

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a rare inherited genetic disorder characterized by the replacement of the right ventricular (RV) myocardium with fibro-fatty layers, resulting in structural abnormalities, regional dyskinesia, ventricular arrhythmia and often sudden cardiac death.1)2) The diagnosis of ARVC is classified as definitive, borderline or possible, based on major and minor criteria which take into account structure, function, family history, histology, documented arrhythmia and electrocardiogram (ECG) abnormalities.3)4) Cardiac magnetic resonance (CMR) is considered one of the gold standard imaging modalities to detect RV dyskinetic segments, quantify RV volumes and ejection fraction (EF). In comparison to echocardiography, CMR is not limited by acoustic windows, can image the RV in any plane, and provides accurate and reproducible quantitative volumes and functional assessment, in addition to tissue characterization such as intramyocardial fat and myocardial fibrosis.5)
However, many patients with palpitation and arrhythmia have only focal dyskinetic segments with normal RV volume and/or EF. It is unclear whether these are non-specific findings, part of the spectrum of the disease, or precursor for ARVC detected early because of early screening.6) Their clinical implication and prognosis are also unknown.
Our study aims at assessing those patients with isolated focal RV dyskinesia, compare them to a control group and those who meet definitive criteria for ARVC, in a better attempt to characterize them.
METHODS
Study population
From the CMR database at Clemenceau Medical Center, Beirut, Lebanon, the charts of 65 consecutive patients who were imaged between July 2015 and September 2017 with clinical suspicion for ARVC, were extracted and reviewed for final analysis. Patients were referred because of clinical symptoms, family history of sudden cardiac death, suspicious ECG, high premature ventricular contraction burden, non-sustained or sustained ventricular tachycardia on 24 hours Holter, that meet some criteria for ARVC based on the 2010 revised Task Force criteria (TFC) (Table 1).4)
Table 1
Baseline characteristics stratified by presence or absence of RV dyskinetic segments by CMR
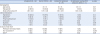
ARVC: arrhythmogenic right ventricular cardiomyopathy, CMR: cardiac magnetic resonance, ECG: electrocardiogram, RV: right ventricle, VT: ventricular tachycardia.
*dilated RV on echocardiography.
†Holter results were available for 51 patients (total) (26 with normal CMR, 21 with minor/indeterminate criteria, 4 with major criteria).
‡Other: epsilon wave, sinus tachycardia, supraventricular tachycardia, idioventricular rhythm and 2:1 AV block.
Data shown are number (%) not otherwise specified.
There were no patients with ischemic heart disease, dilated cardiomyopathy, congenital heart disease and/or insufficient axial or short axis cine images for exclusion. Demographics and indication of CMR testing were prospectively entered at the time of testing and were subsequently retrieved from the reports for analysis. The study was approved by the Institutional Review Board committee with waiver of consent and complied with the Declaration of Helsinki.
CMR imaging
CMR was performed on all patients with suspected diagnosis of ARVC, using 3.0 Tesla GE MR scanner (DiscoveryTM MR750w GEM 70 cm, Milwaukee, Wisconsin, USA). RV wall motion analysis was assessed using standard FIESTA cine sequences for axial, short-axis, 2, 3 and 4-chamber views (slice thickness 8.0 mm, TE minimum, flip angle 45°, bandwidth 125 Hz, NEX 1.0). The presence of fatty infiltration was assessed using T2 imaging with and without fat saturation (slice thickness 8.0 mm, TE 55 ms, auto refocus flip angle 107°, echo train length 25, blood suppression inversion time 648 ms, bandwidth 83.3 Hz, NEX 1.0). Delayed gadolinium enhancement analysis (slice thickness 8.0 mm, TE Min Full, flip angle 25°, inversion time 300-400 ms, bandwidth 41.7 Hz, NEX 1.0) was performed after intravenous injection of Omniscan's GE Healthcare Gadolinium-based contrast agent, administered with 40 mL saline flush at a dose of 0.15 mmol/kg.
Both axial and short axis images were used to assess for the presence of dyskinetic or aneurysmal segments. Quantitative analysis of RV volumes and EF was performed from the short axis cine stack images as recommended2)4) using GE workstation AW750w and the Cardiac VX software (cardiac analysis and reporting, software version 1.1.0, 2013, General Electric Company, Waukesha, Wisconsin, USA).
Major CMR criteria for ARVC were defined according to the 2010 revised TFC4) as: regional RV akinesia, dyskinesia or dyssynchronous contraction AND 1 of the following:
Minor criteria were defined as regional RV akinesia, dyskinesia or dyssynchronous contraction AND 1 of the following:
The quantitative analysis and wall motion interpretation were performed by a single level III trained and experienced reader, who de-identified and re-read all 65 studies, and was blinded at the time of the reading to the detailed clinical available data (i.e. family history, results of the Holters and ECG) and whether the referred patients met any major or minor non-imaging criteria that could bias his interpretation.
Patients were classified as having no RV dyskinetic segments, those with RV dyskinesia and meet major CMR criteria for ARVC, and those with isolated RV dyskinesia.
Statistical analysis
Continuous variables were expressed as means (standard deviation) and compared by use of the unpaired Student t-test, Wilcoxon rank test or ANOVA as appropriate. Categorical variables were expressed as frequency (percentages) and compared by use of the Fisher exact test, Pearson chi-square test, or Kruskal-Wallis as appropriate. All statistical tests were 2-sided. A p-value < 0.05 was set a priori and considered statistically significant. All statistical analyses were performed with the SPSS Statistics version 22 (IBM Corp., Armonk, NY, USA).
RESULTS
The cohort consisted of 65 patients (mean age of 43 ± 15 years, 67.6% of males) who were referred for CMR with a clinical suspicion for ARVC. The most common indications for CMR were palpitations, abnormal echocardiogram, presyncope/syncope, and abnormal 24 hours Holter monitoring (Table 1).
There were 5 patients (7.7%) that fulfilled a major CMR criterion for ARVC: 4/5 were classified as having definitive ARVC; and 1/5 as borderline (based on the available family history, ECG and/or Holter findings) (Table 1). There were 33 patients (50.8%) with no RV dyskinetic segments (4/33 had mildly dilated RV thought to be most likely athletic heart, and all with preserved EF): none were classified as having definitive or borderline ARVC; 4/33 were classified as possible ARVC (based on other non-imaging minor criteria); leaving 29/33 as normal or no ARVC (Tables 1 and 2). Finally, there were 27 remaining patients (41.5%) with isolated RV dyskinetic segments (almost a third had mildly dilated RV and 15% with mildly reduced RVEF): 1/27 was classified as definitive ARVC; 4/27 as borderline; 8/27 as possible; leaving 15/27 as indeterminate (Tables 1 and 2).
Table 2
RV characteristics by CMR
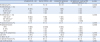
Compared to patients with no RV dyskinetic segments, those with isolated RV dyskinesia (and similarly the subgroup labelled as indeterminate 15/27) had larger RV end-diastolic volume index (82 ± 12 mL/m2 vs. 72 ± 12 mL/m2, p-value 0.0127), and a trend for higher odds of dilated RV (odds ratio 3.0 [0.81-11], p-value 0.09). No odds ratio could be calculated for RV EF since there were no abnormal EF in the control group.
DISCUSSION
The key findings of the study were: 1) almost 40% of patients referred for suspicion for ARVC had isolated dyskinetic RV segments; 2) of these 27 patients, 1, 4, and 8 were classified as having definitive, borderline or possible ARVC, respectively, while the majority remained unclassified; 3) this subgroup had more RV dilation and abnormal RV EF compared to the control group.
ARVC is a rare genetic disorder characterized by dyskinetic/aneurysmal RV walls, RV dilation and impaired systolic function, and is one of the leading causes of sudden cardiac death among athletes in the Mediterranean region (Figure 1).7)8) The prevalence of ARVC varies from 1:1000 to 1:5000.9)10) Despite its low prevalence, ARVC accounts for a disproportionately high percentage of referrals for CMR. The diagnosis relies on major and minor criteria which take into account structure, function, family history, histology, documented arrhythmia and ECG abnormalities. CMR is a reference standard imaging modality that allows visualization of all RV walls for global and regional RV function (axial and short axis views), quantifies EF, and differentiates ARVC from several mimickers of the disease.11)
Figure 1
Cardiac magnetic resonance (CMR) imaging of a 45-year-old male patient with family history of sudden cardiac death and ventricular tachycardia on Holter. CMR showed dilated right ventricle (RV) with end-diastolic volume index of 120 mL/m2, end-systolic volume index of 76 mL/m2, reduced RV ejection fraction at 37%, and several RV dyskinetic segments (white arrows), meeting major CMR criteria for arrhythmogenic right ventricular cardiomyopathy.

Non-pathological wall motion disorders are common; some are due to tethering of the free wall by the moderator band, and can easily be mistaken for pathological regional wall motion contraction, particularly with unexperienced or biased readers.12)13)14) Therefore, the presence of isolated RV dyskinesia should be accompanied by clinical and follow-up data to ascertain whether this is pathological finding and part of a spectrum of a progressive disease. While intramyocardial and RV free wall fat imaging is still performed, its role should be limited to avoid over calling.15)
The 2010 revised TFC for the diagnosis of ARVC became more stringent than those published in 1994, and resulted in reduction of total patients meeting any diagnostic CMR criteria for ARVC from 22.7% to 2.6%,16) and similarly in other studies.17)18) The reduced sensitivity however was counterbalanced by increased specificity,19) although a significant high proportion of patients has become unclassified, reaching almost a third in one study.6) Our study showed that almost 40% of patients had isolated RV dyskinesia and more than half of them remained unclassified (Figure 2). The new finding is that this cohort had higher RV end-diastolic volumes index and were more likely to have impaired RV systolic function compared to the control group. Similarly, in a prospective analysis by Hamid et al.20), relatives of patients with ARVC who had isolated minor criteria were found to have higher prevalence of electrocardiographic T wave inversion, positive signal averaged electrocardiography and non-sustained ventricular tachycardia, and hence classified as probable ARVC, giving more evidence to the fact that there is a spectrum for the disease and evolution of it. Still, there is presently no official consensus on serial imaging or clinical strategy for surveillance of patients with isolated RV dyskinesia.
Figure 2
Two patients with isolated focal right ventricular (RV) dyskinetic segments (white arrows) that remained unclassified. Panel A: 42-year-old female with frequent premature ventricular beats on Holter. Cardiac magnetic resonance (CMR) showed RV end-diastolic volume index of 87 mL/m2, end-systolic volume index of 44 mL/m2, and a calculated RV ejection fraction at 49%. Panel B: 50-year-old male with palpitations. CMR showed end-diastolic volume index of 105 mL/m2, end-systolic volume index of 61 mL/m2, and a calculated RV ejection fraction at 42%.

It has been well established that EF is not a very sensitive marker of impaired systolic function, at least not in the early stages. Indeed, in cardio-oncology, global longitudinal strain was shown to be a better indicator of early left ventricular systolic dysfunction than EF.21) It is reasonable to assume that many patients with isolated focal dyskinetic RV segments might have abnormal global longitudinal strain despite normal global RV EF, which could reclassify patients. Indeed, a recent study showed that strain analysis by feature-tracking CMR objectively quantified global and regional RV dysfunction and dyssynchrony in patients with ARVC, and provided incremental value over conventional cine CMR imaging.22) Hence, integrating abnormal RV strain as an add-on criterion for ARVC might reclassify patients, and increase the sensitivity of the test without compromising its specificity. This remains hypothesis-generating and should be evaluated in future studies.
Limitations
To the best of our knowledge, this is the first study to assess patients with clinical suspicion for ARVC and isolated RV dyskinesia from the Mediterranean region. However, we recognize several limitations. First, this is a retrospective single centre study with referral and selection bias. Second, the sample size is relatively small given that ARVC is a rare disease. Third, the study lacked echocardiographic and histological data, and only half of the patients had Holter results available for analysis; this would affect the final classification of patients as having definitive borderline, possible, or indeterminate ARVC. Fourth, clinical and imaging follow-up are lacking, which would have been of great interest particularly for those with isolated focal RV dyskinesia. There is an ongoing effort to follow-up these patients, repeat CMR imaging as well as ECGs and Holters in the following years, and gather clinical endpoints such as sudden cardiac death, syncope, and heart failure. In the absence of clinical endpoints, the relevance of isolated RV dyskinetic segments remains poorly understood. Fifth, RV wall motion was assessed by a single reader, with a lack of data on reproducibility, intra and inter-observer agreement. Finally, the potential differential and alternative diagnosis for isolated RV dyskinesia remains hypothetical in many of the cases in the absence of further clinical data.
Conclusion
Among patients with a clinical suspicion for ARVC, almost 40% had isolated focal dyskinetic RV segments with the majority remaining unclassified. This cohort had more RV dilation and abnormal EF compared to control. Integrating other imaging CMR data such as RV strain might prove useful in detecting subtle RV systolic impairment and could classify further patients. The clinical and prognostic implications of these findings need to be followed up prospectively in larger cohorts.
 XML Download
XML Download