

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Alzheimer's disease (AD) is the most common neurodegenerative disorder and is characterized by molecular pathogenesis, including amyloid plaques and neurofibrillary tangles in the brain. Several studies have suggested that amyloid-ß (Aß) and tau proteins in the cerebrospinal fluid (CSF) may act as reliable biomarkers of AD1,2 which can reflect the pathological process in the brain. Based on this knowledge, recently revised research criteria for AD have proposed these biomarkers as standards for diagnosis.3,4 Thus, the use of CSF biomarkers in clinical trials has been increased in both individuals with dementia and mild cognitive impairment, as well as in cognitively normal people of all ages. Moreover, with this increase comes a greater chance for individuals to receive lumbar punctures (LP) in memory clinics.
Although LP is classified as an invasive approach, many previous studies have demonstrated that it is a simple and safe procedure.5 The most common complication of LP is post-lumbar puncture headache (PLPH), the incidence of which has reportedly increased up to 50%.6 However, most studies about PLPH have analyzed LP in instances of spinal anesthesia,6,7 and not for outpatients. Moreover, no Korean study has evaluated whether the risk of PLPH after LP is increased in cognitively normal people or in individuals with AD.
In this study, we retrospectively analyzed the frequency of PLPH and its associated factors in a single-center study in Korea.
METHODS
We retrospectively collected data from patients with AD and cognitively normal people who were enrolled in a case-controlled study that was aimed to identify biomarkers of AD. The study was conducted at the Neurocognitive Behavior Center at Seoul National University Bundang Hospital in Korea between April 2012 and November 2014. The inclusion criteria for cognitively normal people were as follows: age of 50 to 90 years, satisfied normal aging criteria,8 normal cognitive status using the Mini-Mental State Examination (MMSE) and Seoul Verbal Learning test, and no brain lesion correlated with cognitive decline. The inclusion criteria for patients with AD were as follows: age of 50 to 90 years, satisfied the criteria set forth by the National Institute on Aging-Alzheimer's Association4 for probable AD, and no hemorrhagic lesion or other infarctions that could influence cognition. We excluded subjects who did not perform the LP due to fear. Moreover, subjects that had dropped out of the study prior to its completion or those that had other side effects were also excluded.
An interventional radiologist with expertise in the LP procedure carried out LP testing using fluoroscopy. All LPs were performed in the morning (8-12 a.m.) in the lateral decubitus position at the space between levels L3/L4 or L4/L5. LP was performed using either cutting-edge Quincke needles (20 gauge) or pen-point "atraumatic" Whitacre needles (20 or 22 gauge). Opening pressure was measured in all cases, and a total of 10-15 mL of CSF was collected by free flow of CSF. All subjects were advised to rest in the supine position for more than 2 h after the test and recommended to drink additional fluids, avoiding activity in the upright position.
Within 7 days after the procedure, subjects were contacted by telephone and were interviewed to assess whether they were experiencing any complications. Close attention was paid to reports of headache, and characteristics of the headache, as associated with criteria of PLPH,9 were recorded. Headaches were either classified as mild in intensity (needed simple analgesics or no treatment), moderate (needed to limit daily activity and stay in bed for several hours of the day), and severe (condition requiring hospitalization or were invalidating).10
To identify the association between PLPH and several variables including age, sex, clinical diagnosis, body mass index, opening pressure, needle type, and CSF Aß, we performed statistical analysis on the frequency of PLPH using the Mann-Whitney test for continuous variables and Fisher's exact test for categorical variables. To identify the association between PLPH and several variables, a multiple logistic regression analysis was performed. Variables with p values of <0.20 or whose association with PLPH were clinically relevant were considered for entrance into the model. These variables were then examined using a multiple logistic regression with backward stepwise method. All statistical analyses were performed using IBM SPSS Statistical software version 19.0 (IBM Inc., Armonk, NY, USA).
RESULTS
We identified 62 participants who were enrolled in the case-controlled study about on AD biomarkers. In total 3 (4.84% of 62) subjects were excluded because of LP refusal or dropout. Thus, we reviewed the remaining 59 subjects (patients with AD=28, cognitively normal subjects=31). Of the 59 cases, 29 (49.15%) satisfied the HIS criteria of PLPH.9 The severity of pain in PLPH was graded as more than moderate in most cases (mild=5, moderate=17, severe=7), and 2 subjects were treated by epidural blood patch. Table 1 summarizes the characteristic demographics between groups of subjects with and without PLPH. Interestingly, when compared to subjects without PLPH, subjects with PLPH tended to be younger and cognitively normal. Opening pressure and ratio of using cutting-edge needles also tended to be higher in subjects with PLPH. Body mass index and CSF Aß were not different between the two groups.
Table 2 shows the association between PLPH and related variables. In the multiple logistic regression analysis, several demographic variables and factors related to the LP procedure were included into Model 1. Among the demographic variables, older subjects were associated with a significantly lower incidence of PLPH [odds ratio (OR) 0.869 per year, p=0.003]. Clinical diagnosis was also found to correlate with PLPH incidence, and patients with AD were less likely to develop PLPH than cognitively normal individuals (OR 0.229, p=0.035). Regarding needle type, in Model 1 atraumatic needles did not influence the occurrence of PLPH when compared to cutting-edge needles. Likewise, the occurrence of PLPH was not influenced by sex or opening pressure (Table 2, Model 1). However, the backward stepwise logistic regression analysis showed that needle type did significantly correlate with PLPH (OR 0.165, p=0.014), and this was maintained with age and clinical diagnosis (Table 2, Model 2).
DISCUSSION
In a study aimed to identify AD biomarkers from CSF, we found an overall 49% incidence of PLPH in patients with AD and cognitively normal subjects. Among the variables that could increase an individual's risk for PLPH, we found that age, clinical diagnosis, and needle type were strong predictors of the occurrence of PLPH after LP.
Previous reports have suggested that the frequency of PLPH ranges between 20 to 50%.6,10 In contrast, other studies have reported considerably low frequencies of less than 2%.5,11 Discrepancies in the frequency of PLPH could be explained by differences in the populations examined and/or in the methodologies employed. For example, as demonstrated here and as reported by other studies, age and diagnosis could influence whether an individual develops PLPH, while different degrees of psychological factors might affect the frequency of headache.12 In terms of the LP method, it has been shown that needle type, needle size, and procedure technique might all be major factors in the development of PLPH.13,14
In the current study, younger, cognitively normal individuals receiving LP via cutting-edge needles were demonstrated as predictive factors of PLPH development. The effect of age and needle type on PLPH development has been reported previously.15,16,17 The lower incidence of PLPH in older individuals can be explained by the fact that pain sensitivity decreases with aging, and there is less leakage of CSF through narrower intervertebral foramina.11 Moreover, regarding the LP pro-cedure, elderly individuals tend to be less anxious.18 Peskind et al.5 measured the anxiety and pain scale by subject group, which included older normal subjects and patients with AD/mild cognitive impairment and then suggested that patients with AD/mild cognitive impairment tend to endure LP well with lower pain and anxiety. The other predictive factor, clinical diagnosis, shows discrepancy among reports.5,10,11,18 For example, cerebral atrophy and, consequently, larger CSF space, may explain the low frequency of PLPH in patients with dementia. However, additional study is needed to identify the influence of brain atrophy and concentration of CSF protein/cell count of patients with dementia.
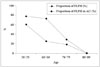
Although headache after lumbar puncture is usually a temporary symptom that lasts several days, it can result in patient discomfort. Furthermore, serious complications like seizure and subdural hematoma can arise from PLPH.19 Considering our result of the relatively high frequency of PLPH in up to 60% of young individuals (Fig. 1), more aggressive protocols that prevent PLPH are needed. We suggest that needle type is the key modifiable factor that will be able to ensure the safety, and thus maximize the acceptability, of LP in memory clinics. More specifically, the use of atraumatic needles could be useful because of their blunt tips and higher flexibility; however, clinicians performing LPs with atraumatic needles need to pay closer attention during procedures because it is often difficult to penetrate the skin and good handling technique is required.20
The current study had a number of limitations that should be addressed. First, the sample size in the current study was small. This was due to the characteristics of the base study design; future studies across a larger population are needed. Second, this was a retrospective review; thus, we did not control for conditions such as resting time after the procedure or total volume of CSF extracted. Moreover, we did not assess subjects' anxiety or stress before the LP was performed.
Despite these limitations, this is the first Korean report, to our knowledge, to evaluate PLPH risk factors by targeting patients with AD and cognitively normal people in a memory clinic. In such clinics, exposure to LP procedures will increase with the approval of CSF protein as an appropriate diagnostic test. Furthermore, the number of clinical trials on young subjects at pre-symptomatic stages may increase in the coming years. Here, we determined that PLPH was a relatively common complication of LP, especially in young, cognitively normal individuals that had undergone the procedure with a certain needle type. Based on these results, we advocate the use of an atraumatic needle for the prevention of PLPH; however, the difficulty of performing LPs with this needle type should be discussed in future studies.


 XML Download
XML Download