

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Alzheimer's disease (AD) is the most common form of neurodegenerative dementia, mainly characterized by progressive cognitive decline.1 Cholinesterase inhibitors (ChEI) are effective in AD treatment, however, clinical responses to ChEI th-erapy are variable. Some of patients improve cognitively or behaviorally in response to ChEI therapy while others deteriorate progressively.2 The heterogeneity of AD may be associated to the response to ChEI treatment. The short-term cognitive response to ChEI therapy is reported to be heterogeneous among individuals with AD. A better cognitive response to treatment was observed in patients with a fast disease progression rate before the treatment3 in patients who were more cognitively impaired,456 male,7 and patients taking larger doses of ChEIs;8 however, these results were inconclusive9 and long-term cognitive responses were not assessed.10
Recently, functional brain imaging using positron emission tomography (PET) and single photon emission computerized tomography (SPECT) may reflect heterogeneity within the AD population.11 While PET has a greater spatial resolution than SPECT, SPECT is a clinically simpler and more feasible technique. Therefore, a possible complementary strategy could be one of patient sub-grouping through a combination of functional and neuropsychological measures. The identification of subgroups that have a good response to ChEI therapy may provide valuable prognostic information to clinicians and social service providers, as well as increased knowledge regarding patient and family counseling concerning treatment effects. The aim of this study was 1) to find neuropsychological factor that influences the functional response to donepezil therapy, and 2) to determine whether regional cerebral blood flow (rCBF) pretreatment predicts a cognitive change in response to donepezil treatment.
METHODS
Patients
All new diagnoses of dementia resulting from probable AD were based on the National Institute of Neurological Communicative Diseases and Stroke-Alzheimer's Disease and Related Disorders Association criteria,12 with the additional requirement of a minimal severity based on the Korean version of Mini-Mental State Examination (K-MMSE)13 score. K-MMSE scores range between 14 points and 26 points, and a decreased cerebral perfusion compatible with AD in brain SPECT.
Among 37 patients, five patients dropped out after baseline assessment due to an incomplete evaluation at endpoint. We analyzed 32 patients in this study (20 females; 12 males). As a reference, none of them had a history of cerebrovascular events. All subjects were then examined by experienced neurologists and received a full clinical assessment which included standard dementia screening with K-MMSE,13 routine blood tests with CBC, biochemistry, the thyroid function test, chest X-ray, cranial CT and/or MR scanning to rule out cerebrovascular disease or other space occupying lesions. All the patients received a fixed dosage of donepezil (10 mg/day) following a 3-6 week induction period (5 mg/day) and tolerated medication without serious adverse effects. All participants or their guardians gave written informed consent before participating in the study, which was approved by the Institutional Review Board of Chonnam National University Hospital.
Neuropsychological tests and evaluation of cognitive impairment
Neuropsychological tests including the K-MMSE, Clinical Dementia Rating (CDR)14 and Seoul Neuropsychological Screening Battery15 including measures of attention, language and associated function, visuospatial function, memory and frontal executive function were performed for each patient upon each hospital visit. Among them, digit span (forward and backward), the Korean version of the Boston Naming Test (K-BNT), calculation, ideomotor praxis, the Rey-Osterrieth Complex Figure Test (RCFT) (copying, immediate and 20-min delayed recall and recognition), the Seoul Verbal Learning Test (SVLT: three learning-immediate recall trials of a 12 item list, a 20-min delayed recall trial for the 12 items), contrasting program test/go-no-go test, a test of semantic fluency and letter-phonemic fluency (the Controlled Oral Word Association Test, or COWAT), Stroop test (Color Word Stroop Test or CWST; correct number of responses for word reading and naming the color of the font for 112 items during a twomin period) were adopted for this study. Moreover, two behavioral scales were included in the battery: the Instrumental Activity of Daily Living16 and Alzheimer's Disease Co-operative Study-Activities of Daily Living (ADCS-ADL).17 A subgroup analysis of ADL was conducted with three subscales derived from 23 items in the ADCS-ADL scale.
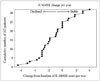
The severity and progression of cognitive impairment were assessed using the K-MMSE.13 The K-MMSEs of baseline and follow up evaluations were analyzed to calculate the annual K-MMSE change [(baseline-follow up K-MMSE score)/year]. The average annual change in K-MMSE score was -1.51±0.42 (mean1±SD). Doody et al.18 report that the mean annual MMSE score change in untreated AD patients is -3.71±4.6 (mean1±SD). Based on this data, we divided the subjects into s-AD and d-AD, where the cut-off value of annual K-MMSE score was less than 0.9 (Fig. 1).19
Brain SPECT imaging
Each patient underwent two Tc-99m ethylcysteinate dimer (ECD) brain SPECTs at baseline and endpoint evaluations for the cerebral perfusion assessment. The SPECT data was acquired using a dual-headed SMV DST-XLi gamma camera (GE Medical systems, Milwaukee, WI, USA) with a high-resolution collimator, setting the energy photo-peak at 140 keV, with a 20% symmetric window and an 180° acquisition arc. Imaging started 5 min after intravenous injection of 740 MBq (20 mCi) of Tc-99m ECD. The SPECT acquisition was undertaken in 32 steps (64 projections) and each collection step counts for 40 s. Reconstruction of the images was performed by filtered backprojection using a Butterworth filter. Matrix size and slice thickness of the SPECT images were 128×128 mm and 3.38 mm, respectively.
Image analysis and statistical analysis
SPECT data were analyzed using Statistical Parametric Mapping software (SPM, Wellcome Department of Imaging Neuroscience University College London, UK; http://www.fil.ion.ucl.ac.uk/spm/software/spm/). Prior to statistical analysis, datasets were spatially normalized and smoothed with an isotropic Gaussian kernel of FWHM 12 mm. Proportional scaling was used for global intensity normalization fitting to a linear statistical model. For global SPM analysis, applications returning p<0.001 were considered to be significantly different.
We compared differences in rCBF between the two subgroups at baseline and follow up using an independent sample t-test, and between the baseline and follow-up in each subgroup using paired t-test. For regional perfusion analysis, the spatially normalized and smoothed SPECT images of each subject were compared with a normative reference database generated from the SPECT scans of 12 elderly healthy volunteers (mean age 65±5.5). Each AD patient scan was compared with those from healthy controls for global activity using mean scaling procedures. Z scores [Z=(meansubject-meandatabase)/SDdatabase] were calculated, voxel by voxel, at a threshold of p≤0.01 (1-sided) corresponding to Z ≥2.33.202122 Z scores are reported in absolute values, and high Z scores are indicative of reduced blood perfusion in the scan of patients relative to the control mean.23 Z score maps obtained with this method were analyzed for regional blood perfusion deficits. Regional blood perfusion deficits, which are represented by the percentage of significant pixels of each anatomical area with the following equation [Activity (%)=(number of significant pixels/total number of pixels in a given anatomical area)×100], were measured using Functional and Anatomical Labeling of Brain Activation (FALBA) software.2425 FALBA software is used to identify and quantify the local sensitivity of brain perfusion deficits in each anatomical and/or functional area. One-hundred percent activity in an anatomical area indicates the highest sensitivity, whereas 0% activity indicates no sensitivity.
Those two groups were compared in age, sex, follow-up interval, education and initial K-MMSE scores. Statistical analysis was performed using SPSS statistics software (version 19.0, SPSS Inc., Chicago, IL, USA). An independent sample t-test was used to compare the two groups in terms of clinical characteristics. Statistical significance for these tests was set at p<0.05.
RESULTS
Demographic, clinical characteristics and neuropsychological assessment
The mean delay between the baseline and the follow-up neuropsychological tests were 14.91±3.87 months. The mean delay between the baseline brain SPECT and follow-up brain SPECT was 14.50±5.07 months. The mean delay between the baseline neuropsychological tests and baseline brain SPECT was 7.63±10.54 days (range -7 to 27). The mean delay between the follow-up neuropsychological tests and follow-up brain SPECT was 0.66±8.00 days (range -21 to 29).
Table 1 shows the demographic and general cognitive features of s-AD and d-AD groups based on their response to ChEI treatment at baseline and follow up. Fourteen (43.8%) of the 32 patients were categorized as s-AD, whereas 18 (56.2%) were d-AD. No significant differences in the two groups were found in terms of age, sex, education, apolipoprotein E e4 status or duration of treatment. At baseline, there were also no significant differences in K-MMSE, CDR, Global Deterioration Scales, Barthel Activities of Daily Living scores between two groups, however, the s-AD group showed significantly better ADCS-ADL functions (p=0.04) than the d-AD group (Table 1).
Table 2 shows the results of the neuropsychological tests in the two groups. At baseline, no significant differences in the two groups were found (p>0.05), however, the s-AD group presented higher performances on Go-no-Go (p=0.14), immediate SVLT (p=0.18), immediate RCFT (p=0.26), and K-BNT (p=0.26) than the d-AD group.
Brain SPECT
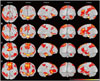
SPM analysis revealed that the baseline SPECT of enrolled patients showed lower perfusion than the elderly healthy volunteers used for comparison (FDR<0.005) (Fig. 2). At baseline (Fig. 2A) and follow up (Fig. 2B), the s-AD group showed decreased rCBF compared to normal controls. At baseline (Fig. 2C) and follow up (Fig. 2D), the d-AD group revealed the same pattern in the similar cerebrocortical regions, such as the superior frontal gyrus, supplementary motor area, inferior frontal gyrus, superior temporal gyrus, supramarginal gyrus, precuneus, inferior occipital gyrus, and rolandic operculum (Fig. 2).
In the group comparison using global SPM analysis, there was no statistical difference of rCBF at baseline and follow up between s-AD and d-AD groups. In the global SPM longitudinal analysis, there was no statistical difference of rCBF between baseline and follow up brain SPECT in each group (no figure). However, with regional blood perfusion analysis (FALBA software), the group comparison at baseline revealed a significantly higher perfusion deficit for the d-AD group in the supramarginal gyrus, inferior occipital gyrus, and rolandic operculum (Table 3).
DISCUSSION
We found that the higher preserved ADCS-ADLs predicted a better improvement in the MMSE scores in response to ChEI therapy. An increased positive functional response to ChEI was observed in Go-no-Go, immediate SVLT, immediate RCFT and short form K-BNT. So far, many studies have not examined the relationship of neuropsychological tests and response to ChEI therapy.
Wattmo et al.26 reported that better-preserved cognition and more impaired ADL ability implied an increased functional response to ChEI therapy. However, there were differences in baseline behavioral profiles in Physical Self-Maintenance Scale measurements. Responders have a better-preserved ADL ability at baseline, and these findings agreed with our results.
Prior work has reported that cognitive deficits are a risk factor for functional impairment among the elderly.27 Others demonstrate a weak linear association between cognition and ADL response, which agrees with our results that higher preserved ADL is associated with cognition improvement. An individual with well-preserved ADL take medication regularly and engage in a healthy lifestyle.
In addition, our study demonstrates that a more positive functional response to ChEI treatment was observed in individuals who had a high Go-no-Go score. Riekkinen et al.28 report that a severe frontal dysfunction, as shown both by neuropsychological tests and by SPECT, blocked the therapeutic effects of tacrine in a single-dose study. Our results support their findings, that frontal function is associated with response to ChEI treatment.
With global SPM analysis, rCBF levels in the brain SPECT did not appear to influence the effect of ChEI therapy on cognitive function as assessed by MMSE. However, with regional perfusion analysis (FALBA software), perfusion defects in the supramarginal gyrus, inferior occipital gyrus, and rolandic operculum can predict poor response to ChEI therapy or rapid progression of AD.
Previous neuroimaging studies, including SPECT, show that the response to donepezil treatment in AD patients have produced inconsistent results. Hanyu et al.29 report that ChEI therapy responders had higher baseline rCBF values throughout extensive brain areas, including the lateral and medial frontal lobes, relative to non-responders, even though the duration of treatment was only 15 weeks.
There may be differences between a short-term and long-term response after ChEI treatment. In contrast, Mega et al.30 report that ChEI therapy responders had a lower baseline rCBF in the lateral orbital frontal and dorsolateral frontal lobes than non-responders, and their data support that a neural effect of the frontal lobe is not involved in cognitive but in behavioral responders to donepezil treatment in AD patients. In our study, global SPM analysis showed no differences in rCBF between the two subgroups at baseline and follow-up, and between the baseline and follow-up in each subgroup. Our results agree with the findings of Shimizu et al.19 showing no significant differences in baseline rCBF in any region of the brain between the stable and declined subgroups, but did not agree with their results showing significantly lower rCBF at follow up brain SPECT of patients with the declined subgroup in the lateral and medial frontal lobes, limbic lobe, lower lateral temporal lobe, and cingulate gyrus than the stable subgroup.
Instead of global SPM analysis, our study analyzed regional blood perfusion (FALBA software) and observed that the d-AD group had a lower baseline rCBF in the supramarginal gyrus, inferior occipital gyrus, and rolandic operculum than the s-AD group. Our regional analysis findings agree with the results of Hanyu et al.29 showing high rCBF in ChEI therapy responders. Our results also support the findings of Shimizu et al.19 that low rCBF at follow up brain SPECT in the declined subgroup compared with the stable subgroup. The rCBF measurements with brain SPECT have the advantage of showing effects due to the actual degeneration of specific brain regions, together with neuronal dysfunction on brain systems. However, this advantage turns into a limitation if one wants to identify a causal relationship between regional effects and the response to the therapy, as it is impossible to distinguish rCBF decreases between the two groups diagnosed AD already using global SPM analysis.
There are several limitations in this study. First, the number of subjects was small. Second, we were unable to create a control AD group that did not take a ChEI medication. Thus, we do not know how spontaneous progress of AD affected the change of rCBF, nor do we know the effect of donepezil on the blood perfusion in healthy subjects after a 1-year treatment. Third, we measured clinical outcomes using the K-MMSE. Although K-MMSE has the advantages of being both easy to administer and is not time-consuming, however, this test was not designed to assess subtle changes in cognition.31
In conclusion, we found that the higher ADCS-ADLs predicted a better improvement in the K-MMSE scores in response to ChEI therapy and a more positive functional response in the group with preserved frontal function. Furthermore, the regional perfusion analysis of brain SPECT, instead of global SPM analysis, provided hints to the variable response to the therapy with ChEI treatment.



 XML Download
XML Download