri I. Lens guide suture for transport and fixation in secondary IOL implantation after intracapsular extraction. Int Ophthalmol. 1986; 9:151–160.

3. Holt DG, Young J, Stagg B, Ambati BK. Anterior chamber intraocular lens, sutured posterior chamber intraocular lens, or glued intraocular lens: where do we stand? Curr Opin Ophthalmol. 2012; 23:62–67.

4. Hannush SB. Sutured posterior chamber intraocular lenses: indications and procedure. Curr Opin Ophthalmol. 2000; 11:233–240.
5. Fernández-Buenaga R, Alio JL, Pérez-Ardoy AL, et al. Late in-the-bag intraocular lens dislocation requiring explantation: risk factors and outcomes. Eye (Lond). 2013; 27:795–801. quiz 802.
6. Por YM, Lavin MJ. Techniques of intraocular lens suspension in the absence of capsular/zonular support. Surv Ophthalmol. 2005; 50:429–462.
7. Solomon K, Gussler JR, Gussler C, Van Meter WS. Incidence and management of complications of transsclerally sutured posterior chamber lenses. J Cataract Refract Surg. 1993; 19:488–493.
8. Teichmann KD, Teichmann IA. The torque and tilt gamble. J Cataract Refract Surg. 1997; 23:413–418.
9. McAllister AS, Hirst LW. Visual outcomes and complications of scleral-fixated posterior chamber intraocular lenses. J Cataract Refract Surg. 2011; 37:1263–1269.
10. Heilskov T, Joondeph BC, Olsen KR, Blankenship GW. Late endophthalmitis after transscleral fixation of a posterior chamber intraocular lens. Arch Ophthalmol. 1989; 107:1427.
11. Bading G, Hillenkamp J, Sachs HG, et al. Long-term safety and functional outcome of combined pars plana vitrectomy and scleral-fixated sutured posterior chamber lens implantation. Am J Ophthalmol. 2007; 144:371–377.
12. Johnston RL, Charteris DG, Horgan SE, Cooling RJ. Combined pars plana vitrectomy and sutured posterior chamber implant. Arch Ophthalmol. 2000; 118:905–910.
13. Davison JA. Capsule contraction syndrome. J Cataract Refract Surg. 1993; 19:582–589.
14. Moon AR, Moon NJ, Choi KY. Long-term results and complications using scleral-fixated posterior chamber intraocular lenses. J Korean Ophthalmol Soc. 1996; 37:1283–1292.
15. Herschler J. Trabecular damage due to blunt anterior segment injury and its relationship to traumatic glaucoma. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1977; 83:239–248.
16. Singh H, Safran SG, Ahmed II. Laser iridotomy for pseudophakic reverse pupillary block in patients with pupillary optic capture after sulcus-placed intraocular lenses. J Cataract Refract Surg. 2017; 43:299.
17. Narang P, Agarwal A. Pupilloplasty for pupil size attenuation to prevent pupillary capture: theory of quintet in glued IOL. J Cataract Refract Surg. 2017; 43:3–7.
 XML Download
XML Download